
[box type=”bio”] Learning Point of the Article: [/box]
Preoperative assessment of acetabular defects by 3 D printed models increases accuracy of acetabular defect identification and subsequent reconstruction.
Case Report | Volume 10 | Issue 7 | JOCR October 2020 | Page 18-21 | Bharath Loganathan, Vipin Sharma, MuthukumaranRavi Kumar, Sivamurugan Soundarapandian, Dhiraj Prem Sukh Marothi, Kavya Sharma. DOI: 10.13107/jocr.2020.v10.i07.1900
Authors: Bharath Loganathan[1], Vipin Sharma[2], MuthukumaranRavi Kumar[3], Sivamurugan Soundarapandian[1], Dhiraj Prem Sukh Marothi[1], Kavya Sharma[4]
[1]Department of Orthopaedics, Soundarapandian Bone and Joint Hospital, Chennai, Tamil Nadu, India.
[2]Department of Orthopaedics, Dr. Rajendra Prasad Government Medical College, Kangra at Tanda, Himachal Pradesh, India.
[3]Department of Orthopaedics, Railway Hospital, Chennai, Tamil Nadu, India.
[4]MBBS Student, MM Medical College, Kumarhatti-Solan, Himachal Pradesh. India.
Address of Correspondence:
Dr. Vipin Sharma,
H No 21, Type 5, Block B, Dr. RPGMC, Kangra at Tanda, Himachal Pradesh, India.
E-mail: vipinsh_hp@rediffmail.com
Abstract
Introduction: Acetabular reconstruction in a patient with neglected DDH during complex primary total hip replacement is a challenging procedure to do. We are reporting assessment of acetabular defect in one such patient with pre-operative 3D printing, followed by reconstruction with trabecular metal shell and augments.
Case Report: A 32-year-old female with neglected DDH (Crowe’s type 4) reported to us with pain, limp, and shortening of affected limb. Operated somewhere else with THR, she had a missing acetabular component and coral stem in situ at the time of presentation. Acetabular defect was assessed by 3D printing of pelvis following which acetabular reconstruction with tantalum cup and augments along with femoral stem revision was done.
Conclusion: This study confirmed the role of 3D printing pelvis model in meticulous pre-operative planning in patients with complex hip deformities. Reconstruction of acetabular defects with tantalum cup, and augments is a reasonable solution to achieve better function.
Keywords: 3D Printing, Acetabular defects, Tantalum cup.
Introduction
Distorted hip anatomy in patients with neglected developmental dysplasia hip presents with unique challenges, while performing total hip replacement [1, 2]. At the beginnings of arthroplasty era, total hip replacement in these groups of patients was thought to be practically impossible[3]. However, with passage of time accurate pre-operative planning and better surgical techniques have stood the test of time to make total hip replacement in such patients a feasible and long-lasting solution [1]. With the advent of 3D printing technology, accurate tactile and visual assessment of defect can be made on the printed model and pre-operative trialing with components can also be done. While pre-operative assessment of acetabular defects was done using 3D printing technology; the acetabular reconstruction was done using trabecular cup and metal augments.
Case Report
A 32-year-old female reported to us with pain, limp, and shortening of the left lower limb. The patient was on traction for the left lower limb. The previous records revealed that patient was operated for DDH 4 Left hip (Crowe’s Classification) at some other institute 3 weeks ago (Fig.1). During surgery eccentric reaming of acetabulum resulted in medial and posterosuperior acetabular wall defects. An uncemented metal backed cup was used on acetabular side and Corail stem was used for femoral side. Difficulty in achieving on table reduction of hip during surgery led surgeon to explant Corail stem and take a lower neck cut. However, this resulted in iatrogenic trochanteric fracture. Due to lack of proximal support in femur, Corail Stem(Depuy) was exchanged for distal fitting Solution stem (Depuy). Meanwhile acetabular component migrated medially which went unnoticed during surgery and was detected on postoperative X-rays (Fig. 2a).The acetabular component was removed by primary surgeon at subsequent surgery while femoral stem was retained in situ. Postoperatively, patient was placed on skin traction for 3 weeks.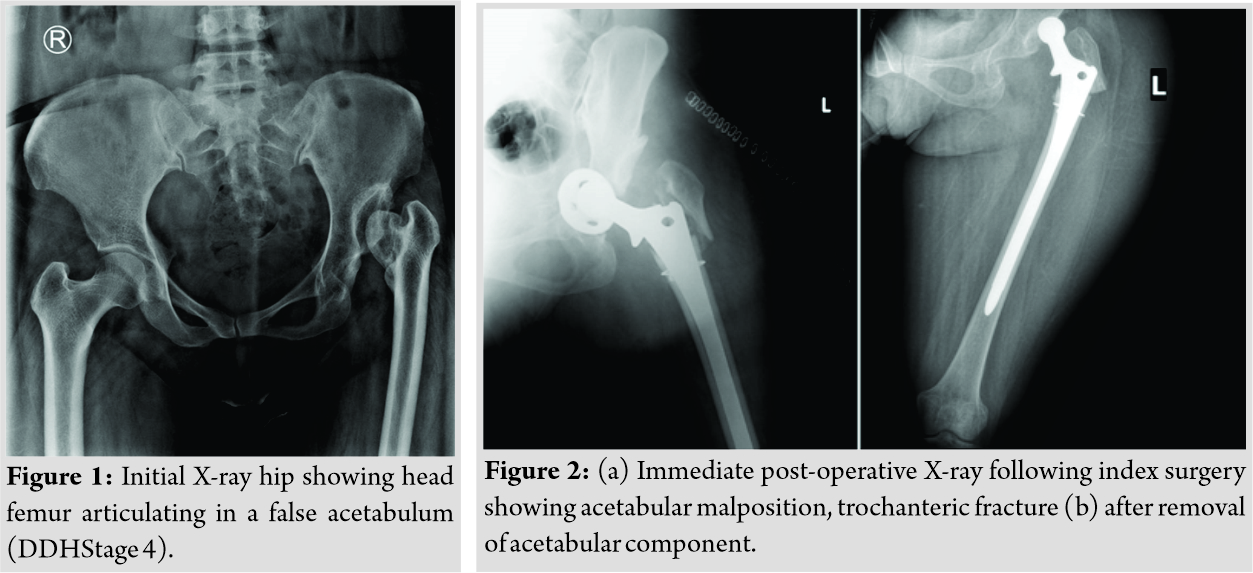
When the patient presented to us patient was non ambulatory and on traction for the left lower limb. X-ray at the time of presentation to us revealed empty bony acetabulum, fractured greater trochanter, and femoral stem (Solution) in situ (Fig. 2b).Subsequent investigations, for example, routine Hemogram, ESR, and CRP were normal while joint aspirate did not show any growth after 72 h of incubation.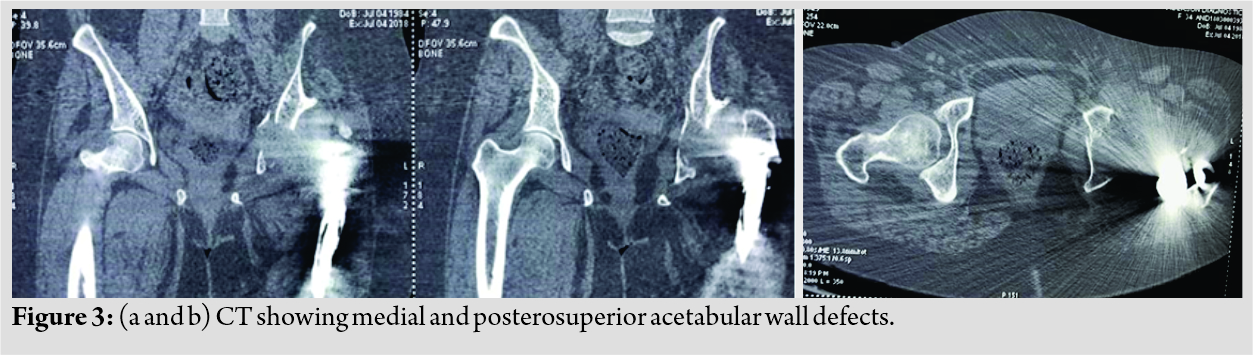
On the basis of CT of affected hip, which showed defects in medial and posterosuperior wall of true acetabulum (Fig. 3) a pre-operative 3D CT model of affected hip was printed to accurately assess the underlying acetabular defects and to see which acetabular reconstruction option worked best in current scenario (Fig. 4). 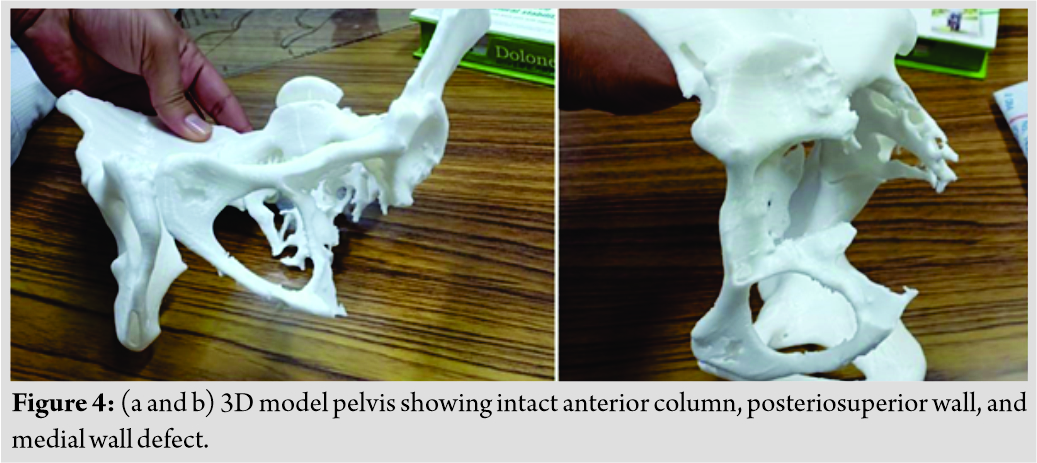 On the 3D model, a false acetabulum just superior to true acetabulum was noted; both acetabula being separated by a bony ridge. True acetabulum showed a breached medial wall, along with deficient posterosuperior wall and column defect. Pre-operative trialing was done using a Bursch Schneider cage of appropriate size on the 3D model of true acetabulum(Fig. 5). However, due to the presence of superior bony ridge between true and false acetabula, superior iliac flange of cage could not be seated over it properly. Hence, option of reconstruction of acetabular defect with tantalum posterior column wedge, tantalum cup, and tantalum augments was entertained.
On the 3D model, a false acetabulum just superior to true acetabulum was noted; both acetabula being separated by a bony ridge. True acetabulum showed a breached medial wall, along with deficient posterosuperior wall and column defect. Pre-operative trialing was done using a Bursch Schneider cage of appropriate size on the 3D model of true acetabulum(Fig. 5). However, due to the presence of superior bony ridge between true and false acetabula, superior iliac flange of cage could not be seated over it properly. Hence, option of reconstruction of acetabular defect with tantalum posterior column wedge, tantalum cup, and tantalum augments was entertained.
Operative steps
Patient was taken for surgery under epidural anesthesia and using posterolateral approach to hip. Based on pre-operative planning, surgical challenges anticipated were underlying deformed anatomy of acetabulum including breached medial wall and posterosuperior superior wall, column defect. Preoperatively, acetabular cavity had fibrosis. Since exposure was difficult due to fibrosis and femoral stem in situ, stem was extracted out to visualize the underlying anatomy better. After meticulous dissection, a global view of acetabulum was achieved and was confirmed using Image Intensifier TV control(C Arm). Preoperatively, acetabulum was found to have PaproskyIII A defect. Task was taken to construct acetabular defects first. Superior bony ridge between true and false acetabulum was erased with a burr. Acetabular posterior column tantalum wedge was anchored in iliac wing, and a multiholed tantalum cup (Zimmer) was placed in position and fixed with multiple screws. A highly cross linked poly (HXPE) liner (Zimmer) was cemented in the tantalum multiholed cup in 40 abduction and 15 anteversion (Fig. 6). 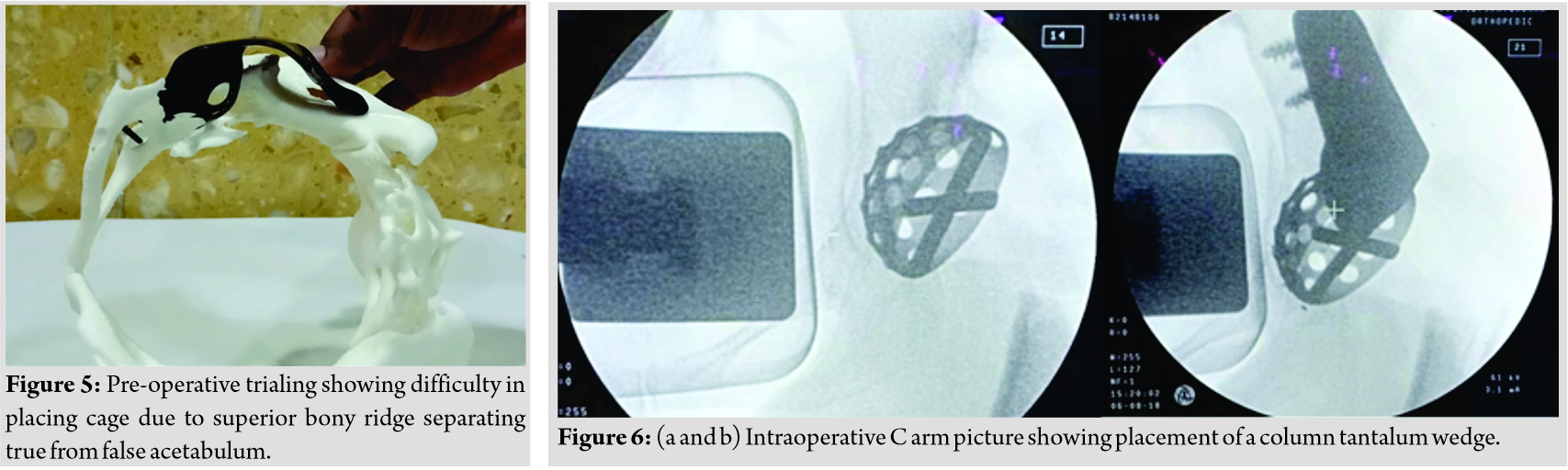 Since medial acetabular wall had some bone stock, so medial bone grafting was not done. Tantalum wedge and tantalum cup were cemented mutually at their points of contact. For femoral side, a distal fitting solution stem one size higher than original stem along with tension band wiring for greater trochanter fracture was done(Fig. 7). Postoperatively, patient was mobilized on day seven and discharged on day 14. Harris hip score of 90 was noted at 1year follow-up(Fig. 8).
Since medial acetabular wall had some bone stock, so medial bone grafting was not done. Tantalum wedge and tantalum cup were cemented mutually at their points of contact. For femoral side, a distal fitting solution stem one size higher than original stem along with tension band wiring for greater trochanter fracture was done(Fig. 7). Postoperatively, patient was mobilized on day seven and discharged on day 14. Harris hip score of 90 was noted at 1year follow-up(Fig. 8).

Discussion
Reconstruction of acetabular defect during Total Hip Replacement in Neglected DDH presents with unique challenges. In view of obscured surrounding landmarks, placement of acetabular cup in such cases is a difficult task. Some authors advocate placing the cup at high hip center, but studies have shown that elevation of hip center by even 1 mm, increases the load on hip to the tune of 0.1%, and increases body weight lever arm, leading to early failure of hip joint [1]. For cup to be stable and have adequate coverage at the level of true acetabulum, identification of true acetabulum and assessment of associated acetabular defects is required. Acetabular defects can be preoperatively assessed using 3D construction CT. In the present case pre-operative, 3D CT followed by 3D printing was used to print a model of pelvis with acetabular defects. This helped us to analyze configuration of true acetabulum and the associated defects. On 3D printing extent of posterosuperior and medial wall defect was identified. Along with a superior bony ridge could be seen separating the true from false acetabulum on 3D model. Although 3D CT reconstruction films have been used to preoperatively assess acetabular defects, 3D printed models are known to provide the surgeon with visual and tactile appreciation of acetabular defects preoperatively. Pre-operative templating and trialing of implants can be done on 3D models, thereby reducing chances of per-operative complications and reducing surgical time [4]. Studies have shown that 3D models help in pre-operative surgical simulation, enabling pre-operative cup, augment, buttress sizing, cage templating, thereby minimizing para-operative complications [5]. Reconstruction of posterosuperior defect is quite challenging with the literature coming up with various reconstruction options, such as autologous bone graft, allograft, cage along with autologous bone graft augmentation,Standard metal augments (prefabricated), and Custom made acetabular augments (3D printing). Each reconstruction option has its own merits and demerits. Some studies have advocated use of allograft or autograft for reconstruction of posterior superior acetabular defects. Although vascularized autografts hold the promise of better integration with iliac bone; donor site morbidity, graft failure, and graft resorption make autograft a less inviting option for reconstruction[6, 7]. Graft resorption and failure may lead to secondary instability at hip[1]. Use of allografts is also limited because of complications such as graft failure and graft resorption. Second, bone bank facilities are not available in every institute, hence limiting the use of allografts for acetabular reconstruction[1].Some authors have used half and full cup cage constructs for major acetabular defects, but complications such as cup cage migration and non-progressive acetabular lucencies have been noted [8]. The use of trabecular metals is limited by their cost, but these have certain advantages. Potential advantage of trabecular metal is they have increased biocompatibility, allow bone ingrowth and fixation, hence a reasonable option in acetabular bone loss [9]. This helps to circumvent complications related with bone grafts and need of custom made implants or oblong cups [1]. In one of the studies acetabular defect was managed by trabecular acetabular cup, while associated anterior column defect was addressed by sliding iliac bone to construct acetabular column [10]. In the present case, initially, cage was planned for current acetabular defect, but it was found that superior bony ridge prevented sitting of iliac flange of cage on the acetabular margin. Hence, option of trabecular metal wedges and cup was exercised.
Conclusion
The use of CT based 3D printing technology creating 3D pelvic model goes a long way to assess acetabular defects and plan reconstruction preoperatively, leading to increased surgical precision and reduced complications. Pre-operative assessment of defects and planning with tantalum cups and wedges helps in accurate per-acetabular deformity correction to a great extent and provides optimal function.
Clinical Message
Reconstruction of acetabular defects with tantalum cup and augments for Paprosky III A defects is aviable option. The use of 3D printing models preoperatively to assess defects and plan surgeries improves patient outcome and minimizes pre-operative complications.
References
1. Bicanic G, Barbaric K, Bohacek I, Aljinovic A, Delimar D. Current concept in dysplastic hip arthroplasty: Techniques for acetabular and femoral reconstruction. World J Orthop 2014;5:412‐24.
2. Yang S, Cui Q. Total hip arthroplasty in developmental dysplasia of the hip: Review of anatomy, techniques and outcomes. World J Orthop 2012;3:42-8.
3. Charnley J, Feagin JA. Low-friction arthroplasty in congenital subluxation of the hip. Clin Orthop Relat Res 1973;91:98‐113.
4. Andrew J. Hughes AJ, DeBuitleir C, Soden P, O’Donnchadha B, Tansey A, et al. 3D printing aids acetabular reconstruction in complex revision hip arthroplasty. Adv Orthop 2017;2017:8925050.
5. Hurson C, Tansey A, O’Donnchadha B, Nicholson P, Rice J, McElwain J. Rapid prototyp-ing in the assessment, classification and preoperative planning of acetabular fractures. Inju-ry 2007;38:1158-62.
6. Iwase T, Ito T, Morita D. Massive bone defect compromises postoperative cup survivorship of acetabular revision hip arthroplasty with impaction bone grafting. J Arthroplasty 2014;29:2424-9.
7. Buttaro MA, Comba F, Pusso R, Piccaluga F. Acetabular revision with metal mesh, impac-tion bone grafting, and a cemented cup. Clin Orthop Relat Res 2008;466:2482-90.
8. Sculco PK, Ledford CK, Hanssen AD, Abdel M, Lewallen DG. The evolution of the cup-cage technique for major acetabular defects: Full and half cup-cage reconstruction. J Bone Joint Surg Am 2017;99:1104-10.
9. Bobyn JD, Stackpool GJ, Hacking SA, Tanzer M, Krygier JJ. Characteristics of bone in-growth and interface mechanics of a new porous tantalum biomaterial. J Bone Joint Surg Br 1999;81:907-14.
10. Wada K, Goto T, Takasago T, Tsutsui T, Sairyo K. Acetabular reconstruction using a tra-becular metal cup with a novel pelvic osteotomy technique for severe acetabular bone de-fect. Case Rep Orthop 2018;2018:9015727.
 |
 |
 |
 |
 |
 |
| Dr. Bharath Loganathan | Dr. Vipin Sharma | Dr. MuthukumaranRavi Kumar | Dr. Sivamurugan Soundarapandian | Dr. Dhiraj Prem Sukh Marothi | Dr. Kavya Sharma |
| How to Cite This Article: Loganathan B, Sharma V, Ravikumar M, Soundarapandian S, Marothi DP, Sharma K. Acetabulum Reconstruction with Tantalum Cup and Augments in Dysplastic Hip Type 4 using 3D Printing Technology. Journal of Orthopaedic Case Reports 2020 October;10(7): 18-21. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


