
[box type=”bio”] Learning Point of the Article: [/box]
GCT of bone is locally aggressive in nature and is associated with high incidence of recurrence. Majority of recurrences occur within the first 2 years, late recurrences are known and long-term surveillance is recommended in these patients. Total serum acid phosphatase (TACP) could be used as a tumor marker for monitoring response to the treatment of GCT. Measuring TACP levels at follow-up would likely diagnose recurrence; early and prompt treatment with better results could be obtained.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 62-65 | Rajat Kapoor, Chandra Prakash Pal, Karuna Shankar Dinkar, Yajuvendra Kumar Sharma. DOI: 10.13107/jocr.2020.v10.i02.1698
Authors: Rajat Kapoor[1], Chandra Prakash Pal[1], Karuna Shankar Dinkar[1], Yajuvendra Kumar Sharma[1]
[1]Department of Orthopaedic Surgery, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
Address of Correspondence:
Dr. Rajat Kapoor,
Department of Orthopaedic Surgery, Sarojini Naidu Medical College, Agra, Uttar Pradesh, India.
E-mail: rajatsarvkapoor@gmail.com
Abstract
Introduction: Giant cell tumor (GCT) at Distal End Radius (DER) have relatively aggressive nature and higher recurrence rate and malignant transformation than their other counterparts. There is no case reported till now of GCT recurrence in grafted fibula used for reconstruction in managing primary DER-GCT. The purpose of the study is to report the recurrence of GCTin fibular graft used for treatment in primary GCT of DER.
Case Report: A 40-year-old female was diagnosed with Campanacci Type 3 GCT-DER 7-year back. The patient was operated and treated by excision of tumor and reconstruction with contralateral fibular grafting with K-wire fixation of DER7-year back and biopsy of growth was sent. After 7 years, the patient again developed swelling over the right wrist and radiological diagnosis of GCT Campanacci Grade 3 is made. She is managed by resection of tumor tissue by volar approach to DER with proximal row carpectomy with ulnocarpal fusion with retrograde K-wire fixation of the 3rd metacarpal resulting in centralization of ulna.
Conclusion: Recurrence in GCT also occurs at donor fibula used in reconstruction for primary treatment and could be safely managed by wide excision and centralization of ulna with good results.
Keywords: Giant cell tumor, distal end radius, fibula graft, recurrence.
Introduction
Distal end radius (DER) and giant cell tumor (GCT)have relatively aggressive nature and higher recurrence rate and malignant transformation than their other counterparts. There is no case reported till now of GCT recurrence in grafted fibula used for reconstruction in managing primary DER-GCT. The purpose of the study is to report the recurrence of GCT in fibular graft used for treatment in primary GCT of DER.
Case Report
A 40-year-old female presented to us with complaint of pain and swelling at the right wrist from the past 3 months with inability to carry out her daily routine activities. Pain was dull aching in nature, non radiating, aggravated with wrist movements, and relieved with rest. Swelling gradually increased in size. On examination, swelling was present over DER, had normal temperature overlying swelling compared to surrounding skin, no crepitus, tenderness present, and movements were painful.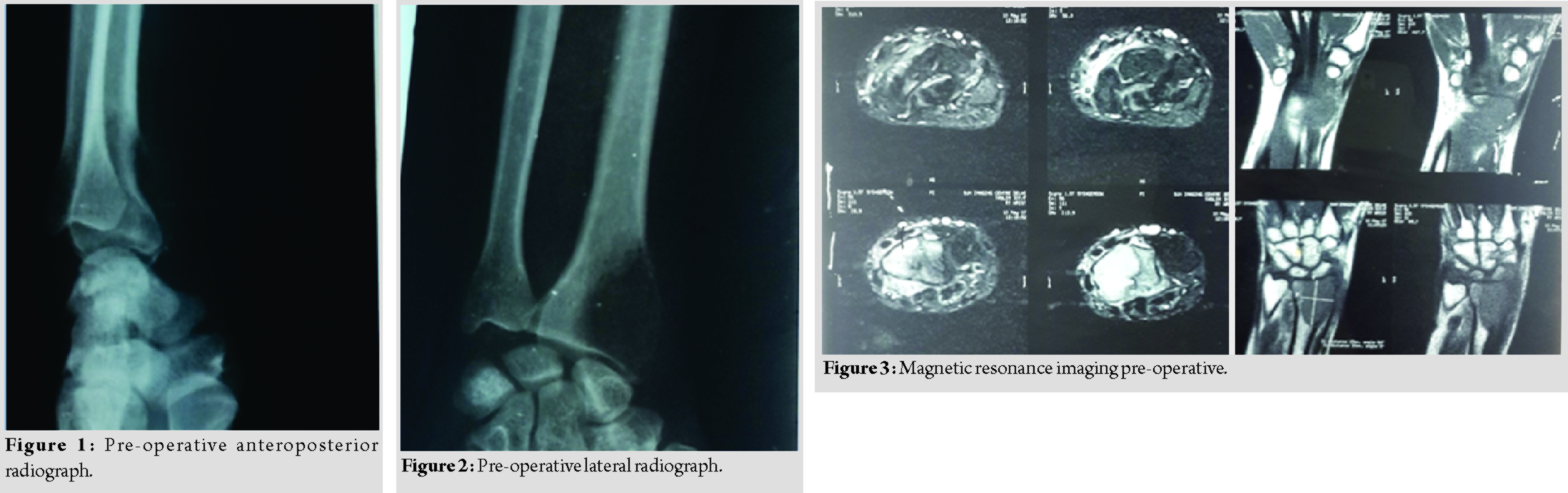
Pre-operative anteroposterior (AP) (Fig. 1) and lateral radiograph (Fig. 2) of the wrist were done which revealed an expanded osteolytic lesion at the epiphyseal region of the distal radius. Magnetic resonance imaging (MRI) (Fig. 3) and fine-needle aspiration cytology were done and GCT was diagnosed Campanacci Type 3. The patient was operated and treated by excision of tumor and reconstruction with contralateral fibular grafting with K-wire fixation of DER and biopsy of growth was sent. Above elbow slab was applied (Fig. 4 and 5).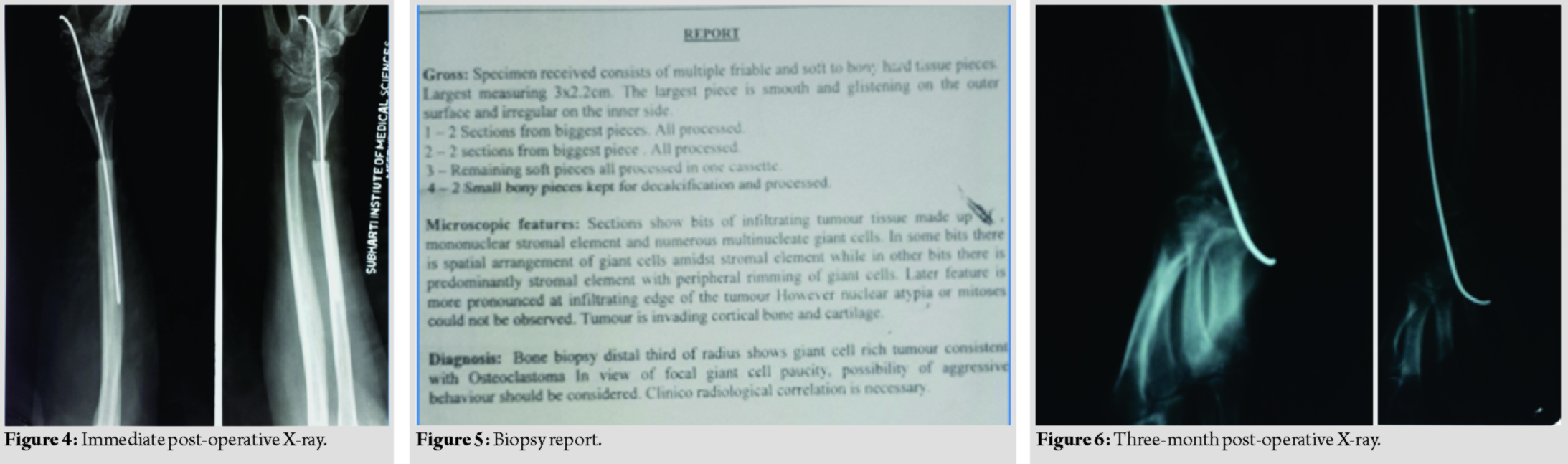
The patient came for regular follow-up at the 1st, 2nd, and 3rd months. Union was confirmed at the 3rd month (Fig. 6) and slab was removed and K-wire removed at 9 months (Fig. 7). The patient was further followed at 3 months interval for the next 18 months with no complaints with the functional score of 21 done using the musculoskeletal tumor society system[1].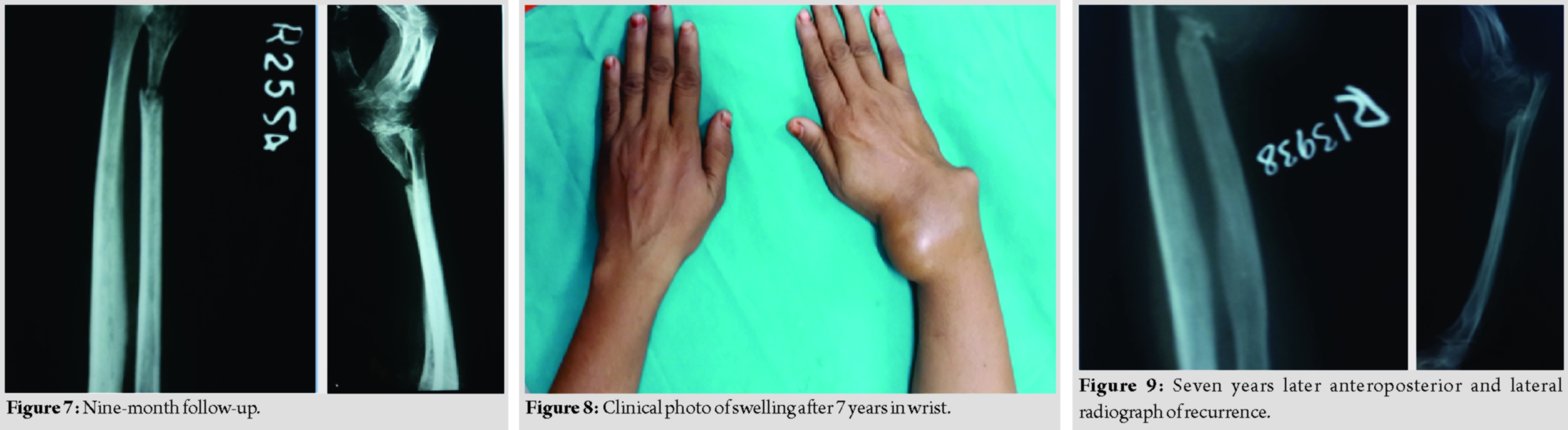
After 7 years, the patient again turned with a swelling at the same region, which is also gradually increasing in size for the past 3 months (Fig. 8) and was able to do daily routine household activities. X-ray AP and lateral views (Fig. 9) of wrist showed gross lytic expansion of the fibular graft with lytic lesions of the multiple proximal carpal bones. MRI of wrist(Fig. 10)shows expansile lytic lesion, with corticomedullary destruction. A radiological diagnosis of GCT Campanacci Grade 3 was made. Bone scan (Fig. 11) was done to rule out any metastasis and showed abnormal increased uptake seen in radiotherapy. She subsequently was managed by resection of tumor tissue by volar approach to DER with proximal row carpectomy with ulnocarpal fusion with retrograde K-wire fixation of the 3rd metacarpal resulting in centralization of ulna. Wound is closed without tension and above elbow pop slab is applied. Above elbow pop slab is applied for 12 weeks. Physiotherapy is commenced immediately after the surgery, starting with finger movements. Wrist physiotherapy is commenced at 12-week post-surgery after confirming union.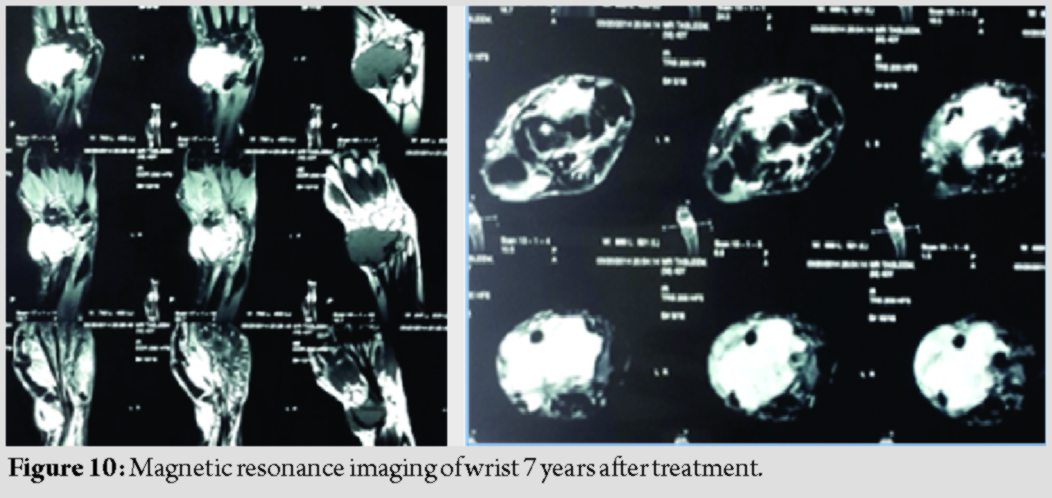
Biopsy sample sent which confirmed the diagnosis of GCT of the distal radius. (Fig. 12) depicts hematoxylin and eosin staining of the sample smear showing features of GCT of bone with osteoclastic type of giant cells, and multinucleate cells interspersed in proliferating stromal cells(Figs. 13 and14).The patient developed necrosis which healed on regular dressing.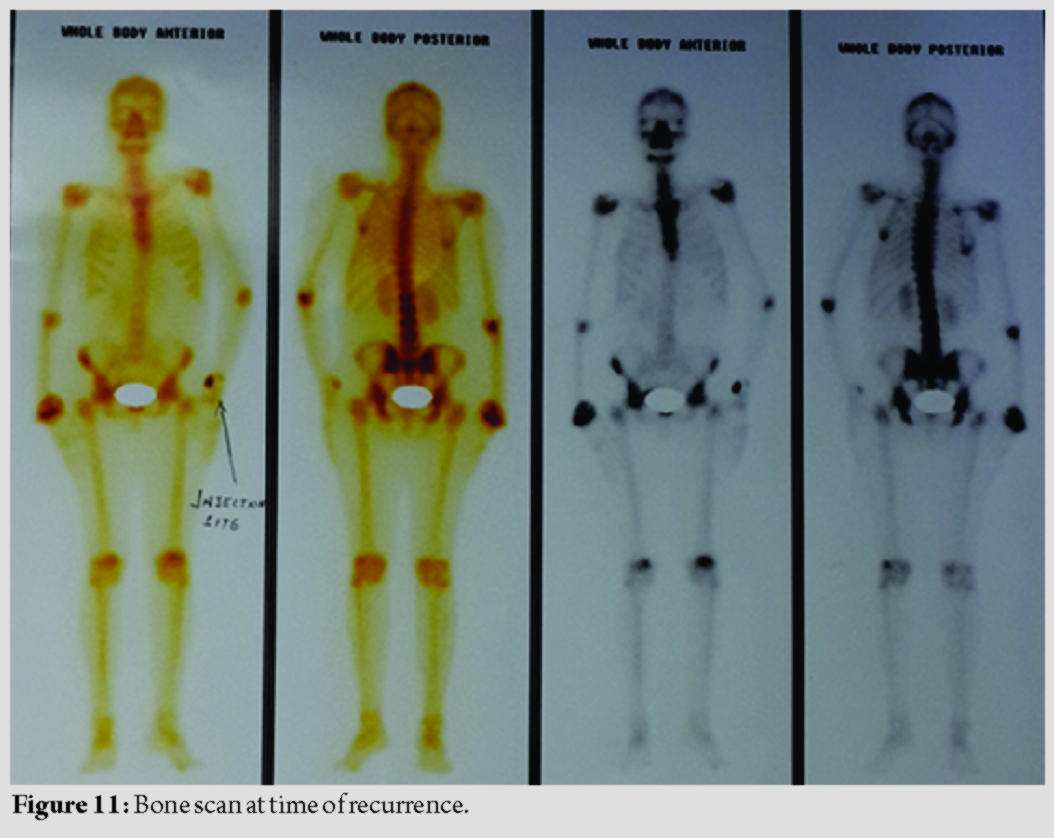
No recurrence noted till the last follow-up and the patient functional score was 15 done using them usculoskeletal tumor society system.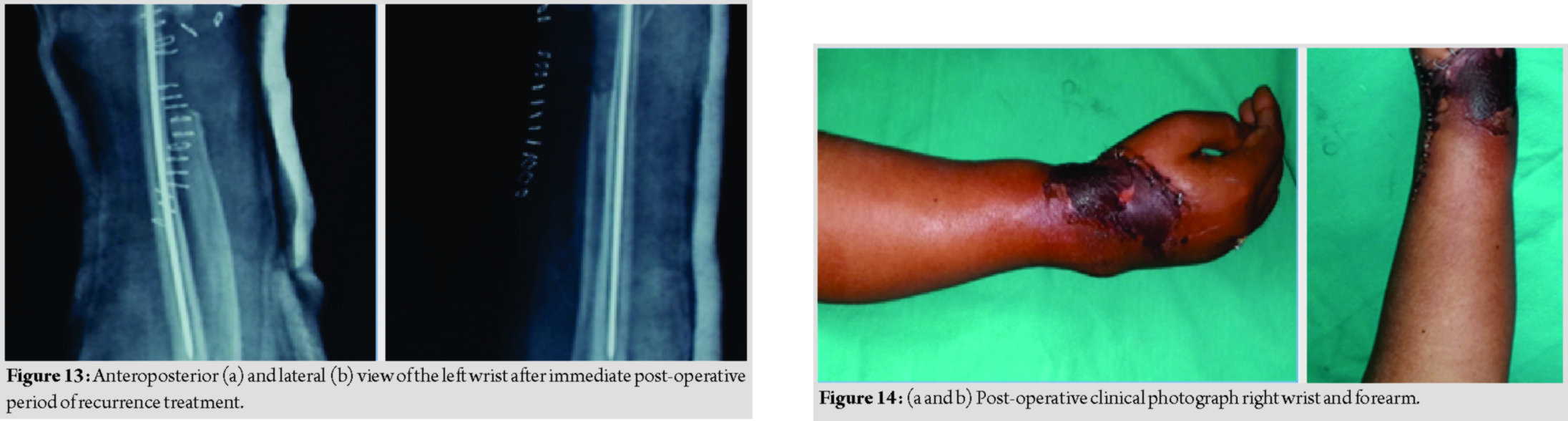
Discussion
GCT of bone is locally aggressive in nature and is associated with high incidence of recurrence [2, 3]. Selection of proper treatment is complicated due to the failure of its histologic appearance to indicate its biology [4, 5]. The goal of treatment is to remove the tumor, decreasing the chances of recurrence [6], and preserve the joint function. Among different modalities of treatment available, simple curettage of giant cell tumor is associated with 5–15% rate of local [7], osteonecrosis with liquid nitrogen is associated with high risk of fracture. Intralesional curettage with packing of the defect with methylmethacrylate (bone cement) has become popular [8]. The free radicals and the thermal effects of the polymerization reaction can cause necrosis as much as 2 or 3 mms in the cancellous bone, with lack of donorsite morbidity, and elimination of the risk of transmission of disease associated with the use of allograft bone, immediate structural stability, and potential for earlier detection of local recurrence. This patient having Campanacci Grade 3 tumor recurred in the grafted fibula. This lesion is not amenable to curettage and adjuvant therapy. Hence, only option left is wide excision including carpals (scaphoid, lunate, trapezoid, and capitate) with reconstruction of the joint. The patient refused for fibular grafting, so wide excision with centralization of ulna[1, 13, 14, 15, 16, 17] was done.
Conclusion
Majority of recurrences occur within the first 2 years, late recurrences are known and long-term surveillance is recommended in these patients as quoted by Scully et al.(1994) and Laurin et al. (1980). A recent study by Akhaneet al. (2005) suggests that total serum acid phosphatase (TACP) could be used as a tumor marker for monitoring response to the treatment of GCT. The high pre-operative TACP values in GCT patients became normalized after surgery but reappeared in recurrence. Measuring TACP levels at follow-up would likely diagnose recurrence; early and prompt treatment with better results could be obtained.
Clinical Message
Recurrence in GCT also occurs at donor fibula used in reconstruction for primary treatment and could be safely managed by wide excision and centralization of ulna with good results.
References
1. EnnekingWF, DunhamW, GebhardtMC, MalawarM, PritchardDJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system.Clin OrthopRelat Res1993;286:241-6.
2. SungHW, KuoDP, ShuWP, ChaiYB, LiuCC, LiSM. Giant-cell tumor of bone: Analysis of two hundred and eight cases in Chinese patients.J Bone Joint Surg Am1982;64:755-61.
3. DahlinDC, CuppsRE, JohnsonEW Jr. Giant-cell tumor: A study of 195 cases.Cancer1970;25:1061-70.
4. GoldenbergRR, CampbellCJ, BonfiglioM. Giant-cell tumor of bone. An analysis of two hundred and eighteen cases.J Bone Joint Surg Am1970;52:619-64.
5. SzendröiM. Giant-cell tumour of bone.J Bone Joint Surg Br2004;86:5-12.
6. HarrisWR, LehmannEC. Recurrent giant-cell tumour after en bloc excision of the distal radius and fibular autograft replacement.J Bone Joint Surg Br1983;65:618-20.
7. O’DonnellRJ, SpringfieldDS, MotwaniHK, ReadyJE, GebhardtMC, MankinHJ. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement.J Bone Joint Surg Am1994;76:1827-33.
8. GitelisS, MallinBA, PiaseckiP, TurnerF. Intralesional excision compared with en bloc resection for giant-cell tumors of bone.J Bone Joint Surg Am1993;75:1648-55.
9. LinN, YeZM, LiWX, TaoHM, YangDS. Long-term result of fibula grafting for reconstruction of the distal radius after giant cell tumor excision.Zhonghua Wai Ke Za Zhi2009;47:1079-82.
10. IharaK, DoiK, SakaiK, YamamotoM, KanchikuT, KawaiS. Vascularized fibular graft after excision of giant cell tumor of the distal radius. A case report.Clin OrthopRelat Res1999;359:189-96.
11. Lackman RD, McDonald DJ, Beckenbaugh RD, Sim FH. Fibular reconstruction for giant cell tumor of the distal radius. Clin OrthopRelat Res 1987;218:232-8.
12. Murray JA, Schlafly B. Giant-cell tumors in the distal end of the radius. Treatment by resection and fibular autograft interpositional arthrodesis. J Bone Joint Surg Am 1986;68:687-94.
13. BhagatS, BansalM, JandhyalaR, SharmaH, AminP, PanditJP. Wide excision and ulno-carpal arthrodesis for primary aggressive and recurrent giant cell tumours.Int Orthop2008;32:741-5.
14. SeradgeH. Distal ulnar translocation in the treatment of giant-cell tumors of the distal end of the radius.J Bone Joint Surg Am1982;64:67-73.
15. PuriA, GuliaA, AgarwalMG, ReddyK. Ulnar translocation after excision of a CampanacciGrade-3 giant-cell tumour of the distal radius: An effective method of reconstruction.J Bone Joint Surg Br2010;92:875-9.
16. Walthar M. Resection de extremiteinferieure du radius pour osteosarcoma geffe de I extremitesuperiuete du perone. Sac Chir Par Bull Mem 1911;37:739-47.
17. SmithRJ, MankinHJ. Allograft replacement of distal radius for giant cell tumor.J Hand Surg Am1977;2:299-308.
 |
 |
 |
 |
| Dr. Rajat Kapoor | Dr. Chandra Prakash Pal | Dr. Karuna Shankar Dinkar | Dr. Yajuvendra Kumar Sharma |
| How to Cite This Article: Kapoor R, Pal CP, Dinkar KS, Sharma YK. Recurrence of Giant Cell Tumor in Fibular Graft Used for Treatment in Primary Giant Cell Tumor of Distal End Radius: A Case Report and Surgical Treatment with Excision of Tumor with Proximal Row Carpectomy with Ulnocarpal Fusion. Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 62-65. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


