
TENS nailing with wedge osteotomy can be used as a procedure for definitive management in cases of monostotic FD of the tibia, with meticulous pre-operative planning, and execution.
Dr. Mrinal Kambli,
Department of Orthopaedics, Grant Medical College and Sir J.J. Group of Hospitals,
Byculla, Mumbai, Maharashtra, India.
E-mail: kambli.mrinal@gmail.com
Introduction: Titanium elastic nailing (TENS) with wedge osteotomy for the management of monostotic fibrous dysplasia (FD) of tibia is done in a 6-year-old male patient.
Case Report: This is a case describing monostotic FD of right tibia in a 6-year-old male patient. The patient’s parents noticed a diffuse swelling in the right leg a few days after birth. It was managed conservatively till 3 years of age when the patient started complaining of pain in his right leg and difficulty in walking and running. The patient developed gradual and progressive anterior bowing in the right leg in the next 3 years. The patient was diagnosed with monostotic FD of the right tibia based on clinical and radiological findings. Wedge osteotomies were done in the tibia and fibula with TENS nailing as a definitive procedure for this patient.
Discussion: Management of monostotic FD of the right tibia with TENS nailing and wedge osteotomy can be a possible modality of definitive management with complete pain relief and deformity correction.
Conclusion: Correction of deformities secondary to FD requires meticulous pre-operative planning and execution. But with proper planning, even major deformities as in our case, procedures as simple as wedge osteotomy and TENS nailing can give excellent outcomes.
Keywords: Fibrous dysplasia, monostotic, titanium elastic nailing.
Fibrous dysplasia (FD) is a disorder consisting of a developmental defect in osteoblast differentiation and bone maturation [1]. It develops during childhood with tumor-like lesions manifesting typically during adolescence and early adulthood. Treatment of FD is difficult due to its varied presentations such as severe deformities, pain, pathological fractures, and high chances of recurrence [2]. There are no clear guidelines for its management. The treatment modality or decision for surgery varies from case to case and decided by individual surgeons accordingly. In this case, the focus was on correcting the deformity and providing early recovery as well as ambulation.
Here we present the case of a 6-year-old male with chief complaints of pain, swelling, and deformity in the right lower limb with difficulty in walking. History was given by the patient’s parents. They denied any history of trauma. The patient’s parents had noticed a localized swelling in right lower limb few days after birth. It was managed conservatively till 3 years of age when After 3 years the patient started complaining of pain in his right leg and difficulty in walking and running. The patient developed gradual and progressive anterior bowing in the right leg over the next 3 years. On examination of the right leg, the patient had a diffuse swelling with anterior bowing deformity (Fig. 1).
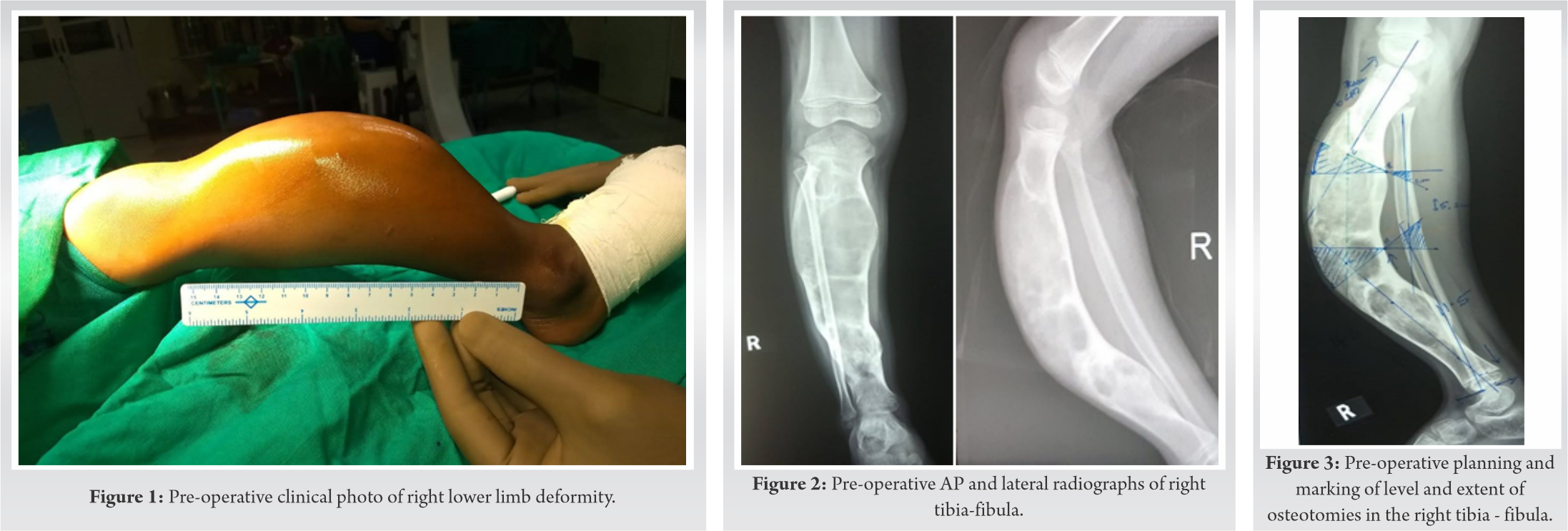
No similar lesions were seen anywhere else in the body or in any sibling. No areas of abnormal pigmentation or precocious puberty were seen. Anteroposterior and lateral radiographs were ordered for bilateral lower limbs (Fig. 2). Radiographs for the left lower limb were normal. Radiographs of right tibia fibula showed multiple osteolytic lesions with cortical thinning in tibia; on basis of which provisional diagnosis of monostotic FD was established. The decision for surgery taken with proper preoperative discussion and planning to avoid any intra-operative or post-operative complications (Fig. 3).
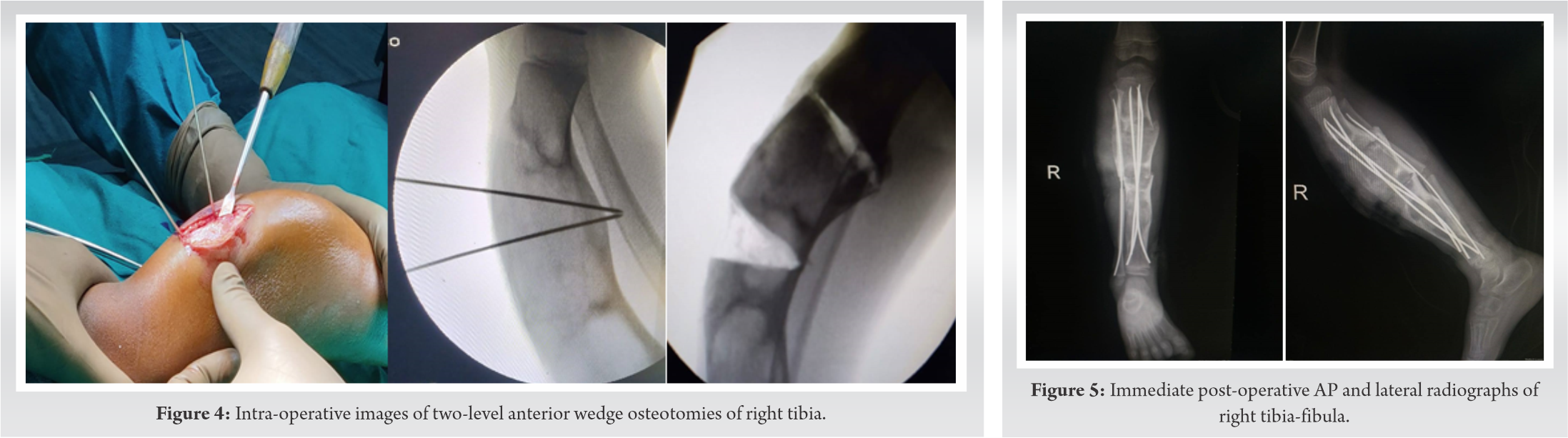
Patient placed in a supine position on the operating table. The incision was taken in anterior midline 6 cm from the knee joint. 2 cm wedge resected and closed wedge osteotomy done as planned preoperatively. The incision for the 2nd wedge osteotomy taken 5 cm distal to the proximal site 3.5 cm wedge resected and closed wedge osteotomy performed at this site (Fig. 4). 3 titanium elastic nailing (TENS) nail (2.5 mm) inserted from distal entry site just proximal to the epiphysis and passed from distal to the proximal site.
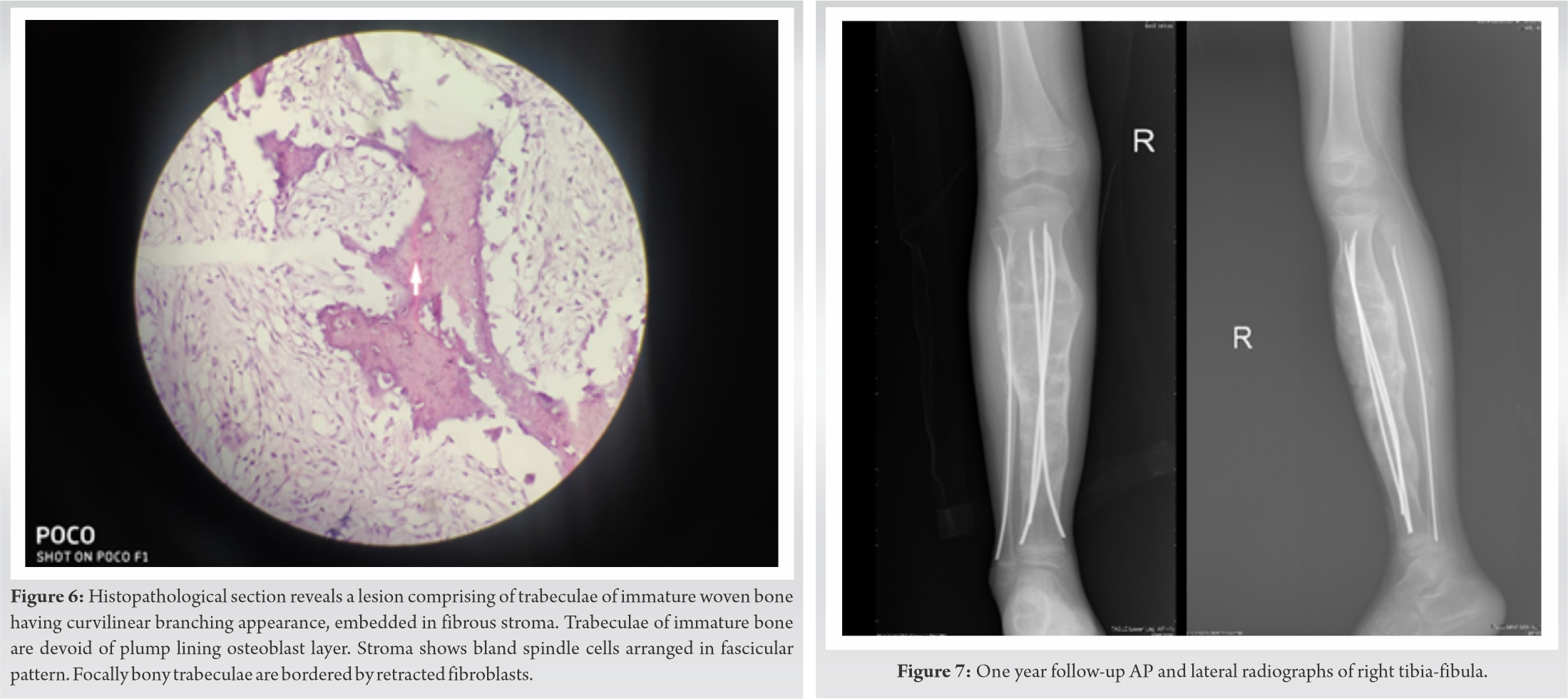
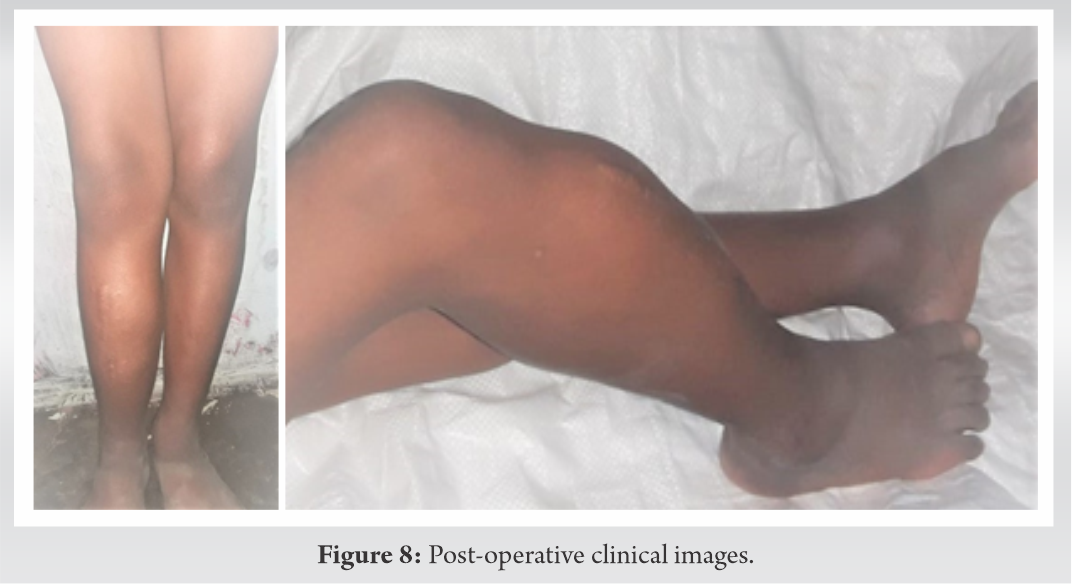
Fibular osteotomy is done at the midshaft level and a single tens nail of 1.5 mm inserted through the distal entry site just proximal to the epiphysis and passed from distal to the proximal site (Fig. 5). Tissue samples collected and sent for histopathological examination on the basis of which confirmatory diagnosis of FD was established (Fig. 6). Closure done in layers and sterile dressing done. Above knee slab given in the extension. The patient advised nil weight-bearing for 4 weeks. Static quadriceps strengthening exercises, active and passive hip range of motion exercises started immediately on post-operative day 2. Wound check is done on post-operative day 2 and suture removal was done on day 12 post-operative. After 4 weeks, above knee slab removed and the clamshell brace was given. The patient started assisted walk with a walker with partial weight bearing on the affected limb for 4 weeks. Hip, knee, and ankle range of motion exercises started. After 8 weeks of post-operative full weight bearing walk started. Now, a year post-operative patient can walk unassisted and has no pain and deformity. Clinical as well as radiological follow-up showed correction of the deformity with a good union at all the three osteotomy sites (Fig. 7). The range of motion is free and full in the right hip, knee, and ankle (Fig. 8).
FD is a disorder consisting of a developmental defect in osteoblast differentiation and bone maturation. The term FD was coined by Lichtenstein in 1938 [3]. Lichtenstein and Jaffe described FD in a larger case series in 1942 [4]. It consists of single or multiple foci of fibrous tissue composed of irregular bone trabeculae. FD consists of 7% of benign bony lesions [5]. FD can be classified into two types: Monostotic, involving single bone, and polyostotic, consisting of multiple lesions in different bones. Polyostotic variety may affect one or multiple extremities and is known to be associated with multiple endocrine disorders including hyperthyroidism, hypophosphatemia, acromegaly, hyperprolactinemia, and Cushing’s disease [6]. Monostotic variety is more common as compared to a polyostotic variety [7]. It occurs due to a mutation in the GNAS1 gene at chromosome 20q13.2–13.3, which encodes for the alpha-subunit of a stimulatory G protein [8]. The disorder is not inherited as the mutation occurs after fertilization of somatic cells. FD is also a characteristic of McCune-Albright syndrome (polyostotic FD, café-au-lait spots, and endocrine dysfunction) and Mazabraud’s syndrome (polyostotic FD and soft-tissue myxomas) [9, 10]. The long bones involve in FD have a greater tendency for pathological fractures [11]. However, no definite criteria have been established to identify patients at high risk for pathological fractures [12]. Some form of intervention becomes necessary to avoid such pathological fractures. Management options include closed fixation, internal fixation or curettage, and bone grafting. Conservative treatment is usually recommended for adolescents as the majority of lesions of FD cease to develop or progress following adolescence except for lesions of McCune Albright syndrome [13]. Curettage and bone grafting may be done in an attempt to eradicate the lesion and prevent further deformity. However, the lesions have a tendency to recur. Furthermore, curettage may cause further weakening of the bone and may itself result in pathological fractures [14]. By far the most superior outcomes have been obtained with internal fixation [15]. It is generally accepted that monostotic lesions necessitate fewer surgeries and are associated with better outcomes [16]. Our case report describes the use of two wedge osteotomies to correct the anterior bow of the tibia and the use of TENS nail for internal fixation which has seldom been done. The outcome was favorable with the cessation of pain for the patient as well as early and full return to physical activity.
TENS nailing with wedge osteotomy can be used as a procedure for definitive management in cases of monostotic FD of the tibia, with meticulous pre-operative planning, and execution. Precise, pre-planned anterior closed wedge two-level osteotomies allow for deformity correction, and the use of TENS nails allows for a minimally invasive approach that provides relative stability to both tibia and fibula at the site of osteotomies. This allows for satisfactory outcomes, early ambulation, and rehabilitation in such patients.
TENS nailing with wedge osteotomy can be used as a primary and definitive modality of treatment in cases of monostotic FD of right tibia.
References
- 1.Rosado ER, Ortiz EH, Aponte CL, Ortiz PV. Bilateral tibia fibrous dysplasia in a pediatric patient treated with intramedullary nailing: A case report. Bol Asoc Med P R 2016;108:23-5. [Google Scholar]
- 2.Guille JT, Kumar SJ, MacEwen GD. Fibrous dysplasia of the proximal part of the femur. Long-term results of curettage and bone-grafting and mechanical realignment. J Bond Joint Surg Am 1998;80:648-58. [Google Scholar]
- 3.Lichtenstein L. Polyostotic fibrous dysplasia. Arch Surg 1938;36:874-98. [Google Scholar]
- 4.Lichtenstein L. A condition affecting one, several or many bones, the Graver cases of which may present abnormal pigmentation of skin, premature sexualdevelopment, hyperthyuroidism or still other extra-skeital abnormalities. Arch Pathol 1942;33:777-816. [Google Scholar]
- 5.Campanacci M. Bone and Soft Tissue Tumors: Clinical Features, Imaging, Pathology and Treatment. Berlin: Springer Science and Business Media; 2013. p. 11866. [Google Scholar]
- 6.Parekh SG, Rao DR, Ricchetti E, Lackman RD. Fibrous dysplasia. J Am Acad Ortho Surg 2004;12:305-13. [Google Scholar]
- 7.Smith SE, Kransdorf MJ. Primary musculoskeletal tumors of fibrous origin. Semin Musculoskelet Radiol 2000;4:73-88. [Google Scholar]
- 8.Chapurlat RD, Meunier PJ. Fibrous dysplasia of bone. Best practice Res Clin Rheumatol 2000;14:385-98. [Google Scholar]
- 9.Wirth WA, Leavitt D, Enzinger FM. Multiple intramuscular myxomas. Another extraskeletal manifestation of fibrous dysplasia. Cancer 1971;27:1167-73. [Google Scholar]
- 10.Blasier RD, Ryan JR, Schaldenbrand MF. Multiple myxomata of soft tissue associated with polyostotic fibrous dysplasia: A case report. Clin Orthop Relat Res 1986;206:211-4. [Google Scholar]
- 11.Enneking WF, Gearen PF. Fibrous dysplasia of the femoral neck. Treatment by cortical bone-grafting. J Bone Joint Surg Am 1986;68:1415-22. [Google Scholar]
- 12.DiCaprio MR, Enneking WF. Fibrous dysplasia: Pathophysiology, evaluation, and treatment. J Bone Joint Surg Am 2005;87:1848-64. [Google Scholar]
- 13.Kusano T, Hirabayashi S, Eguchi T, Sugawara Y. Treatment strategies for fibrous dysplasia. J Craniofac Surg 2009;20:768-70. [Google Scholar]
- 14.Grabias SL, Campbell CJ. Fibrous dysplasia. Orthop Clin North Am 1977;8:771-83. [Google Scholar]
- 15.Keijser LC, Van Tienen TG, Schreuder HB, Lemmens JA, Pruszczynski M, Veth RP. Fibrous dysplasia of bone: Management and outcome of 20 cases. J Surg Oncol 2001;76:157-66. [Google Scholar]
- 16.Funk JF Jr., Wells RE. Hip problems in fibrous dysplasia. Clin Orthop Relat Res 1973;90:77-82. [Google Scholar]








