
[box type=”bio”] Learning Point of the Article: [/box]
Atypical mechanism of injury for fracture neck femur involving blunt trauma.
Case Report | Volume 10 | Issue 5 | JOCR August 2020 | Page 31-33 | Sameer Aggarwal, Chirag Arora, Vishal Kumar, Prasoon Kumar. DOI: 10.13107/jocr.2020.v10.i05.1826
Authors: Sameer Aggarwal[1], Chirag Arora[1], Vishal Kumar[1], Prasoon Kumar[1]
[1]Department of Orthopaedics, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
Address of Correspondence:
Dr. Chirag Arora,
C-2/74 Ashok Vihar Phase 2, New Delhi – 110 052, India.
E-mail: aro.chirag@gmail.com
Abstract
Introduction: Simultaneous bilateral neck femur fracture is a rare entity that has been associated with metabolic disorders, osteoporosis, drugs, trauma, and seizure disorders. Its occurrence following a physical assault is very rare. We present a case report of a prisoner presenting with bilateral neck femur fracture following a physical assault during prison confinement.
Case Presentation: This article presents the case of a 64-year-old male prisoner who sustained bilateral intracapsular fracture neck femur following the physical assault. Bilateral uncemented total hip replacement was done using a posterior approach at separate sittings. The patient made an uneventful recovery with return of pain-free normal range of motion at the time of discharge. The weight-bearing mobilization was allowed immediately following bilateral hip arthroplasty. Harris hip score at the time of discharge and the last follow-up of 12 months was 83.4 and 90.3, respectively. No wound-related or other systemic complications were noted.
Conclusion: bilateral fracture neck femur is commonly associated with metabolic conditions, rarely associated blunt trauma. This article highlights the need to suspect these fracture in all elderly cases presenting with hip pain.
Keywords: Arthroplasty, assault, bilateral neck femur fracture, osteosynthesis.
Introduction
The traumatic simultaneous bilateral neck of femur fractures is a rare occurrence. Bilateral fractures of the neck of the femur have been reported to have occurred following trauma, metabolic disorders, osteoporosis, drugs, and seizure disorders secondary to convulsions. Major disorders associated with these fractures include osteomalacia, malnutrition, hyperparathyroidism, cystic fibrosis, bone tumors, and renal osteodystrophy [1]. Violent muscle contractions, as seen during convulsions or electric shock, are also known causes. Osteosynthesis is the preferred treatment modality in bilateral neck femur fractures at a younger age. Total hip arthroplasty (THA) is recommended in relatively elder age group patients. THA should be avoided in cases with uncontrolled seizures due to an elevated risk of instability and dislocation when the neurological terrain is taken into account. Early diagnosis, surgical intervention, aggressive post-operative mobilization and discharge, according to best practice guidelines [2], result in satisfactory outcomes in most cases. We aim to analyze, discuss, and review the management as well as complications of bilateral intracapsular neck femur following trauma in a physiologically active patient population, in routine orthopedic practice.
Case Presentation
A 64-year-prisoner presented with pain in both hip region and inability to bear weight over bilateral lower limbs. He was an active, independent man with no significant comorbidities other than hypertension which is well controlled on regular treatment. His pre-morbid mobility status was good, and he did not require any walking aids. The patient sustained the injuries following physical torture in prison; he was hanged by one leg at a time and tortured with wooden planks. Clinical examination revealed external rotation of both legs and pain on passive movement of both hips. X-ray of his pelvis showed displaced intracapsular hip fractures on both sides (Garden type IV bilateral) (Fig. 1). The fractures were treated by uncemented THA using modular prostheses. The patient was operated first on the right side and later on the left side at a gap of 10 days. The surgery was performed by a senior orthopedic surgeon in the supine position under general anesthesia, using a posterior approach. He had a satisfactory post-operative recovery and was able to mobilize with full weight-bearing within 2 days following surgery (Fig. 2, 3).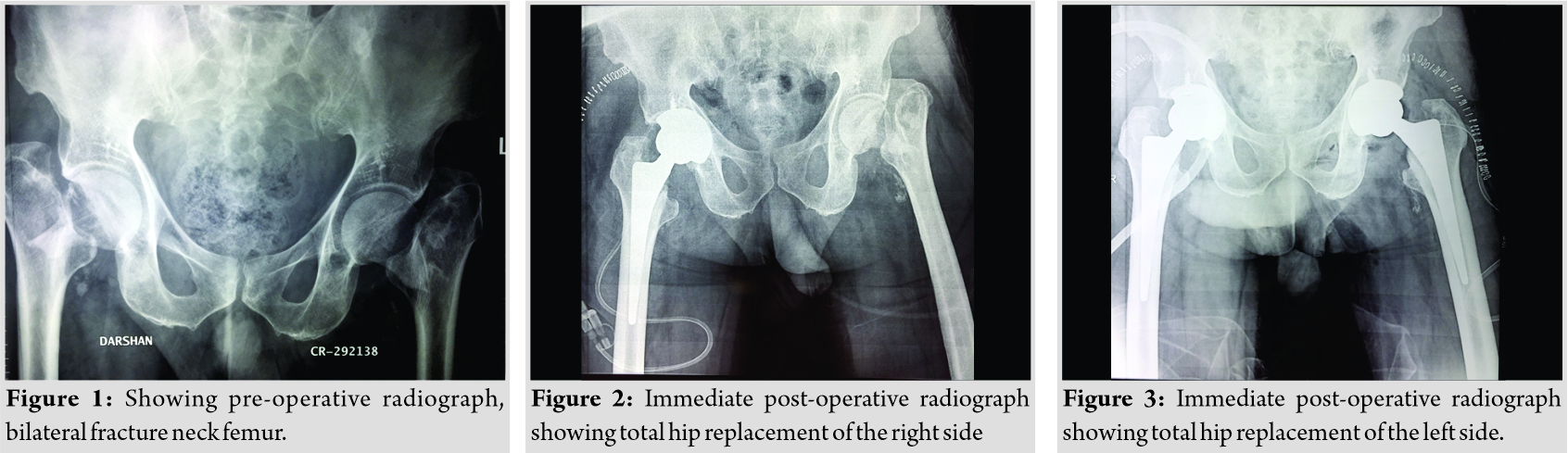
Discussion
Trauma is a rare cause of bilateral fracture neck femur; most cases occur following seizures secondary to epilepsy, drugs, and electrocution [2]. Intracapsular fractures of neck femur before the fifth decade of life usually result from high-velocity trauma; these may be associated with ipsilateral shaft or distal femur fractures or dislocations of hip and knee. Konforti et al. [3] described bilateral neck femur fractures in a 37-year-old gentleman who was crushed during a mining accident. Carrell et al. [4] described the case of an 8-year-old boy who sustained a bilateral neck fractures following a 25 foot fall. Convulsions have been documented as a major cause for bilateral femoral neck fractures, most cases are secondary to metastasis or eclampsia rather than primary causes. Twenty cases of bilateral femur neck fractures after convulsive seizure have been reported in the literature since 1970 [5]. Violent contraction of the periarticular muscles, and particularly the pelvic-trochanteric muscles during the seizure, is the principle cause of these fractures. Associated fractures of proximal humerus [6, 7] and acetabulum have been reported. The antiepileptic drugs have a major side effect of avascular necrosis and osteomalacia; these drugs reduce Vitamin D absorption in the gut and augment bone turnover, leading to reduced bone density. Therefore, surgeons have favored replacement arthroplasty as a modality of choice; however, in the case of uncomplicated fractures, the treatment of choice remains osteosynthesis. There is a load of treatment options available for fracture neck of femur, including arthroplasty and osteosynthesis [8]. Osteosynthesis involving closed/open reduction and internal fixation with screws is preferred modality of treatment in the young population (<60 years), whereas replacement arthroplasty is the treatment of choice in older individuals with an aim to avoid repeat surgeries, allow early mobilization, and avoid complications due to recumbency. Nonetheless, there are no fixed guidelines for choosing one treatment option over another for a particular fracture [9]. The inadequate reduction has a high chance of non-union and avascular necrosis, subsequent shortening, and gait abnormalities [10].
The following table (Table 1) made after an extensive literature search depicts the rarity of this injury.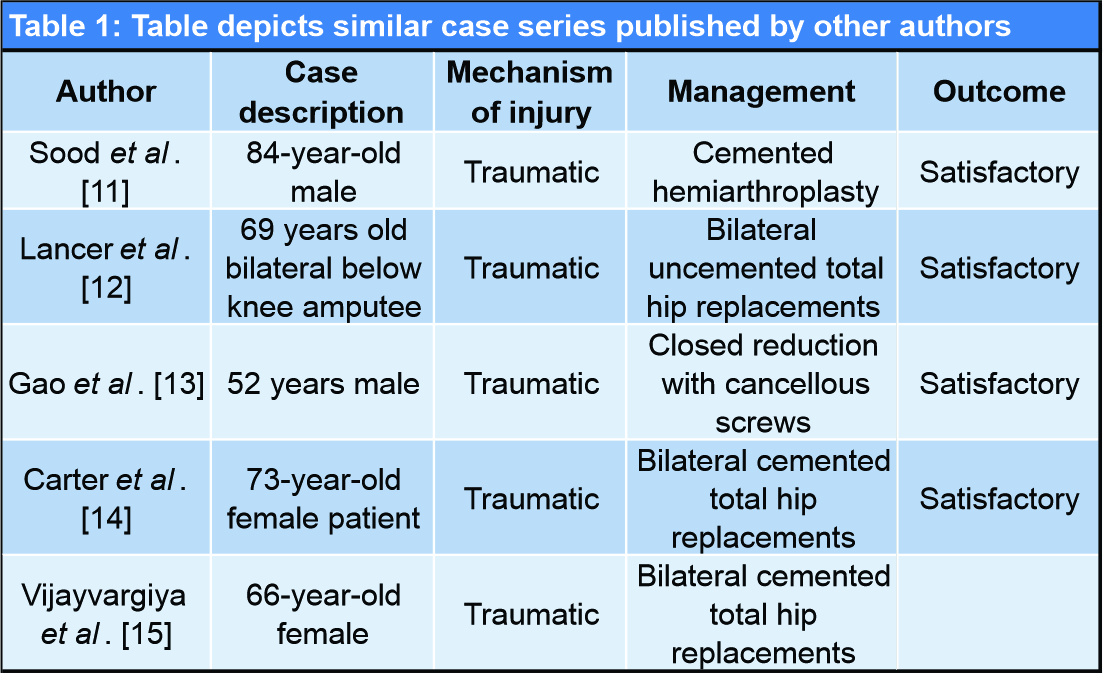
Conclusion
While a unilateral hip fracture is commonly managed appropriately on a regular basis by orthopedic surgeons, bilateral injuries of this nature presenting simultaneously can prove to be a diagnostic and therapeutic challenge. Early recognition and prompt adequate surgical intervention can lead to good outcomes despite the severity of this injury. A pathological workup should always be done to rule out associated conditions.
Clinical Message
There should be a low threshold for radiographic screening for fracture neck femur, especially in patients with compromised nutritional status or with other risk factors. Such a fracture may result as a result of trivial trauma or, in this case, due to physical assault.
References
1. Grimaldi M, Vouaillat H, Tonetti J, Merloz P. Simultaneous bilateral femoral neck fractures secondary to epileptic seizures: Treatment by bilateral total hip arthroplasty. Orthop Traumatol Surg Res 2009;95:555-7.
2. Powell HD. Simultaneous bilateral fractures of the neck of the femur. J Bone Joint Surg 1960;42:236-52.
3. Konforti B, Chokanov K. Simultaneous bilateral nailing by two teams of surgeons in fractures of the femoral neck. Khirurgiia (Sofia) 1956;9:75-8.
4. Carrell B, Carrell WB. Fractures in the neck of the femur in children with paticular reference to aseptic necrosis. J Bone Joint Surg 1941;23:225.
5. Hughes CA, O’Brian DS. Sudden death from pelvic haemorrhage after bilateral central fracture dislocations of the hip due to an epileptic seizure. Am J Forensic Med Pathol 2000;21:380-4.
6. Haronian E, Silver JW, Mesa J. Simultaneous bilateral femoral neck fracture and greater tuberosity shoulder fracture resulting from seizure. Orthopedics 2002;25:757-8.
7. McGlone R, Gosnold JK. Posterior dislocation of shoulder and bilateral hip fractures caused by epileptic seizure. Arch Emerg Med 1987;4:115-6.
8. Hofmann A, Wyatt R. Missed Subcapital Fractures. Ann Emerg Med 1984;13:951-5.
9. Parker MJ. Missed hip fractures. Arch Emerg Med 1992;9:23-7.
10. Zielinski SM, Keijsers NL, Praet SF, Heetveld MJ, Bhandari M, Patka P, et al. Femoral neck shortening after internal fixation of a femoral neck fracture. Orthopedics 2013;36:e849-58.
11. Sood A, Rao C, Holloway I. Bilateral femoral neck fractures in an adult male following minimal trauma after a simple mechanical fall: A case report. Cases J 2009;2:92.
12. Carter T, Jefferies JG. Bilateral simultaneous neck of femur fractures arising from a simple mechanical fall a case report for guidance on safe surgical management. J Orthop Trauma Rehabil 2016;21:10-3.
13. Gao YS, Zhu ZH, Zhang CQ. Simultaneous bilateral fractures of the femoral neck caused by high energy: A case report and literature review. Chin J Traumatol 2015;18:304-6.
14. Lancer HR, Smitham P, Ray P. Bilateral neck of femur fractures in a bilateral below-knee amputee: A unique case. Case Rep Orthop 2016;2016:7083671.
15. Vijayvargiya M, Shetty V, Makwana K, Agarwal N. Bilateral simultaneous neck femur fracture following domestic fall in an elderly patient: A rare case report. Rev Bras Ortop 2017;52:363-5.
 |
 |
 |
 |
| Dr. Sameer Aggarwal | Dr. Chirag Arora | Dr. Vishal Kumar | Dr. Prasoon Kumar |
| How to Cite This Article: Aggarwal S, Arora C, Kumar V, Kumar P. Bilateral Neck Femur Fracture during Prison Confinement: An Atypical Mechanism of Injury. Journal of Orthopaedic Case Reports 2020 August;10(5): 31-33. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


