
Apart from usual complications like pin track infection, non union or stiffness, one must be vigilant and aware about over distraction at PIP joint which can cause vascular compromise in digit while treating volar lip fracture with Pins and Rubber traction system.
Dr. Sanket Tanpure,
DNB Orthopaedic Resident at Jupiter Lifeline Hospital, Thane, Maharashtra, India.
E-mail: sankettanpure55@gmail.com
Introduction: The management of acute proximal interphalangeal (PIP) joint fracture-dislocation by dynamic external fixator is widely practiced method. The complications such as pin loosening or non-union or stiffness are known and can be treated well. The over distraction causing vascular compromise and calcification of volar plate jeopardizing the function and viability of the affected digit is not reported so far.
Case Report: We report a case of 2 weeks post-traumatic ring finger PIP joint fracture-dislocation in a 21-year-old male which was treated by pins and rubber dynamic traction method. The affected digit was found cold and lengthened at 3 weeks of distraction causing vascular compromise. The X-ray showed over distraction by 1.5 cm at PIP joint. The digit was salvaged by removing distractor and applying splintage. Later, at 6 weeks, X-ray showed volar plate calcification causing joint stiffness. This was tackled by volar plate arthroplasty. At 2 months, the patient got 20–80° movement without pain.
Conclusion: The dynamic pins and rubber traction system for acute PIP joint injury can result in complication like over distraction leading vascular compromise. The clinical and radiological assessment with such technique is mandatory once a week to avoid missing such disasters. Even if such complication occurs, immediate fixator removal and splintage can save the digit. Once it survives, secondary procedure for gaining movement or stabilizing the joint like volar plate arthroplasty can be considered.
Keywords: Pins and Rubbers traction system, Over distraction, Vascular compromise
Acute proximal interphalangeal joint injuries in digits are very common [1]. Based on involvement of volar lip fracture and dislocation, various modalities of treatment have been described. Dynamic distraction based on the capsulo-ligamentotaxis principle is popular among all and has the advantage of starting an early active range of movement in the PIP joint.
One of the described methods is pins and rubbers traction system.
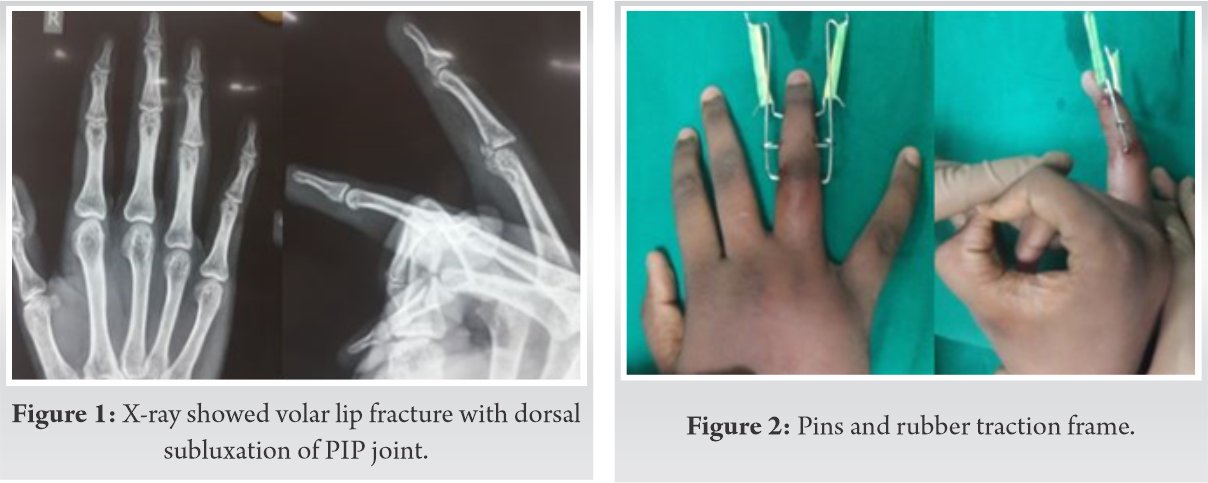
A 21-year-old male right hand dominant student got a cricket ball injury to the right ring finger. He presented to us 15 days post-injury with pain and inability to move the proximal interphalangeal joint (PIPJ) in the right ring finger. His radiograph showed volar lip fracture with dorsal subluxation of the PIP joint. The volar fragment involvement was <30% (Fig. 1). We performed for dynamic distraction frame called “pins and rubbers traction system” application under local anesthesia so that he could start early active movement. Postoperatively, the pins and rubber traction frame was well placed and did not hamper other digits activities (Fig. 2). The X-ray showed excellent PIP joint reduction and good alignment of the volar lip fragment (Fig. 3).
Post-surgery, from day 1, we advised him to do active movement at the PIP joint in the ring finger 5 times every four hourly.
Fifteen days post-surgery, though he had 20°–70° movement in the PIP joint, he noticed lengthening of his digit as compared to the left ring finger but did not inform to author. At 3 weeks after surgery, the patient felt that fingertip was colder and less sensate than other digits and the length of the ring finger was same as the middle finger of same hand.
At this point, the patient was called to the emergency department where author confirmed vascular compromise in the digit and got his X-ray radiography done. The author noticed more than 1.5 cm of over distraction in the PIP joint (Fig. 4). The distractor frame was immediately removed in the casualty, and the patient was given a static finger extension splint.

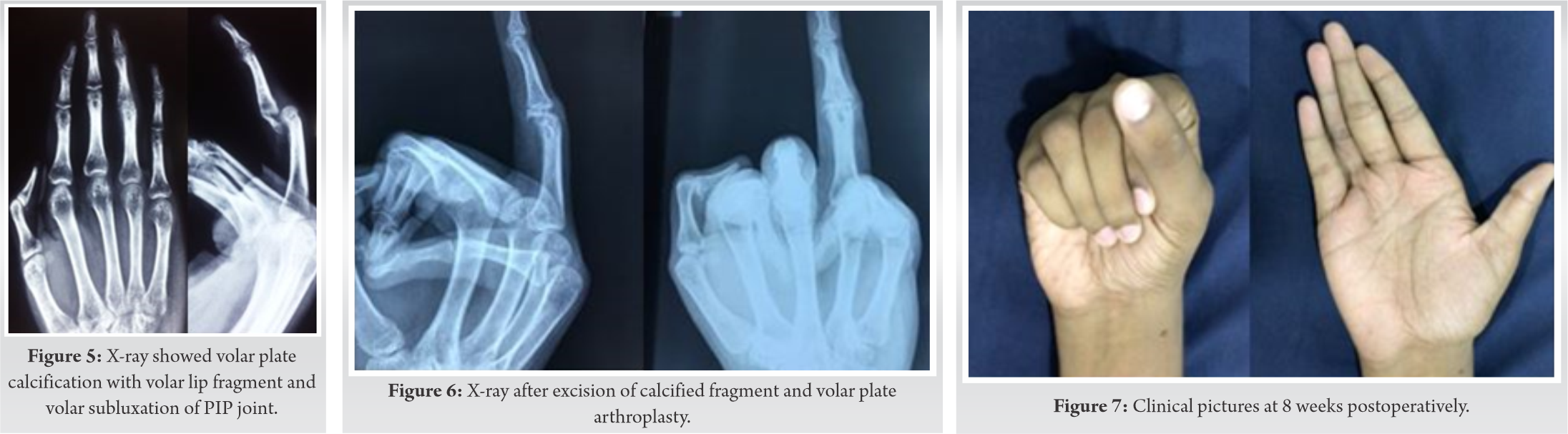
After 1 week of frame removal, reexamination was done. The finger was vascular (capillary filling of <2 s) and sensate (2-point discrimination of 4 mm). The length of the digit was near normal as the left ring finger. The PIP joint was flail, probably because of over stretching of the collateral ligaments. The active range of movement was from 20° to 40°. After 6 weeks, X-ray was repeated, which showed volar plate calcification with volar lip fragment and volar subluxation of the PIP joint (Fig. 5).
Patients were given the option of PIPJ joint arthrodesis or to consider volar exploration, excision of calcified fragment, and volar plate arthroplasty with guarded prognosis.
We performed excision of calcified fragment and volar plate arthroplasty (Fig. 6).
The patient was advised to start range of movement exercises after 2 weeks. At 8 weeks post-operative period, the patient regained 20–90 degree movement in the PIP joint of the ring finger without pain (Fig. 7).
Treatment methods, analysis of fracture and results in metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints was studied extensively by H Hastings in 1988 and proved that displacement of fracture and joint incongruency was better tolerated by MCP joints rather that PIP joints [2]. Many times, PIP joint injuries are treated with complete casualness by surgeons. Because of this, patients may land up in compromised functional outcome and persistent impairment [3]. Because of hyperextension injury, the volar plate can get avulsed from its insertion site at the middle phalanx base. These avulsion fragments can be small tiny bony pieces to large fragments of bone, which can form one-third of the articular surface [3].
Dorsal block pinning for acute PIP joint fracture with dislocation was described as simple method of treatment based on stable arc splinting and early protective motion [4]. Compromised treatment has proven to give suboptimal result in fractures around PIP joint. In recent years, percutaneous screw fixation with dynamic external fixators have also given good results in such injuries as described by Liodaki E et al [5]. Dynamic distractor frame based on principles of capsule ligamentotaxis for PIPJ fracture dislocation is safe and routinely performed surgery. It has the advantage of starting range of movement exercises postoperatively at the earliest. Suzuki frame (P & R traction system) is very compact, easy to apply, and can be applied for acute as well as less than 3 weeks old injury around PIPJ [6]. Complications such as pins loosening, infection, recurrent subluxation, rotation malalignment, osteoarthritis, malunion, and osteophyte formation are well studied in a systematic review done by Hamilton [1]. In Inanami series of seven patients treated with a dynamic distractor published in 1993, he mentioned only one complication of persistent pain due to recurrence of subluxation with 1 mm PIP joint discrepancy [7]. Even Suzuki in his series of seven patients mentioned no complications, except one patient had occasional pain in PIPJ [6]. However, capsule ligamentotaxis causing such fearful distraction has not been published so far. The pins and rubber traction system (PRTS) is very effective method of treatment in cases of pathological fractures around PIP joint, incomplete amputation around PIP joint, and osteochondral defect in head of proximal phalanx [8].
We must warn the patient to have regular follow-up to avoid such dreaded complication. We recommend keeping a close watch on the length of the finger and check for pin sites to diagnose over distraction. We should also take X-rays at least once in 10 days.
The reason for over distraction in our case could be that too many rubber bands attached to both wires hook and too many repetitions of the attempt of movement at the PIP joint. In spite of such complication, appropriate waiting and then considering the secondary procedure followed by rehabilitation gave a better outcome in this case. There should be guidelines about the number of rubber bands or type of rubber bands to be attached and number of attempts of PIP joint mobilization.
Apart from pin tract infection, stiffness, and malunion, over distraction in the dynamic distractor frame for PIP joint fracture dislocation should be looked as one of the complications. The regular follow-up for clinical and radiological assessment is necessary at least once in ten days.
If over distraction is missed, there is a possibility of dreadful complications such as digital ischemia and lengthening of the digit, especially if pathology in the ring finger.
If we diagnose early, then this complication can be treated by analyzing the problem, removing the distractor and later secondary salvage procedures such as volar plate arthroplasty or arthrodesis if required.
The dynamic distractor frame for PIP joint fracture dislocation is an easy and doable procedure. To avoid stiffness, patients are asked to move the joint regularly, but must be warned about the possibility of over distraction. From a clinician point of view, these patients have to come for regular follow-up for clinical assessment such as lengthening of the digit as compared to the opposite side, neurovascular compromise, skin laceration near the pin tract site, and X-ray finding of over distraction.
No fractures in the hand are simple to treat. All intra-articular fractures need very meticulous planning, regular follow-up, and quick action to avoid mishaps.
References
- 1.Hamilton LC. The acute management of unstable intra-articular fractures of the base of the middle phalanx: A systematic review. J Hand Surg Asian Pac 2018;23:441-9. [Google Scholar]
- 2.Hastings H, Carroll C. Treatment of closed articular fractures of the metacarpophalangeal and proximal inter-phalangeal joints. Hand Clin 1988;4:503-27. [Google Scholar]
- 3.Kiefhaber TR, Stern PJ. Fracture dislocations of the proximal interphalangeal joint. J Hand Surg Am 1998;23:368-80. [Google Scholar]
- 4.McElfresh EC, Dobyns JH, O’Brien ET. Management of fracture-dislocation of the proximal interphalangeal joints by extension-block splinting. J Bone Joint Surg Am 1972;54:1705-11. [Google Scholar]
- 5.Liodaki E, Xing SG, Mailaender P, Stang F. Management of difficult intra-articular fractures or fracture dislocations of the proximal interphalangeal joint. J Hand Surg Eur 2015;40:16-23. [Google Scholar]
- 6.Suzuki Y, Matsunaga T, Sato S, Yokoi T. The pins and rubbers traction system for treatment of comminuted intra-articular fractures and fracture-dislocations in the hand. J Hand Surg Br 1994;19:98-107. [Google Scholar]
- 7.Inanami H, Ninomiya S, Okutsu I, Tarui T. Dynamic external finger fixator for fracture dislocation of the proximal interphalangeal joint. J Hand Surg 1993;18A:160-4. [Google Scholar]
- 8.Nanno M, Kodera N, Tomori Y, Takai S. Pins and rubbers traction system for fractures of the proximal interphalangeal joint. J Orthop Surg (Hong Kong) 2019;27:2309499019840771. [Google Scholar]





