
 [box type=”bio”] Learning Point of the Article: [/box]
[box type=”bio”] Learning Point of the Article: [/box]
Osteoid osteoma can occur in any bone at any location so be careful in assessment of imaging examination and exact intraoperative localization of lesion.
Case Report | Volume 10 | Issue 9 | JOCR December 2020 | Page 102-105 | Vaibhav R Gandhi, Saseendar Shanmugasundaram. DOI: 10.13107/jocr.2020.v10.i09.1922
Authors: Vaibhav R Gandhi[1], Saseendar Shanmugasundaram[2]
[1]Department of Orthopaedic, Sudarshan Orthocare Hospital, Aurangabad, Maharashtra, India.
[2]Department of Orthopaedic, Apollo Hospital, Muscat, Sultanate of Oman.
Address of Correspondence:
Dr. Vaibhav R Gandhi,
Department of Orthopaedic, Apollo Hospital, Muscat, Sultanate of Oman.
E-mail: drvaibhavg@yahoo.com
Abstract
Introduction: Osteoid osteoma is a benign osteoblastic bone tumor that mostly arises from the long bones. The acetabulum is a rare site for osteoid osteoma. Moreover, juxta-articular location of the lesion can be associated with delayed diagnosis. We present a case of a juxta-articular osteoid osteoma of the acetabulum that was missed earlier. We also present a novel, easy, and cost-effective way to accurately localize and excise such a lesion, thereby avoiding failure and recurrence.
Case Report: A 15-year-old female presented with a history of insidious onset pain in the right hip for 18 months. Pain was diffuse over the hip. She had undergone a failed biopsy in another hospital. She visited us 1 month later with persistent pain. Examination revealed tenderness over the right anterior hip joint line with painful terminal hip flexion. Computed tomography (CT) suggested an osteoid osteoma of the superolateral acetabular rim. The patient was planned for CT-guided mini-open excision biopsy of the lesion. CT-guided localization of the lesion was performed under local anesthesia in the CT room, followed by open excision of the nidus in the operating room. Histopathology confirmed the diagnosis and a complete excision. At last follow-up at 1 year, the patient was asymptomatic and returned to normal function.
Conclusion: Osteoid osteoma of the acetabulum is uncommon and the diagnosis is usually delayed. A high index of suspicion is needed to avoid a missed diagnosis and CT-guided approach can help in accurate excision. Our technique to localize and completely excise the lesion is novel, simple, and cost effective and can be easily replicated.
Keywords: Osteoid osteoma, Acetabulum, Computed tomography-guided excision, Delayed diagnosis, Missed diagnosis, Periarticular osteoid osteoma.
Introduction
Osteoid osteoma, as described by Jaffe in 1935, is a benign lesion [1] that usually affects young adults. It predominantly affects the appendicular skeleton, especially the femur and the tibia [2]. The presence of this condition has been reported in practically all the bones of the skeleton, including the cranium, face, and spine. It rarely occurs in the pelvis; just 1–3% of all cases are located in this region [3], with majority of pelvic lesions being found in the acetabulum [4]. Juxta-articular localizations frequently are associated with a delayed diagnosis, as seen in our patient [5]. Osteoid osteoma macroscopically is characterized by a friable vascular nidus with sandy consistency and peripherally by sclerotic bone in association with thick vascular periosteum. An articular inspection in juxta-articular osteoid osteoma usually reveals no labial lesions or loose bodies or synovitis [6]. Osteoid tissue along with vascular stroma surrounded by dense bone is microscopic appearance of nidus. The diagnosis can be made by means of simple radiography in 75% of the cases. Radio transparent small oval or rounded focus comprising a nidus is usually seen on imaging. Reactive bone sclerosis is seen around nidus which in particular occasion can be very intense, leading to difficulty in imaging correctly. Hence, specialized imaging studies, such as computed tomography (CT), magnetic resonance imaging (MRI), or bone scintigraphy, can be used to determine the exact location of lesion. The peculiar clinical presentation is pain, predominantly nocturnal, which can be correlated with of increased synthesis of prostaglandins triggered by the lesion [7]. Nonsteroidal anti-inflammatory drugs (NSAIDs) by blocking prostaglandin synthesis give temporary pain-free spells. Mostly, lesion is painful symptomatically. Regarding their location within the bone, subperiosteal, intracortical, endosteal, and intramedullary lesions can be identified, in which intramedullary lesions are the least common. We present a report on osteoid osteoma in an unusual location that was missed clinically, radiologically, and from attempted biopsy. We also present an easy and cost-effective way of accurately localize and excise the lesion, thereby avoiding failure and recurrence. Reference is also made to the importance of the differential diagnosis in this case.
Case Report
A 15-year-old female presented with insidious onset, pain in the right hip for 18 months. Pain was diffuse over the hip, especially on the anterior aspect, radiating to the knee and was relieved by oral NSAIDs. For 6 months, the pain had become more severe, especially during the night, and was not relieved by oral analgesics. Primary surgeon advised her MRI scan. Taking help of MRI scan report, primary surgeon performed open biopsy from iliac crest as MRI showed signal changes in whole iliac bone. However, the biopsy report revealed no pathological cells.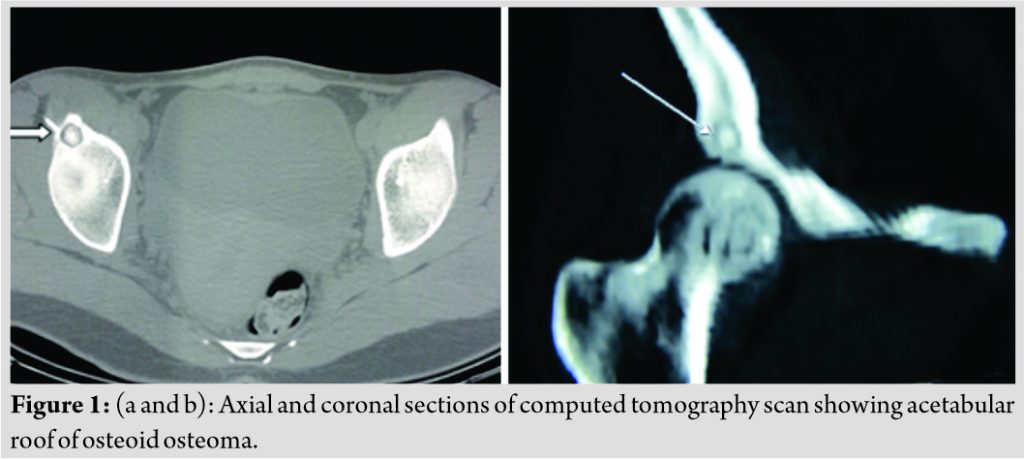
The patient visited our institute 1 month after the primary biopsy procedure with persistent pain. On examination, there was tenderness over the right anterior hip joint line with pain on terminal hip flexion. Her blood parameters including total leukocyte count, erythrocyte sedimentation rate, and C-reactive protein were normal. Radiograph of the pelvis with both hips – anteroposterior view showed sclerosis in supra-acetabulum region. CT revealed a central area of sclerosis surrounded by osteolysis in the right ilium along the superolateral acetabular rim, most likely suggesting an osteoid osteoma. Considering the persistent pain that was not relieved with analgesics, the patient was planned for CT-guided mini-open excision biopsy of the lesion (Fig. 1a, b, 2a, b, c).
Surgical procedure
Under CT guidance, an 18-gauge spinal needle passed onto the lesion under local anesthesia under aseptic precautions. The patient was subsequently shifted to the operating room and under spinal anesthesia a mini-open Smith Peterson approach was used to expose the lesion. The lesion was drilled, the nidus was excised and sent for histopathologic examination (HPE) and the margins of the lesion were curetted. A through wash was performed and the surgical wound was closed in layers. Postoperatively, the patient recovered uneventfully. She was advised non-weight-bearing walking for 3 weeks followed by progressive full weight-bearing.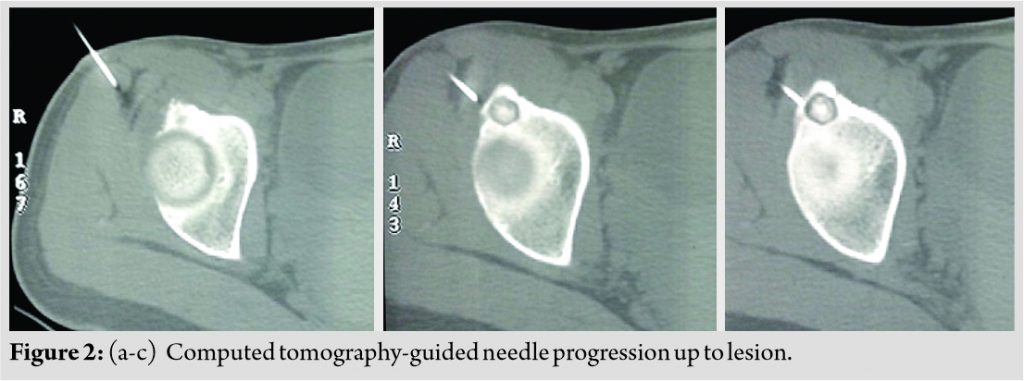
HPE revealed the characteristic appearance of an osteoid osteoma with differentiated osteoblasts lining the osteoid and interconnected trabeculae of woven bone (Fig. 3a, b). The patient improved dramatically with complete pain relief in few days after surgery. The patient was last available for physical follow-up at 1 year postoperatively, when she was completely asymptomatic with normal gait (Fig. 4). The patient was last consulted over a phone call at 4 years postoperatively and she remained to be asymptomatic and had returned to normal physical activity.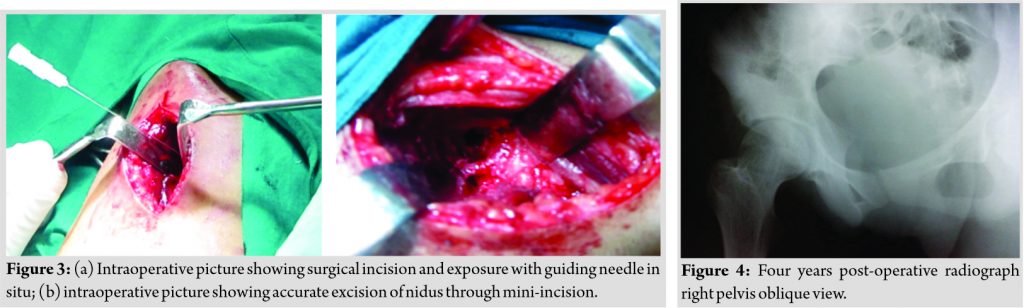
Discussion
In the cases reported here, the patients consulted several specialists and operated with open iliac biopsy. As biopsy site was missed which lead to delayed diagnosis and patient’s pain increased and intake of analgesics increased. Pain kept on increasing affecting activity of daily living. The patient had to bear excessive financial cost of failed biopsy and also delay in treatment. Our method not only gave accurate diagnosis but also accuracy of surgical procedure was highest for adequate excision of juxta-articular lesion in acetabulum region. A confirmed diagnosis was achieved, proven with support of histopathological analysis. Surgical cost of surgery with intraoperative CT scan facility can be around 10 times more than cost of our surgical technique. Radiofrequency ablation probe also has very high cost with associated tissue damage in juxta-articular area.
While considering the differential diagnosis of articular pain which is peculiarly insidious and nocturnal in long duration and alleviated by salicylates and NSAIDs, then the diagnostic hypothesis of osteoid osteoma can be evident. The lesion can be confirmed by CT [8] and MRI [9] when conventional radiographic examination indicates possibility of bony lesion and they are useful for surgical planning. In one of research studies, only 14 reports on cases of osteoid osteoma located in the iliac bone between 1945 and 2014 were seen. Some studies document spontaneous cure of lesion. Although some degree of bone sclerosis remained, the pain and radiological findings were observed to gradually disappear. Surgical intervention is indicated as natural history of this disease is unpredictable and long duration. Radiofrequency ablation guided by CT is an alternative that has been used with very promising results, especially in regions that are difficult to access through conventional surgery [10]. However, the cost of the infrastructure and the therapy limits availability in certain institutions and restricts accessibility for poor patients. During radiofrequency ablation process, cannula and probe fractures are seen and sometimes these intraosseous fractures can remain in the bone [11]. Furthermore, the risk of thermal damage to cartilage needs to be considered. Nevertheless, some patients have recurrences after radiofrequency ablation [12]. Similar risks exist for cryoablation and laser thermocoagulation. Trephine biopsy was not an option in this patient with lesion very close to the articular cartilage due to the fear of violation of the subchondral bone and the articular cartilage. The literature indicates that the preferred treatment is en bloc surgical resection, including the nidus [13]. Consequently, crucial for the success of the intervention is determining the exact location of the nidus during the operation. En block surgical excision was not possible due to proximity to hip joint. Hence, curettage and nidus excision which were done in the present case using pre-operative CT-guided needle technique (Fig. 5).
Conclusion
Osteoid osteoma can occur in any bone at any location so we need to be careful in assessment of imaging examinations and recognition of the importance of the clinical condition. Involvement of the iliac bone is less common, and osteoid osteoma in unusual locations generally leads to late diagnosis. In the case reported here, CT-guided localization and surgical curettage of the lesion were shown to be a cost effective and safe method, as reported in the literature.
Clinical Message
Outpatient-based CT-guided localization of osteoid osteoma can be a cost-effective way to increase accuracy of excision of juxta-articular lesion.
References
1. Broadfoot J. The use of computed tomography in diagnosis of osteoid osteoma. Australas Radiol 1988;32:463-7.
2. Assoun J, Railhac JJ, Bonnevialle P. Osteoid osteoma: Percutaneous resection with CT guidance. Radiology 1993;188:541-7.
3. Ruggieri P, Gasbarrini A, Ferraro A. Osteoid osteoma. Direct visual identification and intralesional excision of the nidus with minimal removal of bone. J Bone Joint Surg Br 1999;81:814-20.
4. Ishikawa Y, Okada K, Miyakoshi N, Takahashi S, Shimada Y, Itoi E. Osteoid osteoma of the scapula associated with synovitis of the shoulder. J Shoulder Elbow Surg 2005;14:329-32.
5. Foeldvari I. Rapid development of severe osteoarthritis associated with osteoid osteoma in a young girl. Clin Rheumatol 1998;17:534-7.
6. Malavolta EA, Assunção JH, Rebolledo DC, Gracitelli ME, Correia LF, Ferreira Neto AA, et al. Osteoid osteoma of the glenoid: Arthroscopic treatment. Orthop Traumatol Surg Res 2015;101:977-80.
7. Greco F, Tamburrelli F, Ciabattoni G. Prostaglandins in osteoid osteoma. Int Orthop 1991;15:35-7.
8. Sans N, Galy-Fourcade D, Assoun J, Jarlaud T, Chiavassa H, Bonnevialle P, et al. Osteoid osteoma: CT-guided percutaneous resection and follow-up in 38 patients. Radiology 1991;212:687-92.
9. Davies M, Cassar-Pullicino VN, Davies MA, McCall IW, Tyrrell PN. The diagnostic accuracy of MR imaging in osteoid osteoma. Skeletal Radiol 2002;31:559-69.
10. Cioni R, Armillotta N, Bargellini I, Zampa V, Cappelli C, Vagli P. CT-guided radiofrequency ablation of osteoid osteoma: Long-term results. Eur Radiol 2004;14:1203-8.
11. Kilinc BE, Sahin C, Boyacioglu MM, Ertugrul R, Varol A. Complications of computer tomography assisted radiofrequency ablation in the treatment of osteoid osteoma. Biomed Res Int 2019;2019:4376851.
12. Albisinni U, Facchini G, Spinnato P, Gasbarrini A, Bazzocchi A. Spinal osteoid osteoma: Efficacy and safety of radiofrequency ablation. Skeletal Radiol 2017;46:1087-94.
13. Kronbauer FL, Ortiz R, Kronbauer AL, Zylbersztejn S. Osteoma osteoide no osso iliaco: Relato de caso. Rev Bras Ortop 1997;32:985-8.
 |
 |
| Dr. Vaibhav R Gandhi | Dr. Saseendar Shanmugasundaram |
| How to Cite This Article: Gandhi VR, Shanmugasundaram S. A Missed Case of Osteoid Osteoma of the Acetabulum Treated with a Novel Computed Tomography-Guided Technique – A Case Report. Journal of Orthopaedic Case Reports 2020 December;10(9): 102-105. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


