
[box type=”bio”] Learning Point of the Article: [/box]
Posterolateral tibia osteochondral fracture is a rare injury and a high index of suspicion in needed for associated tears of the ACL, MCL and lateral meniscus posterior root.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 36-42 | Anshu Shekhar, Ankur Singh, Amit Laturkar, Sachin Tapasvi. DOI: 10.13107/jocr.2020.v10.i03.1738
Authors: Anshu Shekhar[1], Ankur Singh[1], Amit Laturkar[1], Sachin Tapasvi[1]
[1]The Orthopaedic Speciality Clinic, Pune, Maharashtra, India.
Address of Correspondence:
Dr. Anshu Shekhar,
The Orthopaedic Speciality Clinic, 16, Status Chambers, Wrangler Paranjpe Lane, Off FC Road, Pune, Maharashtra, India.
E-mail: dr.anshushekhar@gmail.com
Abstract
Introduction: Injuries to the knee ligaments, menisci, and cartilage are possible in high-velocity trauma as in road traffic accidents. Similarly, these structures can be disrupted in proximal tibia fractures. We present a series of three cases which had a previously undescribed injury combination.
Case Presentation: The first and second patients presented primarily to us following fall from motorbikes. Both these patients had injuries of the anterior cruciate ligament (ACL), medial collateral ligament (MCL), lateral meniscus body and posterior root tear, and osteochondral fracture of posterolateral tibia. The osteochondral fracture was managed by internal fixation with headless compression screws. The ligaments were either repaired or reconstructed and meniscus root tear was treated by transtibial pull through repair. The third patient also had the same injury but was treated at another center. He presented with early arthritis of the lateral tibiofemoral joint and valgus malalignment. Treatment for him was in the form of lateral distal femur open-wedge osteotomy and MCL reconstruction. All three patients had good outcome at the end of 1year.
Conclusion: We report a new injury tetrad of ACL tear, MCL tear, lateral meniscus posterior root tear, and posterolateral tibia osteochondral fracture. The mechanism of injury is most likely a violent external rotation and anterior translation of the tibia with a valgus directed force during impact. The treatment of this injury can be performed in single or two stages based on the merits of the case. Anatomic reduction and fixation of the fracture takes precedence to avoid later devastating sequel for the knee.
Keywords: Knee, fractures, cartilage, anterior cruciate ligament injuries, medial collateral ligament, tibial meniscus injuries, traffic accidents.
Introduction
The anterior cruciate ligament (ACL) is a frequently injured ligament and can present in combination with other ligament, cartilage, or meniscal tears [1]. Sports injuries and road traffic accidents are the common modes of such injuries. Lateral meniscus posterior root tears are reported to occur in 6.6% of ACL tears [2]. Concomitant Grade 3 tears of medial collateral ligament (MCL) in the presence of ACL tears are found in just about 1% of patients [3]. Fractures of the tibial condyle, on the other hand, are associated with more violent trauma. An axial plane fracture of the posterolateral tibia is not even included in standard classification systems [4]. When more than two major knee ligaments are injured, it is defined as a multiligament knee injury (MLKI). A MLKI is often termed as a knee dislocation interchangeably and this has been reported to constitute <0.02% of all musculoskeletal injuries [5,6].As per the classification of Schenck, the presence of a fracture along with injury to two or more ligaments is classified as KD V [7]. Due to the heterogeneous injury combinations and rarity of this injury, there is insufficient literature in this regard and no universally accepted guidelines or method of treatment. We came across three patients over a period of 1 year, who had an injury combination of ACL tear with MCL tear with lateral meniscus posterior root tear extending into the meniscus body with posterolateral tibia osteochondral fracture. This is a report of this hitherto undescribed injury tetrad and its management.
Case Report
History, examination, and investigations
Case 1
A 19-year-old boy having body mass index (BMI) of 18.4 kg/m2 presented to the emergency room (ER) with a history of fall from motorbike, sustaining trauma to the right knee. A recall of the exact mechanism of fall was not possible, but he did report that the bike fell on the inner aspect of his knee which was partially flexed. The knee had Grade 3 effusion, range of motion was painful with inability to bear weight on the right leg. The Lachman test was Grade 2 while valgus stress test was painful. Plain radiograph revealed a bony fragment in the Hoffa’s fat pad in the lateral view and a linear transverse crack in the lateral tibial condyle (LTC). A CT scan revealed an osseous piece originating from the articular area of the LTC displaced anteriorly. Magnetic resonance imaging (MRI) scan revealed cartilage component of the “osseous” fragment with an ACL and lateral meniscus posterior root tear and partial injury to the femoral attachment of MCL (Fig. 1).

Case 2
A 43-year-old gentleman with BMI of 28.6 kg/m2 presented in the ER with a history of fall from a motorbike 2 days prior. He attempted to break his fall, but the bike swerved while his foot was planted on the ground. There was Grade 3 effusion in the knee and he was unable to bear weight on his right leg. There was Grade 3 valgus laxity and a Grade 3 Lachman test on examination. Plain radiograph revealed a bony fragment lying in the patellofemoral space anteriorly on lateral view. MRI scan showed an osteochondral injury of the LTC with complete femoral-sided rupture of the MCL, femoral avulsion of the ACL, and tear of the lateral meniscus posteriorly (Fig. 2).

Case 3
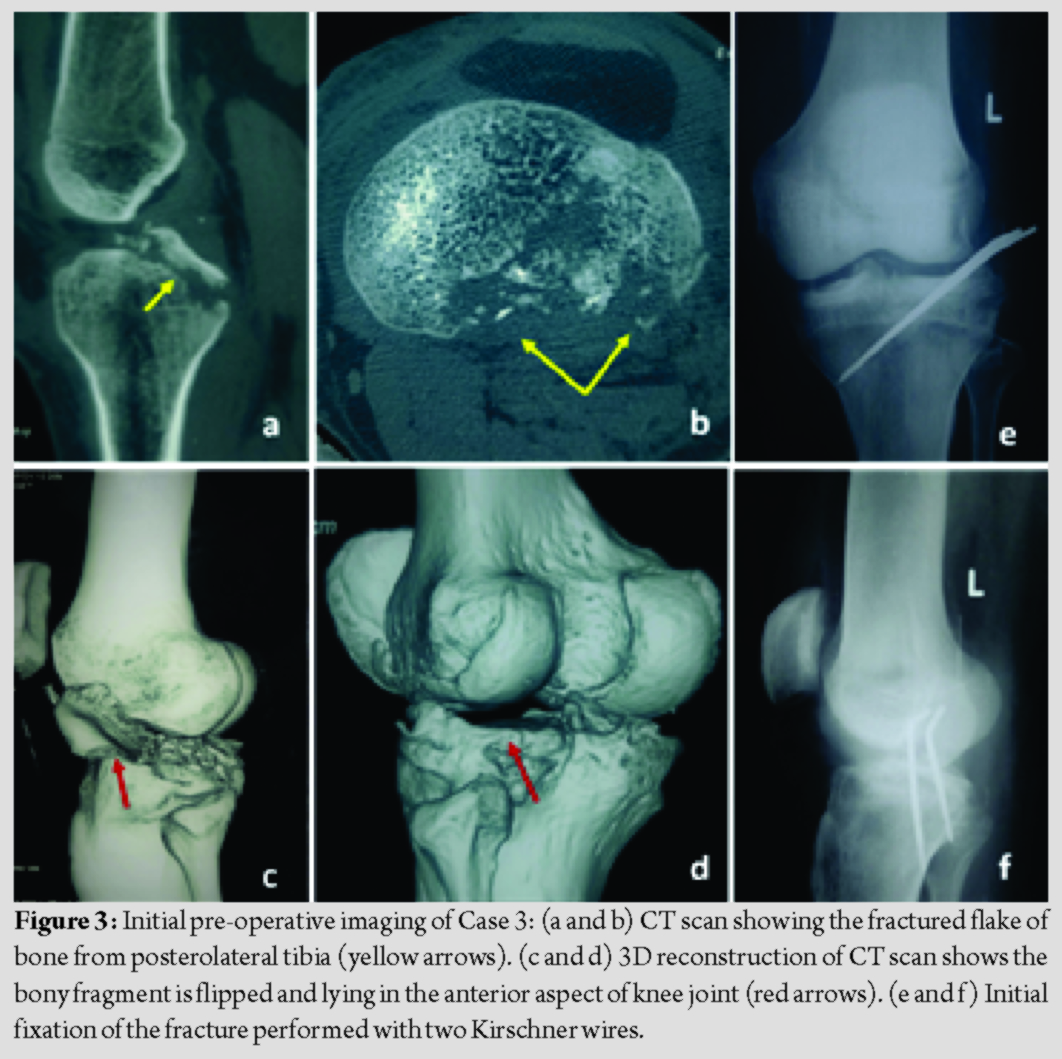
A 27-year-old man BMI of 22.7 kg/m2 came to the clinic with complaints of pain and instability of his left knee. He had a history of fall from motorbike 14 months prior and was diagnosed with fracture of the LTC. Review of his injury investigations showed that he had an osteochondral fracture of the posterolateral tibia as seen of plain radiographs and CT scan. Open reduction and fixation of the fracture with two K-wires was performed through a posterolateral approach (Fig. 3). On examination, there was valgus alignment and he walked with an antalgic gait and valgus thrust. Tenderness was present posterolaterally, range of motion was 0–120° with Grade 3 valgus laxity and Lachman test Grade 3.
Management
Case 1
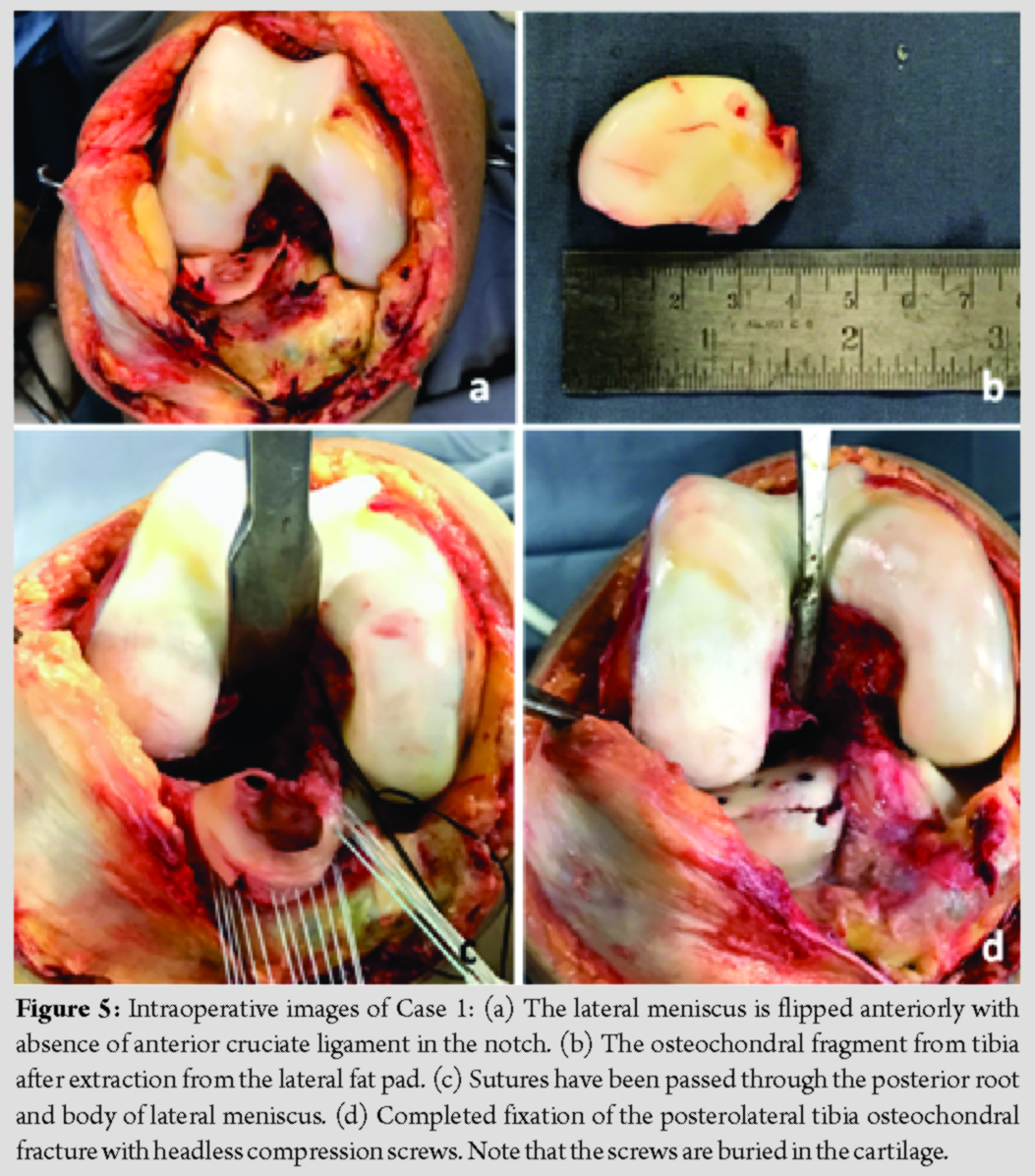
The patient was counseled for surgery, which was performed under neuraxial anesthesia. The knee was approached through a medial parapatellar arthrotomy. The osteochondral fragment from posterolateral tibia was entrapped in the fat pad, ACL was torn in the mid-substance and lateral meniscus flipped anteriorly, having avulsed from the posterior root. The fractured fragment was replaced in its native location based on the orientation of fracture lines. Fixation of this fragment was performed with four 2.4 mm headless compression screws (DePuy Synthes). The screw lengths were measured and care was taken to bury all the screws in the cartilage (Fig. 4).
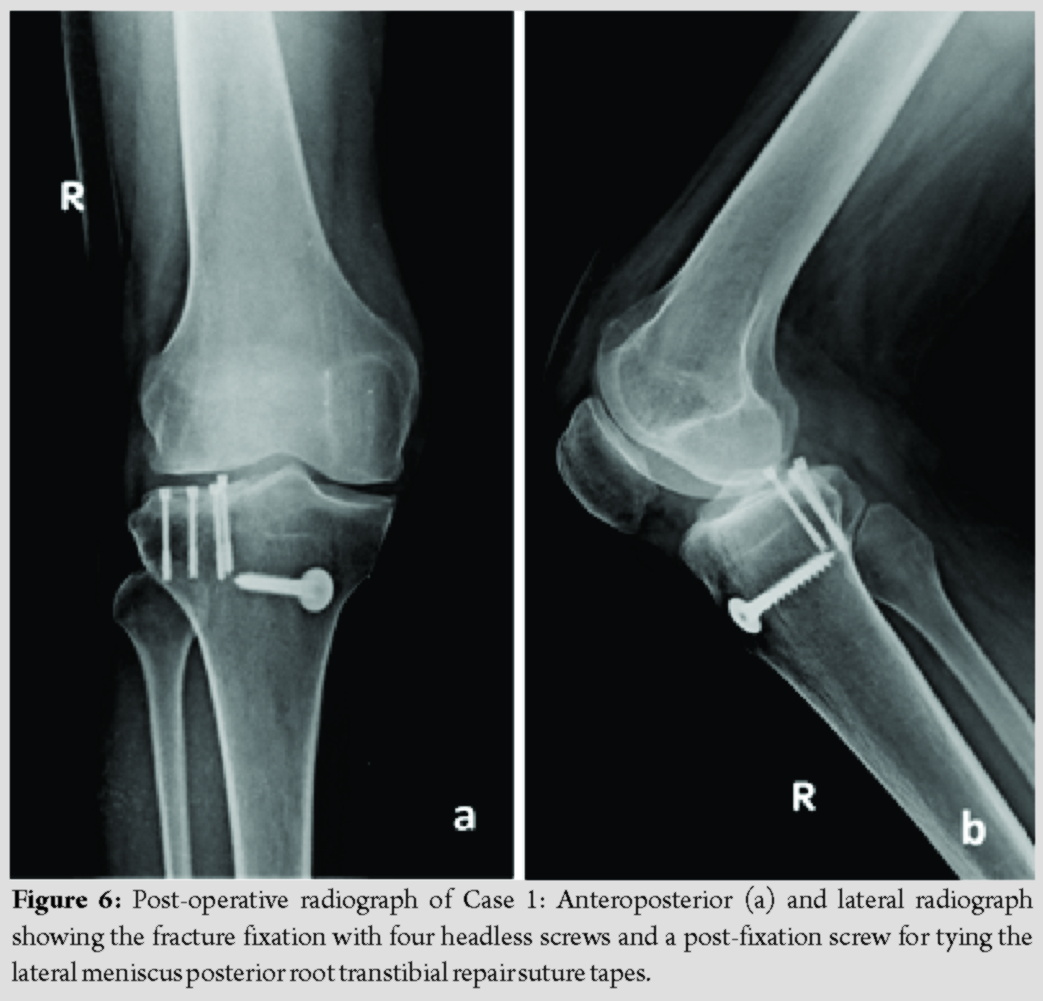
The flipped lateral meniscus was then reduced and the posterior root repaired by transtibial pull through technique using two SutureTapes® (Arthrex, Naples, FL) tied over a post-fixation screw. The body of the meniscus was repaired by inside-out technique with twelve 2-0 FiberWire® (Arthrex, Naples, FL) sutures. MCL tear on the femoral side was repaired primarily with No. 2 FiberWire® (Arthrex, Naples, FL). The ACL tear was not treated at this stage. Postoperatively, the patient was kept non weight-bearing for 4 weeks and allowed gentle range of motion up to 90°.Cryotherapy was started immediately for edema control, along with static exercises for quadriceps and gluteus. Closed chain kinetic exercises were advised for the first 2 months. After 4 weeks, partial weight-bearing for two weeks and full knee bending was allowed. The patient developed arthrofibrosis for which manipulation under general anesthesia was performed after 6 weeks. He subsequently underwent an anatomic single-bundle ACL reconstruction with hamstrings autograft 8 months after the first surgery. The patient is asymptomatic after 12 months of surgery and the osteochondral fragment has healed (Fig. 5).
He has attained full knee range of motion, good quadriceps tone, and power; the knee is stable. The knee range of motion is 0–138° at final follow-up.The Tegner-Lysholm score improved from 38 pre-surgery to 94 at final follow-up.
Case 2
The patient was explained about the need for surgery. The knee was approached through a medial parapatellar arthrotomy like the previous case. The osteochondral fragment from posterolateral tibia was entrapped in the fat pad, ACL was avulsed from the femoral side, lateral meniscus was flipped anteriorly, and MCL peeled off from the femoral attachment (Fig. 6). The osteochondral fragment was treated in the same way by fixation with four 2.4 mm headless compression screws (DePuy Synthes). The lateral meniscus posterior root was repaired by transtibial pull-out sutures and body was repaired with inside-out sutures in the same fashion as the first patient. The ACL was repaired to its femoral footprint using a titanium 5.5 mm CorkScrew® suture anchor (Arthrex, Naples, FL).Finally, the MCL was repaired to its femur attachment using a titanium 5.5 mm CorkScrew® suture anchor. This patient was also kept non weight-bearing with gentle range of motion up to 90°. Like the previous patient, cryotherapy was started immediately for edema control, along with static exercises for quadriceps and gluteus. Closed chain kinetic exercises were advised for the first 2 months. After 4 weeks, partial weight-bearing for two weeks and full knee bending was allowed. This patient also developed arthrofibrosis for which manipulation under general anesthesia was performed after 8 weeks. The patient is asymptomatic after 12 months of surgery and the fracture has healed (Fig. 7).
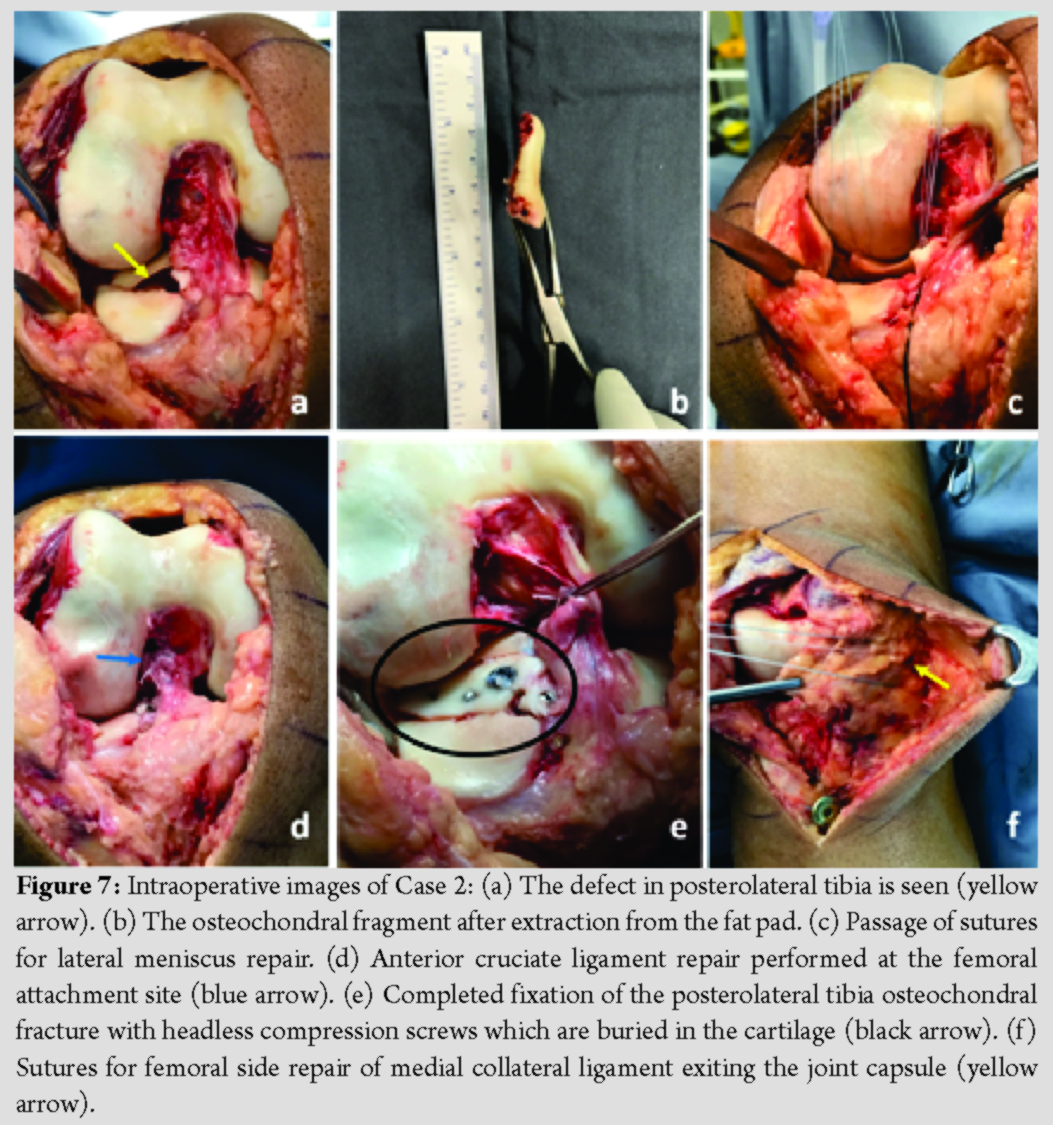
He has a deficit of 5° terminal flexion, good quadriceps tone, and power; the knee is stable. The knee range of motion is 0–128° at final follow-up.The Tegner-Lysholm score improved from 42 pre-surgery to 86 at final follow-up.
Case 3
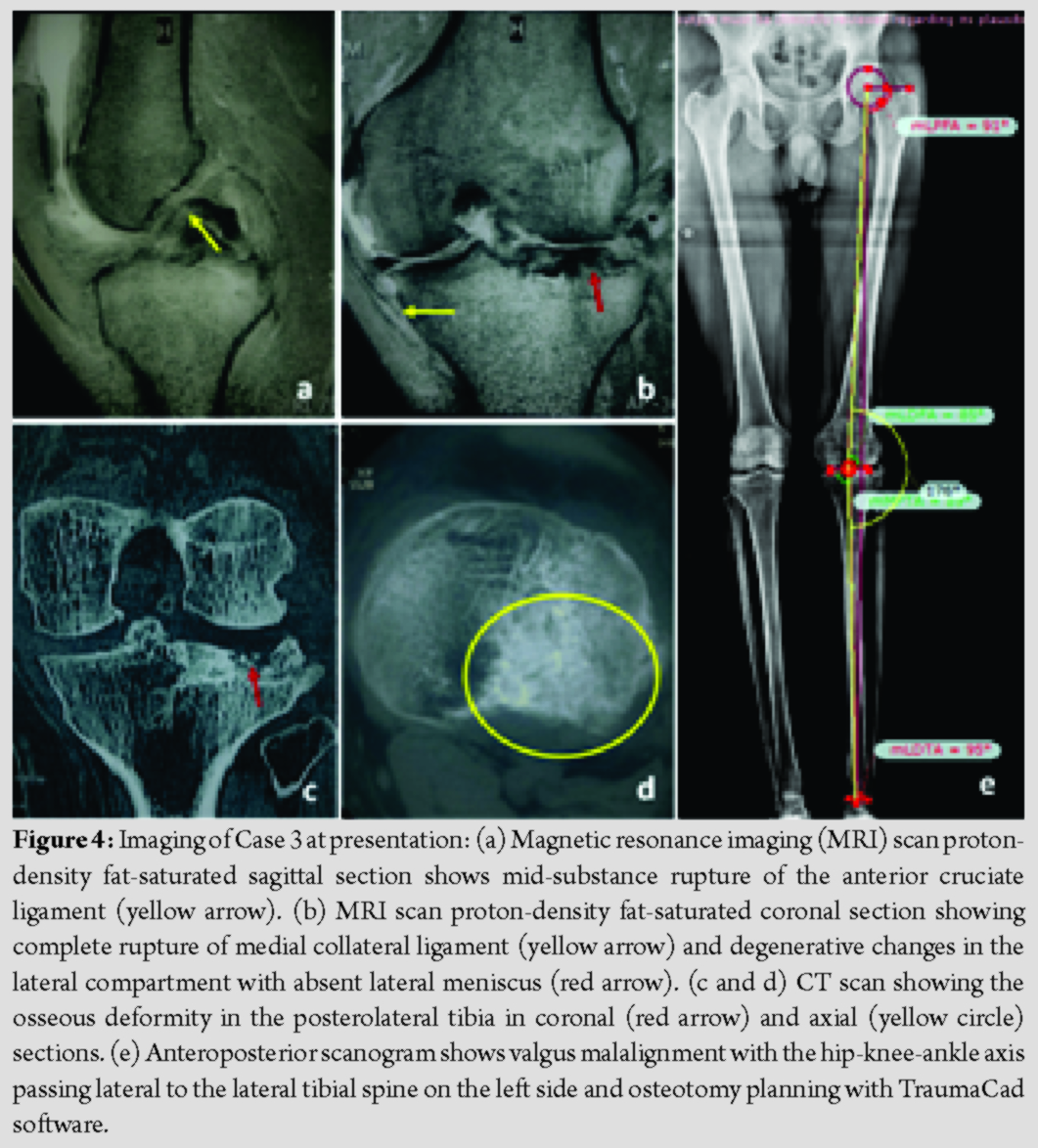
The primary treatment of the patient had already been performed elsewhere and his presenting symptoms included instability and continuous pain in his knee. The plan was to correct his malalignment and treat medial and anterior knee instability. The planning for this deformity correction was done using TraumaCad® (BrainLab, Munich, Germany) software. The anatomic medial proximal tibia angle was 89°, lateral distal femur angle was 85°, and hip knee axis was 184°. It was decided to correct the valgus alignment by a distal femur osteotomy because the coronal alignment of tibia was normal, and an osteotomy at this level would have tilted the joint line. Arthroscopy was performed, which revealed full-thickness cartilage loss of the posterolateral tibial condyle and loss of lateral meniscus tissue (Fig. 8).

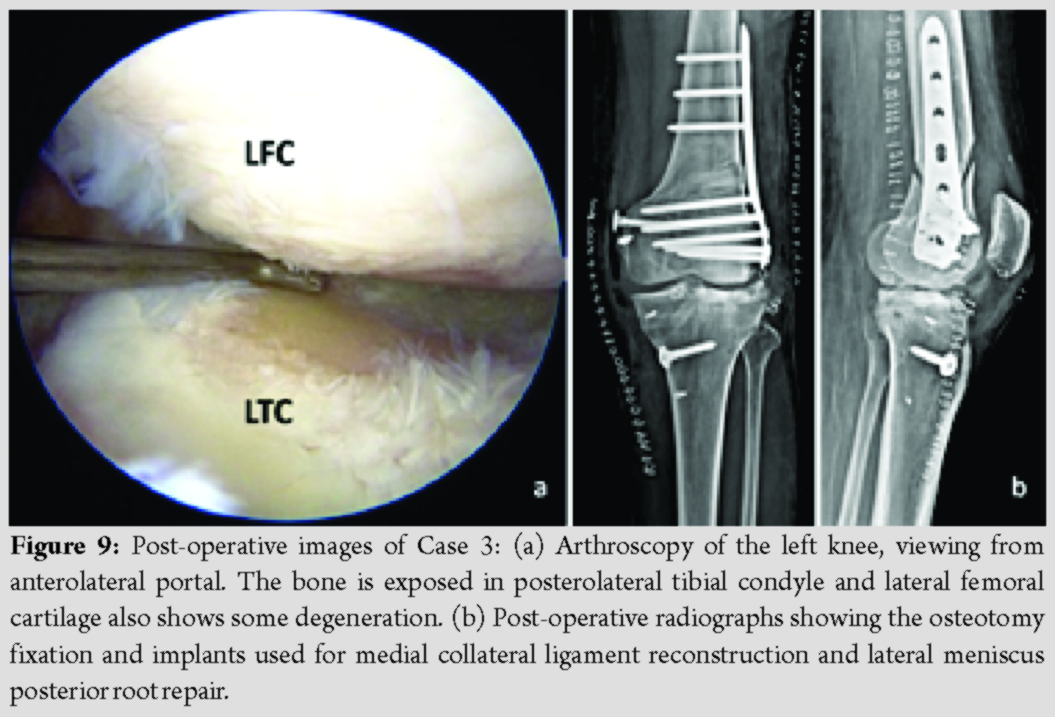
The patient underwent MCL reconstruction with semitendinosus autograft using a triangular construct [8], abrasion chondroplasty for cartilage defect, and a lateral open-wedge distal femur osteotomy with bone grafting (Fig. 9). An ACL reconstruction could not be performed due to hardware on the lateral femur. This procedure was a salvage to relieve patient symptoms and preserve the native knee. Postoperatively, the patient was kept non-weight-bearing and knee flexion restricted to 90° for 4 weeks. Exercises to achieve quadriceps control, cryotherapy for edema reduction, and closed chain kinetic exercises were started immediately. Full weight-bearing was allowed after 6 weeks. After 1 year follow-up, the patient does not complaint of instability but has occasional pain, especially after exertion. He has chosen to defer the ACL surgery. He has 10° deficit of flexion, quadriceps tone and power are good; the MCL is stable. The knee range of motion is 0–126° at final follow-up.The Tegner-Lysholm score improved from 47 pre-surgery to 72 at final follow-up.
Discussion
All the three patients had an injury combination of ACL tear, MCL injury, lateral meniscus posterior root tear, and osteochondral avulsion of posterolateral tibia. Such an injury complex has not been reported in literature to the best of our knowledge. When such an injury presents to a surgeon, a standard management protocol is not possible due to the complexity of the injury. However, anatomic reduction and fixation of the osteochondral injury by open surgery must take precedence, to avoid devastating sequel as was seen in our third case. The long-term outlook after this injury needs to be assessed. Both patients managed primarily by us (Cases 1 and 2) required manipulation under anesthesia after 6–8 weeks as they developed arthrofibrosis due to the extensive open surgery. Thus, the propensity of this injury and its management to cause knee stiffness must be borne in mind and explained to the patient. An osteochondral fracture of the posterolateral tibia occurring in association with ACL tear has been described previously [9, 10, 11]. The case reported by Andrade was the result of a motorcycle accident, where the fracture was fixed by a posterolateral approach and fibula head osteotomy [9]. Jiang reported two cases where an arthroscopic ACL reconstruction was performed and osteochondral fracture fixed through a posterolateral approach [10]. In the report by Teiet al., the osteochondral piece was very small in size in a skeletally immature patient and this was treated by excision of the fragment [11]. The mode of injury is definitely high-velocity trauma causing such severe disruption in the knee. We believe that the mechanism of the injury tetrad is a more exaggerated “lateral quartet” trauma pattern as described before, along with a valgus force [12, 13, 14]. The lateral quartet involves injuries to the ACL, lateral meniscus root, and bone bruises in lateral femoral condyle and posterolateral tibia. It has been hypothesized that a combination of anterior translation and external tibia rotation causes the injury pattern. With more violent force, as happens in a motorcycle crash, the posterolateral tibia bone bruise is aggravated, resulting in the osteochondral avulsion. A simultaneous valgus force would likely cause tearing of the MCL as the knee buckles after the bone fragment has flipped out. The association of articular cartilage injury of posterolateral tibia with ACL tear when bone bruise is detected on MRI scan is also known [15].
Conclusion
We report a new injury tetrad of ACL tear, MCL tear, lateral meniscus posterior root tear, and posterolateral tibia osteochondral fracture. The mechanism of injury is most likely a violent external rotation and anterior translation of the tibia with a valgus directed force during impact. The treatment of this injury can be performed in single or two stages based on the merits of the case. Anatomic reduction and fixation of the fracture takes precedence to avoid later devastating sequel for the knee.
Clinical Message
A hitherto unreported injury pattern following knee trauma is reported, comprising an ACL tear, MCL tear, lateral meniscus posterior root avulsion, and osteochondral fracture of the posterolateral tibia. The surgical management of this injury involves fixation of the fracture with headless screws, transtibial lateral meniscus root repair, ACL repair or reconstruction, and MCL repair or reconstruction. The mechanism of injury is postulated to be external rotation and anterior translation of the tibia with a valgus directed force during impact.
References
1. Mehl J, Otto A, Baldino JB, Achtnich A, Akoto R, Imhoff AB, et al. The ACL-deficient knee and the prevalence of meniscus and cartilage lesions: a systematic review and meta-analysis (CRD42017076897).Arch Orthop Trauma Surg 2019;139:819-41.
2. Praz C, Vieira TD, Saithna A, Rosentiel N, Kandhari V, Nogueira H, Sonnery-Cottet B. Risk factors for lateral meniscus posterior root tears in the anterior cruciate ligament-injured knee: An epidemiological analysis of 3956 patients from the SANTI study group. Am J Sports Med2019;47:598-605.
3. Westermann RW, Spindler KP, Huston LJ, Wolf BR. Outcomes of grade III medial collateral ligament injuries treated concurrently with anterior cruciate ligament reconstruction: A multicenter study. Arthroscopy 2019;35:1466-72.
4. Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF.Fracture and dislocation classification compendium-2018. J Orthop Trauma 2018;32 Suppl 1:S1-170.
5. Vicenti G, Solarino G, Carrozzo M, De Giorgi S, Moretti L, De Crescenzo A, et al. Major concern in the multiligament-injured knee treatment: A systematic review. Injury 2019;50 Suppl 2:S89-94.
6. Moatshe G, Chahla J, La Prade RF, Engebretsen L. Diagnosis and treatment of multiligament knee injury: State of the art. J ISAKOS 2017;2:152-61.
7. Schenck RC. The dislocated knee. Instr Course Lect 1994;43:127-36.
8. Lind M, Jakobsen BW, Lund B, Hansen MS, Abdallah O, Christiansen SE. Anatomical reconstruction of the medial collateral ligament and posteromedial corner of the knee in patients with chronic medial collateral ligament instability. Am J Sports Med 2009;37:1116-22.
9. De Andrade MA, Pimenta FS, DeAbreu E Silva GM, De Oliveira Campos TV, Pires RE. Displaced osteochondral fracture of the posterolateral tibial plateau associated with an acute anterior cruciate ligament injury. Trauma Case Rep 2019;20:100172.
10. Jiang L, Wu H, Yan S. Two cases of contact anterior cruciate ligament rupture combined with a posterolateral tibial plateau fracture. Case Rep Orthop 2015;2015:250487.
11. Tei K, Kubo S, Matsumoto T, Matsushita T, Matsumoto A, Kurosaka M, et al. Combined osteochondral fracture of the posterolateral tibial plateau and segond fracture with anterior cruciate ligament injury in a skeletally immature patient. Knee Surg Sports Traumatol Arthrosc 2012;20:252-5.
12. Forkel P, Petersen W. Knee ligment injuries. In: Oestern HJ, Trentz O, Uranues S, editors. Bone and Joint Injuries. European Manual of Medicine. Berlin: Springer-Verlag; 2014.
13. Petersen W, Forkel P, Achtnich A, Metzlaff S, Zantop T. Injuries of the anterior cruciate ligament: From prevention to therapy. Orthopädische und Unfallchirurgische Praxis 2012;6:232-43.
14. Herbst E, Hoser C, Tecklenburg K, Filipovic M, Dallapozza C, Herbort M. The lateral femoral notch sign following ACL injury: Frequency, morphology and relation to meniscal injury and sports activity. Knee Surg Sports Traumatol Arthrosc 2015;23:2250-8.
15. Nishimori M, Deie M, Adachi N, Kanaya A, Nakamae A, Motoyama M, et al. Articular cartilage injury of the posterior lateral tibial plateau associated with acute anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc 2008;16:270.
 |
 |
 |
 |
| Dr. Anshu Shekhar | Dr. Ankur Singh | Dr. Amit Laturkar | Dr. Sachin Tapasvi |
| How to Cite This Article: Shekhar A, Singh A, Laturkar A, Tapasvi S. Anterior Cruciate Ligament Rupture with Medial Collateral Ligament Tear with Lateral Meniscus Posterior Root Tear with Posterolateral Tibia Osteochondral Fracture: A New Injury Tetrad of the Knee. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 36-42. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


