
Multiple, chronic osteolytic lesions on imaging should be investigated for chronic multifocal osteomyelitis which may be related to a Mycobacterium avium complex associated inflammatory process which responds well to anti-inflammatory medications.
Dr. Jordan Johnson, Mountain View Regional Medical Center-Graduate Medical Education, 4351 E. Lohman Avenue, Suite 300. Las Cruces, New Mexico 88011. E-mail: jordanjohnsondo@gmail.com
Introduction:There are reports which describe multiple lytic lesions seen on X-ray resulting from a non-tuberculous Mycobacterium skeletal infection in immunocompetent adults and children. AdditionallyIn addition, similar multifocal lesions have also been described in chronic recurrent multifocal osteomyelitis (CRMO) which is more common in children but has have rarely been reported in adults. We present a case of a 47-year-old female who presented with multiple osteolytic lesions and discuss how her diagnosis overlaps with CRMO and multifocal non-tuberculous osteomyelitis associated with Mycobacterium avium complex (MAC).
Case Report:A 47-year-old female presented with a mass at her left sternoclavicular joint. Biopsy of the lesion showed acute and chronic inflammation suggesting osteomyelitis. The patient was on intravenousIV antibiotics with some improvement. After three 3 ½ and a half months, she was having knee pain and imaging showed another lesion and a bone scan found a third. Delayed cultures grew Mycobacterium avium complexMAC but ultimately the patient improved when she was taking naproxen for multifocal osteomyelitis.
Conclusion:Multifocal lytic lesions on imaging in an adult can be multifocal osteomyelitis that, like in pediatric patients, may be treated best with nonsteroidal anti-inflammatory medications as with the patient in this case.
Keywords:Multifocal Osteomyelitis, Mycobacterium Avium Complex, Osteitis Multifocal Osteomyelitis, Mycobacterium avium complex, osteitis.
There is a broad differential of diagnoses for a focal osteolytic bone lesion noted on imaging. The differential can be narrowed based on the lesion’s appearance, location, and progression. The differential also changes in the case of multifocal lesions within the bone. While there is a broad differential in these cases, being aware of uncommon pathology will help aid in developing a complete differential to then narrow to an accurate diagnosis. For example, there are reports which describe multiple lytic lesions seen on X-ray resulting from a non-tuberculous Mycobacterium skeletal infection in immunocompetent adults [1, 2, 3, –4] and children [5, 6, ,7, 8, 9, –10]. AdditionallyIn addition, similar multifocal lesions have also been described in chronic recurrent multifocal osteomyelitis (CRMO) which is more common in children [11] but has have rarely been reported in adults [12, 13, –14].
We present a case of a 47-year-old female who presented reporting she had been given the diagnosis of a sternoclavicular joint dislocation. However, upon review of her imaging, an osteolytic lesion in the medial clavicle was found. Later, similar skeletal lesions were found with radiographic evaluation of other body areas. We describe the development of a differential diagnosis for this case. We also discuss how the diagnosis overlaps with CRMO and multifocal non-tuberculous osteomyelitis associated with Mycobacterium avium complex (MAC). An awareness of these conditions through this case will help aid in the development of a diagnosis in future cases of multifocal lesions in adults.
A 47-year-old female presented to the orthopedic clinic for the evaluation of a bump over her left sternoclavicular joint that had been present for four 4 months. On initial presentation, there was no pain in the area, and she denied pain with range of motion. She reported an increase in the size of the lesion over the 4 months since first noticing it. She denied any trauma to the area. She had no history of fevers, weight loss, or smoking. She denied any family history of cancer or any personal history of masses in any other location. 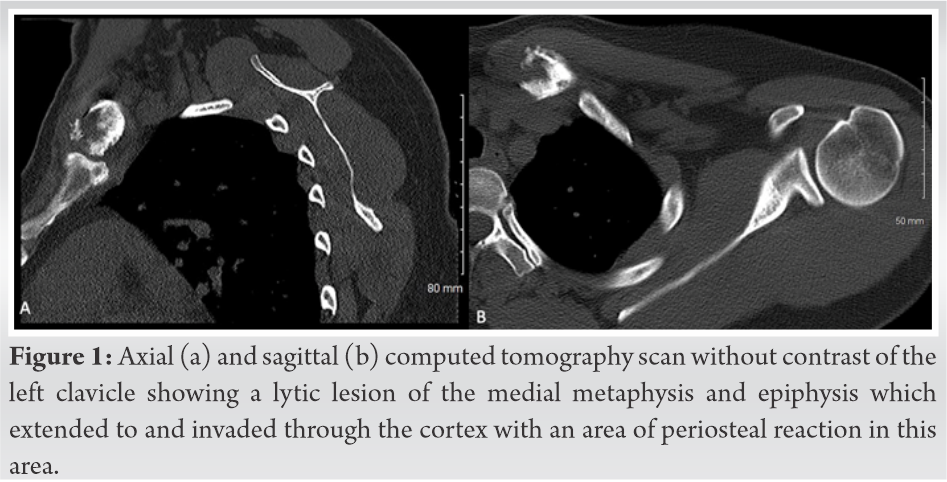
Radiographs demonstrated a lytic lesion of the medial aspect of the left clavicle that was difficult to delineate as it was overlying the mediastinum. She had a computed tomography (CT) scan of the left clavicle without contrast that demonstrated a lytic lesion of the medial metaphysis and epiphysis of the left clavicle which extended to and invaded through the cortex (Figure Fig. 1). There was a small area with periosteal reaction.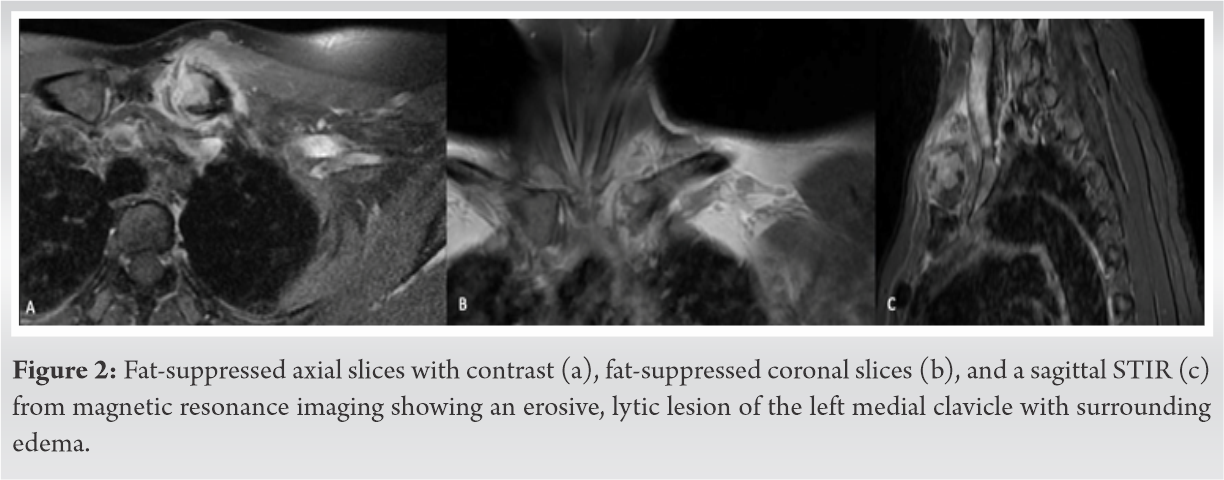
The aggressive nature of the lesion on CT scan was concerning for neoplasm and we recommended that the patient get an magnetic resonance imaging (MRI) with and without contrast to further evaluate the lesion. The MRI confirmed an erosive, lytic lesion of the left medial clavicle with surrounding edema (Figure Fig. 2). At this point, based on the imaging and our evaluation of the patient, the differential included osteomyelitis, eosinophilic granuloma, metastasis from another primary neoplasm, multiple myeloma, and lymphoma. 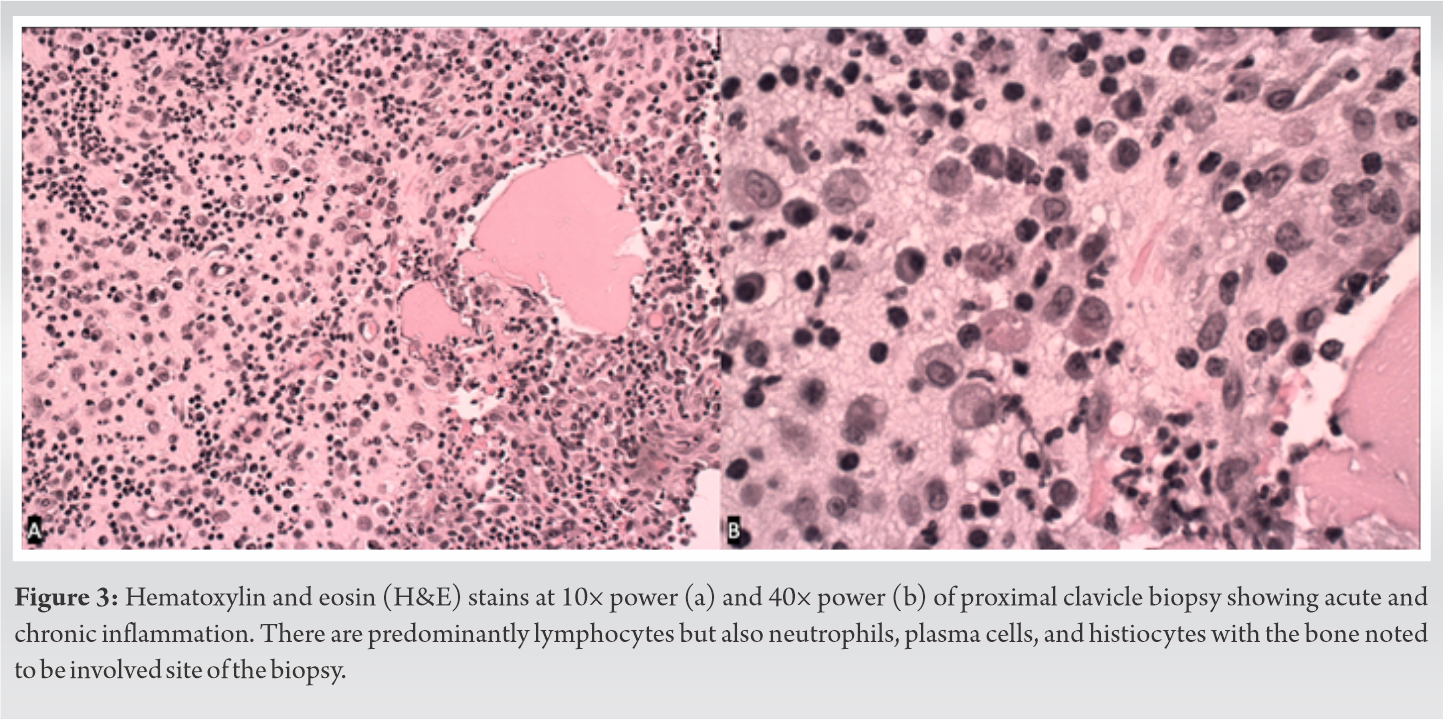
Basic laboratories were also obtained at this time. The C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were slightly elevated at 1.28 mg/L (normal 0.0-–0.5 mg/L) and 24 mm/hr (normal 0-–15 mm/hr). The white blood cell count (WBC) was within normal limits.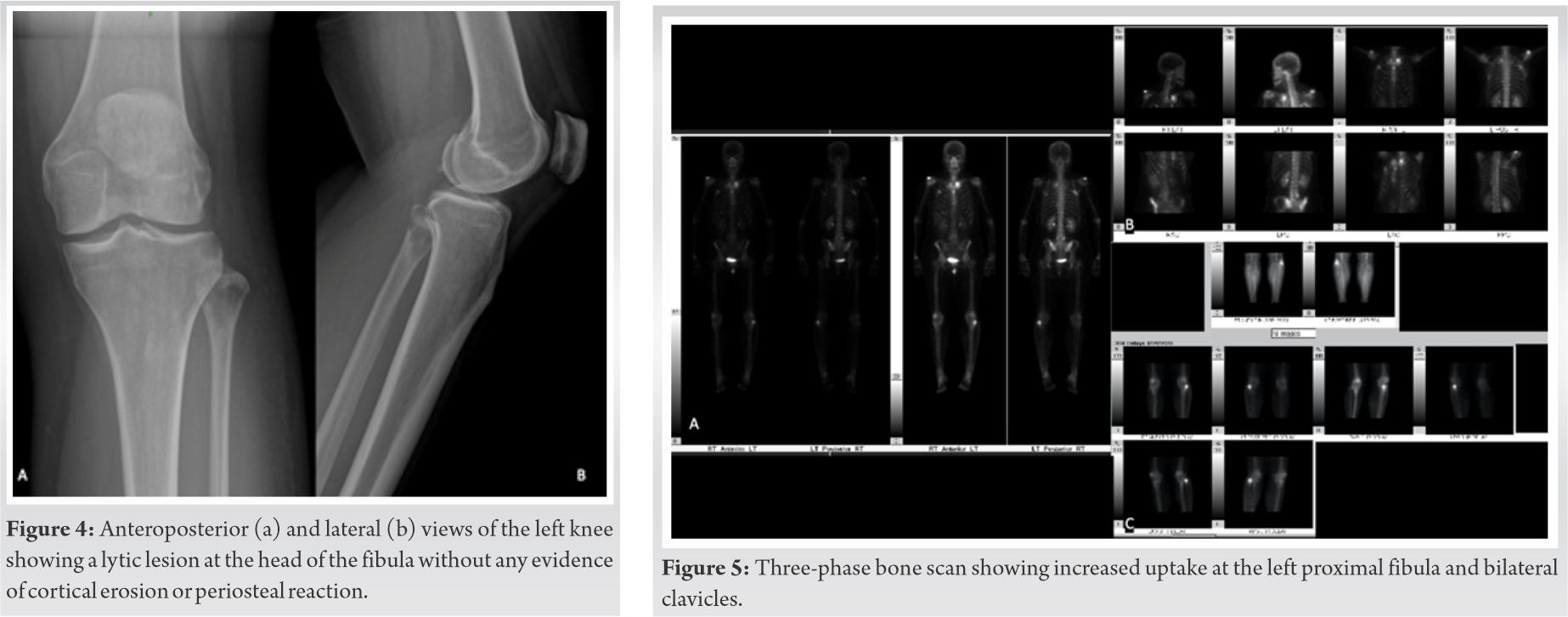
Given the uncertainty of the diagnosis with imaging and laboratories alone, it was recommended, and the patient agreed to proceed with a biopsy of the lesion. The biopsy was sent for culture and for evaluation by the pathologist.
The biopsy showed fibrous tissue with acute and chronic inflammation with skeletal muscle present. There were predominantly lymphocytes with scattered plasma cells and aggregates of neutrophils forming abscesses involving the bone. This was consistent with acute and chronic osteomyelitis (Figure Fig. 3). Given the presence of histiocytic cells, scattered eosinophils, and the density of lymphoid infiltrate, neoplastic and non-neoplastic processes also needed to be considered in the differential pending special studies. Final diagnosis from pathology showed acute and chronic inflammatory infiltrate with no significant lymphoid immunophenotypic abnormalities detected. There was no evidence of lymphoma, plasma cell neoplasm, or metastatic carcinoma. An irrigation and debridement with partial medial clavicle excision were then recommended and performed. The pathology from this procedure again showed acute and chronic inflammation with multi-nucleated cells. Cultures had no growth at five 5 days and intravenous (IV) daptomycin was continued.
Two and a half months after initial presentation, though the patient had some resolution of swelling with intravenous (IV) daptomycin, she developed a sinus tract at the site of the biopsy. An irrigation and debridement with partial medial clavicle excision were then recommended and performed. The pathology from this procedure again showed acute and chronic inflammation with multi-nucleated cells. Cultures had no growth at five 5 days and IV daptomycin was continued.
The patient presented for follow-up 3 ½ Three and a half months after her initial presentation and she indicated she was starting to have left knee pain near the proximal end of her left fibula . Radiographs of the left knee demonstrated an osteolytic lesion in the fibular head with a distinct, well-marginated border, and without sclerosis (Figure Fig. 4). This new lesion, with negative cultures up to this point, raised the suspicion for CRMO. The patient was sent for a bone scan. The antibiotics were discontinued, and she was started on naproxen 500 mg twice a day.
The bone scan demonstrated persistent uptake in the left medial clavicle and positive three-phase uptake at the left fibular head and the right clavicle suggestive of chronic osteomyelitis (Figure Fig. 5). Naproxen was continued for the patient, and she was referred to rheumatology for further treatment with the diagnosis of CRMO.
The initial tests from the mycobacterium culture were negative at the time of biopsy. The polymerase chain reaction (PCR) test for Mycobacterium species eventually was positive for MAC. Despite this development, the patient’s symptoms had resolved while on naproxen at six 6 months follow-up. Given her improvement and normal laboratories, the decision was made not to restart antibiotics and the patient was instructed to continue follow-up with rheumatology with orthopedic follow-up as needed.
Non-tuberculous Mycobacterium have been reported to cause lung, skin, lymph, and skeletal infections [4]. Many have reported these organisms, including MAC, resulting in chronic and recurrent osteomyelitis in immunocompetent adults [1, 2, 3, –4] and children [5, 6, 7, 8, 9, –10]. Most often in these cases, the patients present with symptoms similar to malignancy such as fever, weight loss, and pain with an associated lytic lesion seen on X-rays [3]. Similar lesions can be seen radiographically in CRMO which is commonly thought of as an autoimmune disease of childhood [11], but it has been reported in adults [12, 13, –14]. Onset of CRMO in adulthood is rarely reported and is often associated with synovitis, acne, pustulosis, hyperostosis, and osteitis (SAPHO) syndrome [14]. CRMO is treated with anti-inflammatory and immunomodulating medications [11, 14], while cases of confirmed MAC- associated osteomyelitis are usually treated with antimycobacterial antibioticsantibiotics, and many undergo surgical debridement.
This case bears many similarities between both these pathologies. Our patient had multiple osteolytic lesions in the locations most commonly associated with CRMO, those being the medial clavicle and proximal fibula [8, 11]. In almost all cases of MAC- associated osteomyelitis, the patients had associated fever and weight- loss, and one defining feature that is present with almost all cases of MAC- associated osteomyelitis is the sinus that formed at the site of the biopsy [1, 2, 4, 5, 8]. Our patient had a sinus tract form after biopsy similar to other cases of recurrent multifocal osteomyelitis related to positive MAC but no systemic symptoms.
The PCR testing for mycobacterium species was not shown to be positive until late into the treatment course. Because of this, the patient was on daptomycin for several weeks but not traditional antimycobacterial agents. The antibiotics had been discontinued when more lesions were found and the patient was started on naproxen, one of the traditional first-line drugs in the treatment of CRMO [14]. She has had resolution of her symptoms with this treatment, and as such antibiotics were not restarted.
Though Although the cause of these lesions may be related to MAC, she showed the most symptomatic progress with the use of anti-inflammatory medications, which is one of the most common successful treatments used for CRMO [14]. This suggests that the lesions are likely an inflammatory response rather than an infectious lesion. The knowledge of the possibility of this inflammatory process will aid in the formation of the differential and final diagnosis in adult patients with multiple osteolytic lesions. AdditionallyIn addition, it may be beneficial to aim further research at determining if there is a connection between MAC positivity and the development of multifocal osteitis that responds to anti-inflammatory medication as does traditional non-infections CRMO.
The differential of diagnoses is broad when evaluating patients with multiple osteolytic bone lesions. This case demonstrates that there is an association between non-tuberculous Mycobacterium and CRMO in adults which can be considered in these cases of multiple osteolytic lesions. The patient in this case had features of both MAC osteomyelitis and CRMO and improved with anti-inflammatory medications. This suggests that in cases of chronic multifocal lesions in adults, a trial of anti-inflammatory medications, which in a short course is generally benign enough, could be a good place to start in treating patients with this presentation.
Multiple, chronic osteolytic lesions on imaging should be investigated for a variety of differential diagnoses including, among others, . Within these differentials lies CRMO and infections osteomyelitis . In the case of CRMO, it may be related to a MAC- associated mycobacterial inflammatory process which responds well to anti-inflammatory medications as shown by this case report.
References
- 1.1. Kerens B, Gans EH, Pilot P, van der Tempel H, Verburg AD. Atypical tuberculous osteomyelitis of the humeral shaft caused by Mycobacterium avium. Ned Tijdschr Geneeskd 2006;150:1728-31. [Google Scholar]
- 2.2. Marchevsky AM, Damsker B, Green S, Tepper S. The clinicopathological spectrum of non-tuberculous mycobacterial osteoarticular infections. J Bone Joint Surg Am 1985;67:925-9. [Google Scholar]
- 3.3. Pombo D, Woods ML, Burgert SJ, Shumsky IB, Reimer LG. Disseminated Mycobacterium avium complex infection presenting as osteomyelitis in a normal host. Scand J Infect Dis 1998;30:622-3. [Google Scholar]
- 4.4. Yano K, Kazuki K, Ikeda M, Yoneda M. Osteomyelitis and arthritis of the wrist caused by Mycobacterium intracellulare in an immunocompetent patient: A case report and literature review. Acta Reumatol Port 2014;39:176-81. [Google Scholar]
- 5.5. Lincoln EM, Gilbert LA. Disease in children due to mycobacteria other than Mycobacterium tuberculosis. Am Rev Respir Dis 1972;105:683-714. [Google Scholar]
- 6.6. Stone AB, Schelonka RL, Drehner DM, McMohon DP, Ascher DP. Disseminated Mycobacterium avium complex in non-human immunodeficiency virus-infected pediatric patients. Pediatr Infect Dis J 1992;11:960-4. [Google Scholar]
- 7.7. Bender BL, Yunis EJ. Disseminated nongranulomatous Mycobacterium avium osteomyelitis. Hum Pathol 1980;11:476-8. [Google Scholar]
- 8.8. Kourtis AP, Ibegbu CC, Snitzer JA, Nesheim SR. Recurrent multifocal osteomyelitis due to Mycobacterium avium complex. Clin Infect Dis 1996;23:1194-5. [Google Scholar]
- 9.9. Frosch M, Roth J, Ullrich K, Harms E. Successful treatment of Mycobacterium avium osteomyelitis and arthritis in a non-immunocompromised child. Scand J Infect Dis 2000;32:328-9. [Google Scholar]
- 10.10. Collert S, Petrini B, Wlckman K. Osteomyelitis caused by Mycobacterium avium. Acta Orthop 1983;54:449-51. [Google Scholar]
- 11.11. Duffy CM, Lam PY, Ditchfield M, Allen R, Graham HK. Chronic recurrent multifocal osteomyelitis: Review of orthopaedic complications at maturity. J Pediatr Orthop 2002;22:501-5. [Google Scholar]
- 12.12. Hong CW, Hsiao EC, Horvai AE, Link TM. Chronic recurrent multifocal osteomyelitis with an atypical presentation in an adult man. Skeletal Radiol 2015;44:1359-64. [Google Scholar]
- 13.13. Mahady S, Ladani A. Clinical and diagnostic considerations for atypical, adult onset presentation of chronic recurrent multifocal osteomyelitis (CRMO). Case Rep Rheumatol 2019;2019:8206892. [Google Scholar]
- 14.14. Rech J, Manger B, Lang B, Schett G, Wilhelm M, Birkmann J. Adult-onset Still’s disease and chronic recurrent multifocal osteomyelitis: A hitherto undescribed manifestation of autoinflammation. Rheumatol Int 2012;32:1827-9. [Google Scholar]






