
We describe a case of treated unstable pelvic ring injury using a dual internal anterior subcutaneous fixator we called “dual INFIX”, comprising 4 screws, 2 subcutaneous rods, and 2 cross link connectors, without posterior fixation.
Dr. Takeshi Sasagawa,
Department of Orthopedics Surgery, Toyama Prefectural Central Hospital, 2-2-78 Nishinagae,
Toyama city, Toyama Prefecture, 930-8550, Japan.
E-mail: sasagawawagasasa@yahoo.co.jp
Introduction: External fixation, various subcutaneous screw fixations, and plate fixation can be considered as fixation methods for unstable pelvic ring fractures. We describe a first case of treated unstable pelvic ring injury using a dual internal anterior subcutaneous fixator we called “dual INFIX,” comprising four screws, two subcutaneous rods, and two cross-link connectors, without posterior fixation.
Case Report: An 81-year-old man sustained an unstable pelvic injury (AO type B2) with fracture of the left ilium and pubis. Dual INFIX was used to stabilize the pelvic ring injury. Polyaxial screws were introduced along a path between the anterior inferior iliac spine and ipsilateral posterior superior iliac spine until the head of the screw lay immediately above the fascia. Bilateral cranial screws were connected by a rod passed subcutaneously, and caudal screws were connected by the other rod. Finally, cross-link connectors connected cranial and caudal rods on the right and left. One year after the first operation, the patient could walk without a cane and had no limitation of daily living and bony fusion was achieved.
Conclusion: The stability of the pelvic ring of dual INFIX was sufficient to achieve bony fusion in this case. The stability of dual INFIX should be stronger than that of INFIX. Dual INFIX as with INFIX has other advantages such as ease of management compared with external fixation, and nonnecessity of strict anatomical reduction compared with various percutaneous screw fixation. Furthermore, this technique is simple and minimally invasive compared with plate fixation because it does not require open surgery. However, because the type C fracture with an unacceptable position of reduction by closed reduction has the possibility to become a symptomatic malunion, such cases should not be treated by this method. Furthermore, it is necessary for pelvic stabilization using dual INFIX that the contralateral pelvis is intact because dual INFIX stabilizes the fracture side with the other side of the pelvis. Dual INFIX can be considered as an option of fixation methods for type B-1 or 2 pelvic ring injuries.
Keywords: Internal anterior subcutaneous fixator, minimally invasive, spinal instrumentation, unstable pelvic ring injury.
External fixation [1], various subcutaneous screw fixations [2], and plate fixation [3, 4] can be considered as fixation methods for unstable pelvic ring fractures. Although external fixation is popular and minimally invasive, it has disadvantages such as complicated pin site management, pin site infection, and weak biomechanical stability [1, 4]. Although percutaneous screw fixation of the pelvic ring is also minimally invasive, it requires strict anatomical reduction of fractures and its biomechanical stability is weak [2]. Although plate fixation for pelvic ring fracture has achieved anatomic reduction of fractures under direct vison, it requires major open surgery [3]. Recently, application of an anterior subcutaneous fixator (INFIX) using spinal instrumentation has been reported [4, 5, 6]. INFIX comprises two screws inserted bilaterally into the anterior inferior iliac spine and a subcutaneous rod. INFIX was invented based upon the same biomechanical principles as traditional external fixation, but it is placed subcutaneously. INFIX has many advantages such as ease of management and nonnecessity of strict anatomical reduction and is minimally invasive. By contrast, the biomechanical stability of INFIX is weaker than that of plate fixation [4]. Therefore, INFIX is generally combined with a posterior fixation for fixation of pelvic ring injury [6]. In the case report herein, we describe a case of treated unstable pelvic ring injury using a dual internal anterior subcutaneous fixator we called “dual INFIX,” comprising four screws, two subcutaneous rods, and two cross-link connectors, without posterior fixation.
An 81-year-old man fell from a 4-m height and presented with severe left low back pain. Computed tomography (CT) showed an unstable pelvic injury (AO type B2) with fracture of the left ilium and pubis (Fig. 1). Because of active bleeding from a branch of the left lateral genital artery as detected on contrast-enhanced CT, transcatheter arterial embolization was performed on the day of the injury. Eight days later, dual INFIX was used to stabilize the pelvic ring injury. The patient was positioned supine on a radiolucent table. A longitudinal 5 cm incision was made centered over the anterior inferior iliac spine. Care was taken to protect the lateral femoral cutaneous nerve, which was retracted laterally. The entry point to the supra-acetabular corridor was identified from an obturator-outlet view on image intensification (Fig. 2a).

Polyaxial screws were introduced along a path between the anterior inferior iliac spine and ipsilateral posterior superior iliac spine until the head of the screw lay immediately above the fascia [5, 6] (Fig. 2b).
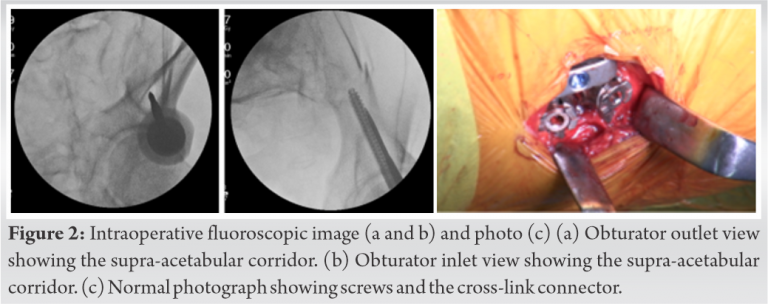
The size of the screws inserted was 80 mm long cranially, 100 mm long caudally, and both 8.0 mm in diameter. This process was repeated on the opposite side. Once both screws were inserted, 5.5 mm titanium rods were cut and shaped, considering the size and abdominal shape of the patient so as not to compress abdominal organs. Bilateral cranial screws were connected by a rod passed subcutaneously, and caudal screws were connected by the other rod. Finally, cross-link connectors connected cranial and caudal rods on the right and left (Fig. 2c and 3).

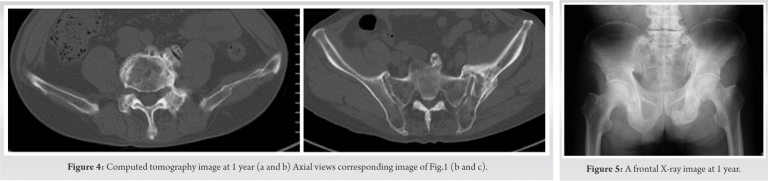
The surgical time was 100 min and intraoperative bleeding was 85 mL. Post-operatively, the patient was allowed to move freely and bear weight depending on pain without any limits. No iatrogenic neuropraxia of the lateral femoral cutaneous nerve occurred. Bony fusion was achieved as seen on CT at 4 month’ follow-up. Therefore, the implant was removed 4 months postoperatively in a 40-min operation. One year after the first operation, the patient could walk without a cane and had no limitation of daily living and there is no problem radiologically (Fig. 4a, b and 5).
Posterior fixation of unstable pelvic ring injuries using spinal instrumentation brings good reduction and strong stability [7, 8]. Recently, minimally invasive posterior fixations of unstable pelvic ring injuries using spinal instrumentation have been reported and show good clinical results [9, 10]. Because these techniques require screw insertion into the ilium, cases of pelvic ring injury with iliac fracture cannot be treated using these methods. Thus, indications of these techniques are unstable pelvic ring injuries with dislocation fracture of the sacrum or sacroiliac joint. Recently, INFIX has been reported and makes possible anterior pelvic ring fixation using spinal instrumentation [5, 6]. Although pelvic ring stability of INFIX is stronger than that of external fixation, that of INFIX is weaker than that of plate fixation [4]. Therefore, INFIX is generally combined with a posterior fixation for pelvic ring injury [6]. Although modified INFIX has been reported to make stability of the pelvic ring stronger than that of INFIX [11, 12], modified INFIX requires a subcutaneous rod to pass near the pubis because modified INFIX requires screw insertion into the pubis. Therefore, the flexibility of the subcutaneous rod path is low. Otherwise, the flexibility of dual INFIX as reported herein is the same as that of INFIX. Furthermore, stability of dual INFIX should be stronger than that of INFIX because dual INFIX comprises four screws, two subcutaneous rods, and two cross-link connectors, while INFIX comprises two screws, and one subcutaneous rod. In the case reported herein, we stabilized an unstable pelvic ring injury using dual INFIX without posterior fixation. The stability of the pelvic ring of dual INFIX was sufficient to achieve bony fusion in this case. Dual INFIX as with INFIX has other advantages such as ease of management compared with external fixation, and nonnecessity of strict anatomical reduction compared with various percutaneous screw fixation. Furthermore, this technique is simple and minimally invasive compared with plate fixation because it does not require open surgery. As a result, in this case, the surgical time was short and intraoperative bleeding was trivial. By contrast, because the reduction method of dual INFIX is closed reduction as is INFIX, strict reduction of fracture cannot be achieved compared with plate fixation, which requires open reduction. In a previous report, no difference in clinical outcome between INFIX and plate fixation was noted [3]. However, because the type C fracture with an unacceptable position of reduction by closed reduction has the possibility to become a symptomatic malunion [1, 13, 14, 15], such cases should not be treated by this method. Furthermore, it is necessary for pelvic stabilization using dual INFIX that the contralateral pelvis is intact because dual INFIX stabilizes the fracture side with the other side of the pelvis. Thus, type B-1 or 2 pelvic ring injuries are good indications for stabilization using dual INFIX. Another disadvantage of dual INFIX is that implant removal is required because subcutaneous implants of dual INFIX are bulkier than those of INFIX. Herein, to our knowledge, we report the initial case of an unstable pelvic fracture treated using dual INFIX. Therefore, more cases, clinical reports, and biomechanical studies comparing this method with INFIX and other fixators are needed.
We describe a case of treated unstable pelvic ring injury using a dual internal anterior subcutaneous fixator we called “dual INFIX,” comprising four screws, two subcutaneous rods, and two cross-link connectors, without posterior fixation. The stability of the pelvic ring of dual INFIX was sufficient to achieve bony fusion in this case. There is a possibility that “dual INFIX” is an option of treatment of type B-1 or 2 pelvic ring injuries.
We describe a case of treated unstable pelvic ring injury using a dual internal anterior subcutaneous fixator we called “dual INFIX,” comprising four screws, two subcutaneous rods, and two cross-link connectors, without posterior fixation. The stability of dual INFIX should be stronger than that of INFIX. Dual INFIX as with INFIX has other advantages such as ease of management compared with external fixation, and nonnecessity of strict anatomical reduction compared with various percutaneous screw fixation. Furthermore, this technique is simple and minimally invasive compared with plate fixation because it does not require open surgery. There is a possibility that “dual INFIX” is an option of treatment of type B-1 or 2 pelvic ring injuries.
References
- 1.Lindahl J, Hirvensalo E, Böstman O, Santavirta S. Failure of reduction with an external fixator in the management of injuries of the pelvic ring. Long-term evaluation of 110 patients. J Bone Joint Surg Br 1999;81:955-62. [Google Scholar]
- 2.Giannoudis PV, Tzioupis CC, Pape HC, Roberts CS. Percutaneous fixation of the pelvic ring: An update. J Bone Joint Surg Br 2007;89:145-54. [Google Scholar]
- 3.Yin Y, Luo J, Zhang R, Li S, Jiao Z, Zhang Y, Hou Z. Anterior subcutaneous internal fixator (INFIX) versus plate fixation for pelvic anterior ring fracture. Sci Rep 2019;9:2578. [Google Scholar]
- 4.Vigdorchik JM, Esquivel AO, Jin X, Yang KH, Onwudiwe NA, Vaidya R. Biomechanical stability of a supra-acetabular pedicle screw internal fixation device (INFIX) vs external fixation and plates for vertically unstable pelvic fractures. J Orthop Surg Res 2012;7:31. [Google Scholar]
- 5.Vaidya R, Colen R, Vigdorchik J, Tonnos F, Sethi A. Treatment of unstable pelvic ring injuries with an internal anterior fixator and posterior fixation: Initial clinical series. J Orthop Trauma 2012;26:1-8. [Google Scholar]
- 6.Dahill M, McArthur J, Roberts GL, Acharya MR, Ward AJ, Chesser TJ. The use of an anterior pelvic internal fixator to treat disruptions of the anterior pelvic ring: A report of technique, indications and complications. Bone Joint J 2017;99:1232-6. [Google Scholar]
- 7.Abumi K, Saita M, Iida T, Kaneda K. Reduction and fixation of sacroiliac joint dislocation by the combined use of S1 pedicle screws and the galveston technique. Spine (Phila Pa 1976) 2000;25:1977-83. [Google Scholar]
- 8.Bederman SS, Hassan JM, Shah KN, Kiester PD, Bhatia NN, Zamorano DP. Fixation techniques for complex traumatic transverse sacral fractures: A systematic review. Spine (Phila Pa 1976) 2013;38:E1028-40. [Google Scholar]
- 9.Koshimune K, Ito Y, Sugimoto Y, Kikuchi T, Morita T, Mizuno S, et al. Minimally invasive spinopelvic fixation for unstable bilateral sacral fractures. Clin Spine Surg 2016;29:124-7. [Google Scholar]
- 10.Okuda A, Maegawa N, Matsumori H, Kura T, Mizutani Y, Shigematsu H, et al. Minimally invasive spinopelvic “crab-shaped fixation” for unstable pelvic ring fractures: Technical note and 16 case series. J Orthop Surg Res 2019;14:51. [Google Scholar]
- 11.Wu X, Liu Z, Fu W, Zhao S, Feng J. Modified pedicle screw-rod fixation as a minimally invasive treatment for anterior pelvic ring injuries: An initial case series. J Orthop Surg Res 2017;12:84. [Google Scholar]
- 12.Becker CA, Kammerlander C, Kußmaul AC, Woiczinski M, Thorwächter C, Zeckey C, et al. Modified less invasive anterior subcutaneous fixator for unstable Tile-C-pelvic ring fractures: A biomechanical study. Biomed Eng Online 2019;18:38. [Google Scholar]
- 13.Lee KJ, Min BW, Oh GM, Lee SW. Surgical correction of pelvic malunion and nonunion. Clin Orthop Surg 2015;7:396-401. [Google Scholar]
- 14.Vanderschot P, Daenens K, Broos P. Surgical treatment of post-traumatic pelvic deformities. Injury 1998;29:19-22. [Google Scholar]
- 15.Matta JM, Dickson KF, Markovich GD. Surgical treatment of pelvic nonunions and malunions. Clin Orthop Relat Res 1996;329:199-206. [Google Scholar]



