
[box type=”bio”] Learning Point of the Article: [/box]
Acetabular stress fractures are exceedingly rare but if consideration for the diagnosis is made and appropriate investigations undertaken, even conservative management can have desirable outcomes.
Case Report | Volume 10 | Issue 3 | JOCR May – June 2020 | Page 85-89 | Sean Garcia, Trevor Seepaul. DOI: 10.13107/jocr.2020.v10.i03.1762
Authors: Sean Garcia[1], Trevor Seepaul[1]
[1]Department of Orthopaedic Surgery, San Fernando General Hospital, Independence Ave, San Fernando, Trinidad, West Indies.
Address of Correspondence:
Dr. Sean Garcia,
Department of Orthopaedic Surgery, San Fernando General Hospital, Independence Ave, San Fernando, Trinidad, West Indies.
E-mail: seangarcia3@hotmail.com
Abstract
Introduction: Stress fractures are overuse injuries resulting from repetitive submaximal loading of a bone. Acetabular stress fractures while highly uncommon can occur in those undergoing intense endurance training as is the case with military recruits. Diagnosis of this injury can be dubious at times, with magnetic resonance imaging (MRI) being the most sensitive diagnostic tool considering the lower sensitivity of plain film radiography.
Case Report: The authors report a case of acetabular stress fracture occurring in a healthy male amateur endurance runner presenting with activity related hip pain that presented acutely without any prodromal pain. Plain film radiography and MRI revealed a transverse fracture of the acetabulum.
Conclusion: Stress fractures of the acetabulum are among the rarest locations in which stress fractures can occur. They typically occur in individuals undergoing intense endurance training and require a high degree of suspicion to diagnose. The patient presented within represents a unique presentation not previously described.
Keywords: Acetabulum, stress fracture, athletics.
Introduction
Stress fractures are those that result from repetitive submaximal loading of a bone so as not to result in a fracture in an acute setting, but rather after a substantial period of time has passed [1, 2, 3]. They are more common in endurance athletes and military recruits as these populations represent those who undergo repetitive, rigorous training and typically tend to occur in the lower extremities [1, 2, 3]. Stress fractures of the acetabulum, as an individual entity, represents one of the least common types of stress fractures known to occur but its prodromal course closely resembles that of a typical stress fracture [3]. The following case report describes a patient who sustained a stress fracture of the acetabulum but follows a presentation separate from most instances of this pathology.
Case Report
A 51-year-old male amateur endurance runner presented with a 1-day history of sudden onset left hip pain and limp aggravated by weight bearing. The patient was previously well, he had a body mass index (BMI) of 21 and recalls no associated trauma. He also gave no history of any prodromal pain. He described that at the time of injury he had just initiated his training routine with a short sprint when he heard a popping noise localized to the left hip with a subsequent inability to fully weight bear on the left lower limb due to pain. Physical examination revealed normal range of motion at the hip but with pain at the extremes of motion as well as pain on axial compression of the hip. Plain film radiographs revealed nondisplaced transverse fracture of the acetabulum (Fig. 1). T2 weighted magnetic resonance imaging (MRI) demonstrated the same with surrounding bone edema and no evidence of lytic lesions or other pathological processes (Fig. 2). Blood investigations were normal inclusive of calcium, parathrmone and Vitamin D levels. A bone density scan (DEXA) of both hips and lumbar spine was within normal limits. Treatment was initiated with non-weight bearing ambulation for a 6-week period. At the end of the 6-week period, repeat plain film radiographs showed satisfactory healing of the fracture. Gradual weight bearing was permitted. The remainder of his recovery was uneventful.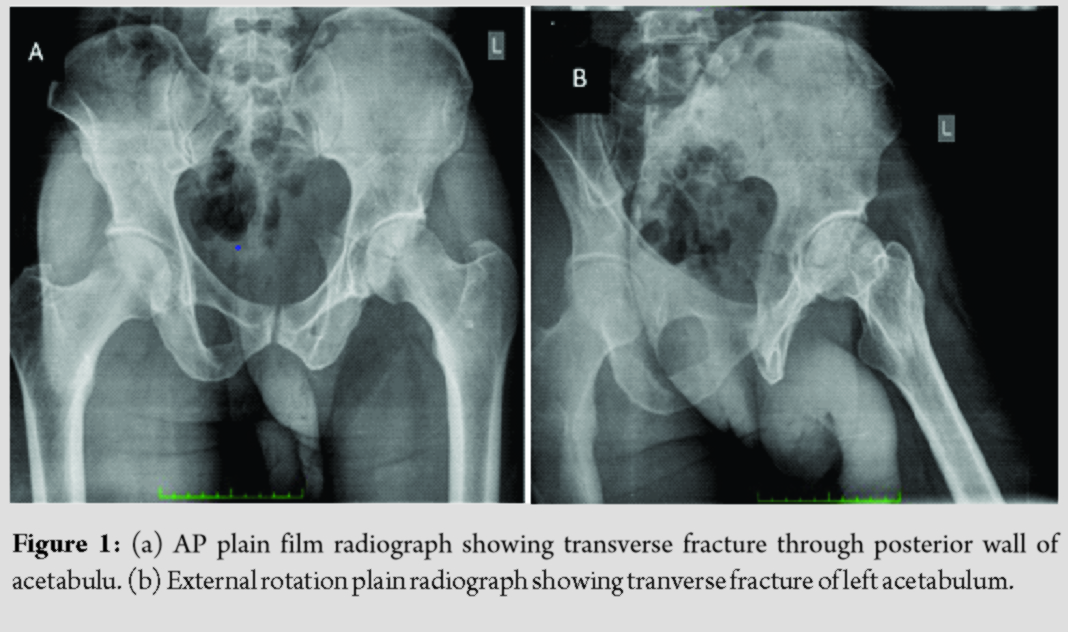
Discussion
Stress fractures are more common in the lower extremities and typically involve the tarsal bones, tibia and metatarsals with a smaller minority involving the femur, fibula, pelvis and spine [1, 5, 6]. Stress fractures are known to occur among athletes that underwent rigorous endurance training for track or long-distance running [1, 2, 3, 5, 6]. Risk factors include, metabolic abnormalities, menstrual disturbances, decreased bone density and nutritional disorders including low BMI and low Vitamin D levels [7, 8, 9]. Our patient had both a normal BMI and bone quality related investigations. Stress fractures of the acetabulum and pelvis remain an uncommon entity, but its incidence has been reported among military recruits [3] with isolated incidents among ballet dancers, a power lifter and a motocross rider [9, 10, 11]. Patients typically complain of prior activity related hip pain with no acute history of trauma. Interestingly, our case reported no such problems. A study reviewing 178 military recruits with hip pain identified 12 patients on MRI with acetabular stress fractures. Most fractures occurred at the roof of the acetabulum [3]. In the elderly population these have the potential to result in protrusio acetabuli as was identified in some extreme cases [12]. Anterior column stress fractures were found to occur sometimes in isolation but also with concomitant inferior pubic rami fractures [3]. Plain film radiographs of stress fractures usually appear normal or show sclerotic changes except in the case of grossly displaced fractures [4, 10]. Nuclear scintigraphy may provide evidence of a fracture but is nonspecific [4]. MRI remains the most reliable tool in identifying stress fractures of the lower extremity due to its higher sensitivity and specificity as well as the added benefit of not requiring the use of ionizing radiation [4]. The widespread use of MRI has led to the introduction of the term “stress injury.” Kiuru, Fredericson and others have proposed MRI classifications which describe a spectrum of stress injury with fracture present in the latter grades [2, 13]. On further review it is noted that many reports do not separate the two terms which leads to an apparent disparity in incidence and diagnosis of injuries and fractures between centers that liberally utilize MRI investigations either as a first line or research tool. Our case as well as that of the power lifter described by Karnes et al. are consistent with stress fracture whereas the case of the ballet dancer and motocross rider reported by Thienport et al. and de Paiva Luciano and Filho respectively are seemingly more consistent with stress injury. More recently, prospective work such as that described by Nattiv and Armsey has confirmed that the rate of recovery is dependent on MRI grade of stress injury; with those illustrating a fracture line on MRI requiring a significantly longer time to fully return to sport [14]. In general, treatment is best served by early identification of a stress fracture and rest in the form of non-weight bearing on the affected limb for 4–6 weeks with gradual return to pre-injury activities following rehabilitation [15, 16]. Most stress fractures heal within 3 months of initiating treatment [4]. However isolated data on the healing of acetabular stress fractures is quite limited and often buried within larger groups of more common stress fracture patterns. Metabolic abnormalities, menstrual disturbances and nutritional disorders should be identified and corrected where possible [15]. Use of shock absorbing insoles has been beneficial in reducing the incidence of stress fractures and stress reactions of bone [17]. Our observations based on the patient described in this report suggest that conservative management, as detailed above, allows for a successful outcome in the management of nondisplaced acetabular stress fractures.
Conclusion
Acetabular stress fractures typically follow a similar natural course, with regards their presentation, to most other stress fractures. However, as was the case in this report, unique presentations cannot be ruled out and if the suspicion exists, then the diagnosis must be sought out.
Clinical Message
Being such an uncommon presentation, a stress fracture of the acetabulum requires a high index of suspicion to diagnose. Diagnosis relies heavily on accurate discernment of the history and natural progression of the ailment aided by thorough examination of the affected extremity. Furthermore, plain film radiography alone may not be enough to reliably diagnose a stress fracture and MRI is likely to be required to ascertain the true extent of the injury.
References
1. Orava S, Hulkko A, Koskinen S, Taimela S. Stress fractures in athletes and military recruits. An overview. Orthopade 1995;24:457-66.
2. Fredericson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging 2006;17:309-25.
3. Williams T, Puckett ML, Denison G, Shin AY, Gorman JD. Acetabular stress fractures in military endurance athletes and recruits: Incidence and MRI and scintigraphic findings. Skeletal Radiol 2002;31:277-81.
4. Wright AA, Hegedus EJ, Lenchik L, Kuhn KJ, Santiago L, Smoliga JM. Diagnostic accuracy of various imaging modalities for suspected lower extremity stress fractures: A systematic review with evidence-based recommendations for clinical practice. Am J Sports Med 2016;44:255-63.
5. Matheson G, Clement D. Stress fractures in athletes. A study of 320 cases. Am J Sports Med 1987;15:46-58.
6. Brukner P, Bradshaw C. Stress fractures: A review of 180 cases. Clin J Sports Med 1996;6:85-9.
7. Myburgh KH, Hutchins J, Fataar AB. Low bone density is an etiologic factor for stress fractures in athletes. Ann Intern Med 1990;113:754-9.
8. Nattiv A, Armsey TD Jr. Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
9. Thienport E, Simon J. Stress fracture of the acetabulum in a ballet dancer. A case report. Acta Orthop Belg 2005;71:740-2.
10. Karnes JM, Hagedorn J, Hubbard DF. Catastrophic failure of an acetabular stress fracture in a healthy male power lifter. Am J Sports Med 2015;43:2559-63.
11. de Paiva Luciano A, Filho NF. Stress fracture in acetabular roof due to motocross. Rev Bras Ortop 2016;51:374-7.
12. Akinbo O, Tyagi V. Acute stress fracture of the pelvis after total hip arthroplasty: A case report. J Orthop Case Rep 2017;7:87-9.
13. Kiuru MJ, Pihlajamaki HK, Hietanen HJ, Ahovuo JA. MR imaging, bone scintigraphy and radiography in bone stress injuries of the pelvis and lower extremities. Acta Radiol 2002;43:207-12.
14. Nattiv A, Kennedy G, Barrack MT, Abdelkerim A, Goolsby MA, Arends JC, et al. Correlation of MRI grading of bone stress injuries with clinical risk factors and return to play: A 5-year prospective study in collegiate track and field athletes. Am J Sports Med 2013;41:1930-41.
15. Brukner P, Bennell K. Stress fractures in female athletes. Diagnosis, management and rehabilitation. Sports Med 1997;24:419-29.
16. Hulkko A, Orava S. Stress fractures in athletes. Int J Sports Med 1987;8:221-6.
17. Gillespie WJ, Grant I. Interventions for preventing and treating stress fractures and stress reactions of bone of the lower limbs in young adults. Cochrane Database Syst Rev 2000;2:CD000450.
 |
 |
| Dr. Sean Garcia | Dr. Trevor Seepaul |
| How to Cite This Article: Garcia S, Seepaul T. Acetabular Stress Fracture in a Healthy Male Amateur Endurance Runner. A Case Report. Journal of Orthopaedic Case Reports 2020 May-June;10(3): 85-87. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


