
Inverted V-shaped High Tibial Osteotomy would be selected as one of the effective treatments for severe genu varum caused by Blount disease.
Dr. Seiju Hayashi,
Department of Orthopaedic Surgery, Mazda Hospital, Fuchu, Hiroshima, Japan.
E-mail: payakichi0213@hotmail.com
Abstract
Introduction: Blount disease is a growth disorder of the medial proximal tibial physis causing a multi-planar deformity of the lower limb. Several types of surgical approaches have been described for the correction of angular deformity including external fixation, opened-/closed- wedge high tibial osteotomy (HTO), and tibial condylar valgus osteotomy. However, they are associated with various disadvantages such as limb length discrepancy, risk of infections, and delayed union at the osteotomy site, especially in cases of severe varus deformity.
Case Report: We report a case of a 16-year-old boy with unilateral severe genu varum caused by Blount disease. Considering that the current case, the patient was severely obese and a highly active young boy with severe unilateral genu varum, with the epiphyseal line almost closed, and with no abnormalities with respect to the intra-articular anatomical structures, inverted V-shaped HTO was applied. After the treatment, the boy was not only able to perform his daily activities but was also able to participate in sports quite early. Although the required correction angle was quite large, inverted V-shaped HTO successfully corrects the deformity with minimal disadvantages
Conclusion: Inverted V-shaped HTO would be selected as one of the effective treatments for a severely obese, young, and highly active patient suffering from severe genu varum caused by Blount disease.
Keywords: Blount disease, genu varum, obesity, high tibial osteotomy (HTO), inverted V-shaped high tibial osteotomy (iVHTO).
Blount disease is a growth disorder of the medial proximal tibial physis and epiphysis, which results in a multi-planar deformity of the lower limb. The disease was first described in detail by Blount in 1937 [1]. Several types of surgical approaches have been described for the correction of angular deformity of the knee including external fixation [2], open-wedge high tibial osteotomy HTO (OWHTO) [3], closed-wedge HTO (CWHTO) [4], and tibial condylar valgus osteotomy (TCVO) [5]. However, they are associated with various disadvantages such as limb length discrepancy, risk of infections, and delayed union or non–union at the osteotomy site, especially in cases of severe varus deformity. In contrast, Levy et al. [6] proposed that inverted V-shaped high tibial osteotomy (iVHTO) is advantageous, especially in severe varus deformity, as it provides sufficient correction angle with large bone stock and wide bony contact with less such disadvantages.
In this study, iVHTO was applied to correct severe tibial genu varum in a severely obese and highly active young boy who was suffering from Blount disease.
A 16-year-old boy noticed asymptomatic right knee deformity two 2 years before visiting the hospital. Although he had played baseball, the gradually deteriorating knee pain prevented him from playing. The height of the boy was 173 cm, the weight was 126 kg, and the body mass index was 33 kg/m2. Severe lateral thrust in walking was noticed (Supplemental File 1).
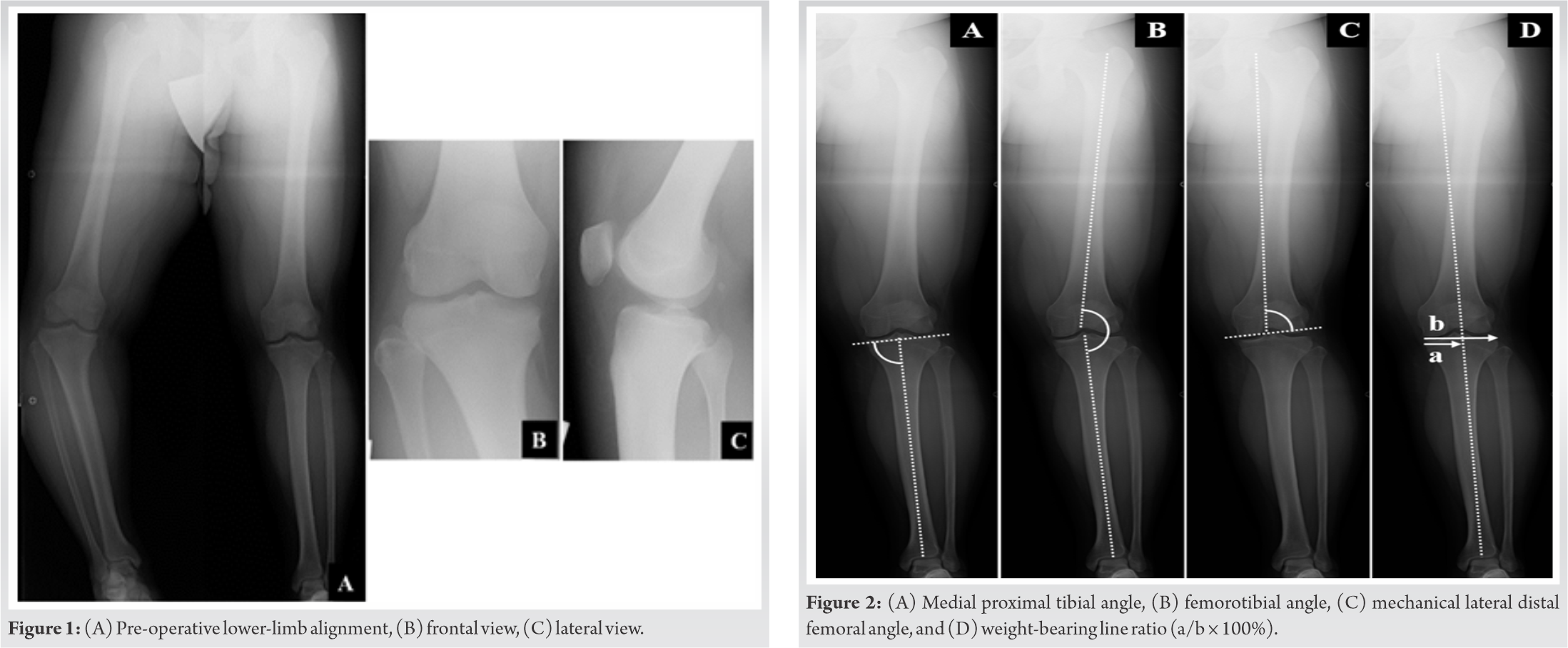 The range of motion (ROM) was 0° in extension and 135° in flexion. The subscales of pre-operative knee injury and osteoarthritis outcome score (KOOS) [7] (symptoms; pain; daily activities; sports and recreational function; and quality of life) were 89.29, 80.56, 82.35, 45, and 75, respectively. Bilateral anteroposterior long-leg weight-bearing radiograph (Fig. 1A-C) showed that the medial proximal tibial angle (MPTA), femorotibial angle (FTA), and the mechanical lateral distal femoral angle (mLDFA) in the right/left legs were 70°/89°, 204°/171°, and 94°/93°, respectively (Fig. 2A-C).The weight-bearing line ratio (WBLR) and non-weight bearing line ratio WBLR (non-WBLR) in the right/left legs were found to be −62%/54%, and −19%/42%, respectively. WBLR is defined as the horizontal distance from the medial edge of the tibial plateau to the WBL divided by the width of the tibial plateau (Fig. 2D). Detailed deformities were examined by using three-dimensional (3D) computed tomography (CT) images (Fig. 3A and B). Magnetic resonance imaging showed no abnormalities in the intra-articular anatomical structures, and the epiphyseal line was almost closed (Fig. 4A-C).
The range of motion (ROM) was 0° in extension and 135° in flexion. The subscales of pre-operative knee injury and osteoarthritis outcome score (KOOS) [7] (symptoms; pain; daily activities; sports and recreational function; and quality of life) were 89.29, 80.56, 82.35, 45, and 75, respectively. Bilateral anteroposterior long-leg weight-bearing radiograph (Fig. 1A-C) showed that the medial proximal tibial angle (MPTA), femorotibial angle (FTA), and the mechanical lateral distal femoral angle (mLDFA) in the right/left legs were 70°/89°, 204°/171°, and 94°/93°, respectively (Fig. 2A-C).The weight-bearing line ratio (WBLR) and non-weight bearing line ratio WBLR (non-WBLR) in the right/left legs were found to be −62%/54%, and −19%/42%, respectively. WBLR is defined as the horizontal distance from the medial edge of the tibial plateau to the WBL divided by the width of the tibial plateau (Fig. 2D). Detailed deformities were examined by using three-dimensional (3D) computed tomography (CT) images (Fig. 3A and B). Magnetic resonance imaging showed no abnormalities in the intra-articular anatomical structures, and the epiphyseal line was almost closed (Fig. 4A-C).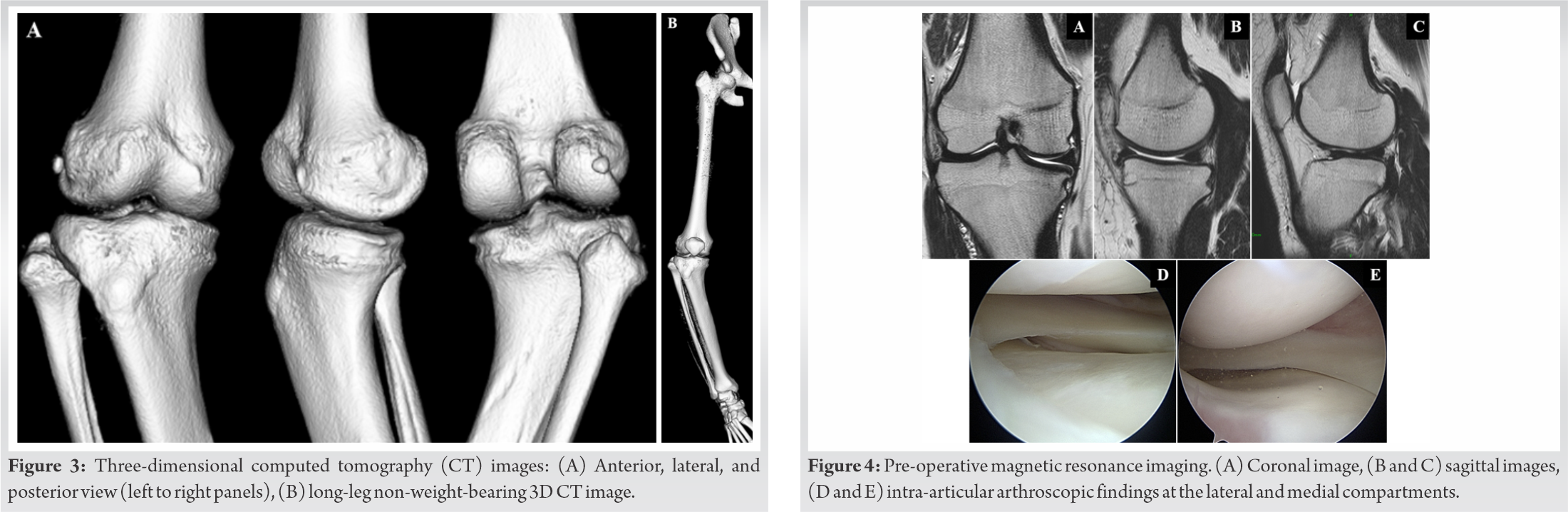
Considering that the current case, the patient was severely obese and a highly active young boy with severe genu varum, with the epiphyseal line closed, and with no abnormalities in the intra-articular anatomical structures, iVHTO was selected.
The surgery was performed as described in the previous studies [8,9,10]. At first, an arthroscopy was performed and no abnormal intra-articular abnormalities were detected (Fig. 4D, and E). The correction angle was set at 19° so that the post-operative non-WBLR would pass where the contralateral side passes. Lateral hemi-closed-wedge and medial hemi-opened-wedge osteotomy were performed, and then, the biplanar V-shaped osteotomy was completed (Fig. 5A-C). Next, the corrected tibia was fixed using a locking compression plate (Tris- Hybrid Lateral 2 HTO Plate system; Olympus Terumo Biomaterials Corp., Tokyo, Japan) (Fig. 5D). Then, the bone stock resected from the lateral tibia was implanted in the medial opening space (Fig. 5E).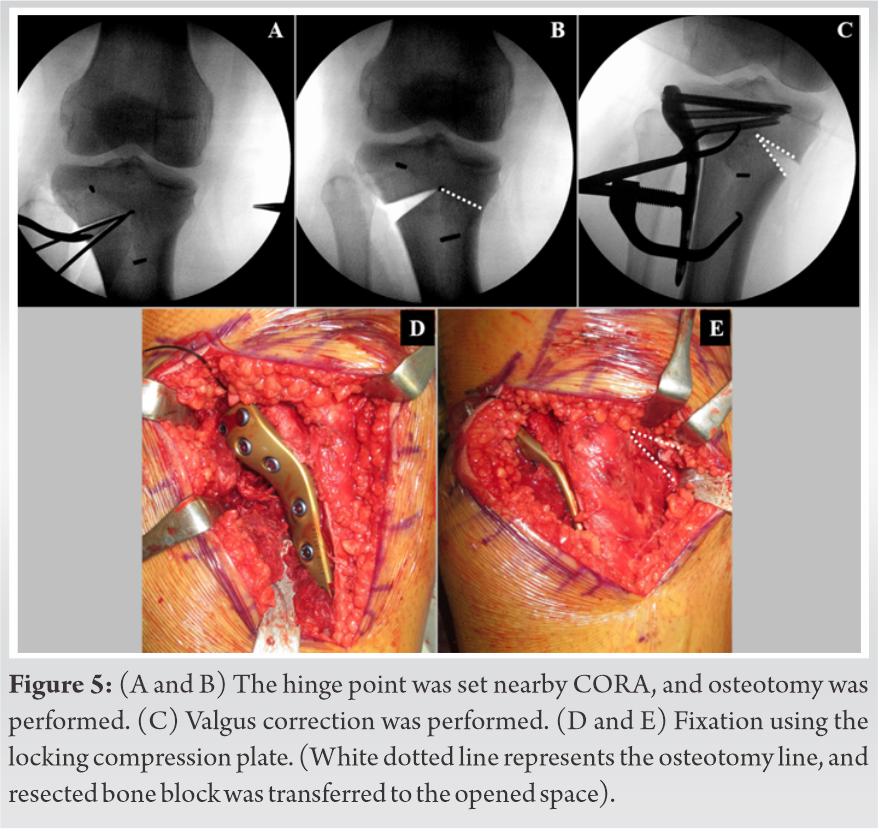
Continuous passive ROM was started one 1 day after the surgery, and the patient was allowed to bear only one-sixth of the body weight (BW) at 1-week post-surgery, each one-sixth of the BW was additionally loaded week by week. The patient was permitted to resume his sports activities gradually 3 months postoperatively. The patient finally resumed his daily activities and could perform quite well at sports as well at 1-year post-surgery (Supplemental File 2). Post-operative MPTA was 95°, FTA was 177°, and WBLR was 35% (Fig. 6A-C). Post-operative 3D-CT imaging revealed that the bones had united completely (Fig. 6D). The subscales of post-operative KOOS also improved to 96.43, 97.22, 100, 100, and 100, respectively.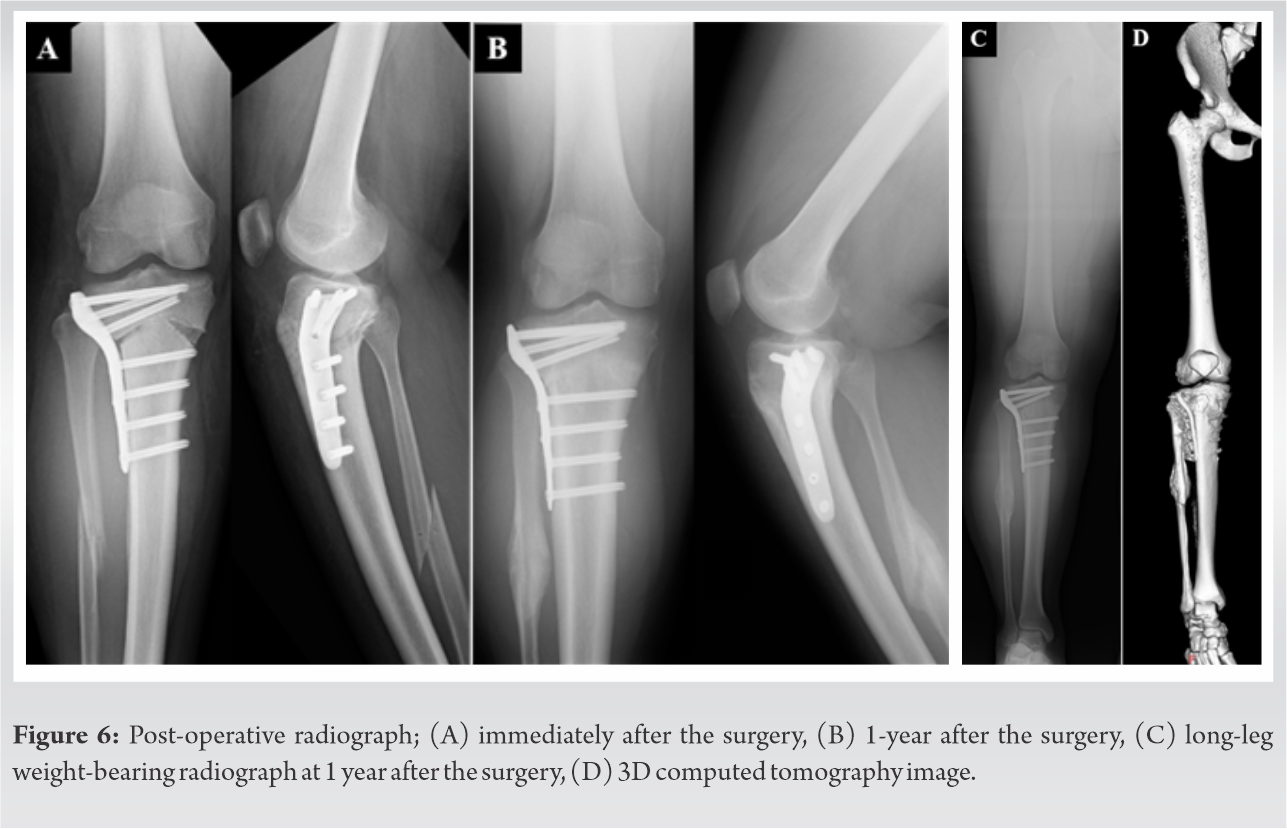
Successful post-operative outcomes were obtained by ivHTO in a severely obese, young, and highly active patient suffering from severe genu varum caused by Blount disease.
The Ilizarov circular fixator is widely used for the correction of Blount disease. The advantages of this method include early motion, and correction of the multi-planar deformity; however, the length of the treatment time and the use of an external fixator may prove to be extremely cumbersome, and the patients are likely to suffer from complications such as skin problem and pin site infection [2].
At present, tibial osteotomy using locking plate system, several types of HTO [3,4,5] are the more preferred options with proven success in producing angular fixation to enable early ROM and weight-bearing with a lower risk of infection. The OWHTO technique suffers from limitations as well, especially in the following cases: When a large correction angle is required; when sufficient valgus correction is required; in case of a compartment syndrome; delayed- union or non-union in the gap; increase in the posterior tibial slope (PTS) angle; and decrease of the patellar height [3,11,12]. The disadvantages of conventional CWHTO are lateral-offset, decrease of the posterior tibial slopePTS angle. Leg length discrepancy is likely to occur in both cases [11,12]. Although, TCVO is a type of opening wedge HTO, it has some disadvantages too. The valgus correction can be done at a limited angle only for correcting the tibia to valgus until the lateral joint is reduced [5]. In addition, it cannot be applied on young patients with intact intra-articular anatomical structures because TCVO requires bone cut into the intra-articular surface.
Inverted V-shaped iVHTO is classified as a hemi-CW and hemi-OW osteotomy, and has advantages, such as it requires a smaller amount of bone resection and smaller opening gap and there is no limitation regarding the correction angle [8,9]. Besides, there is no vacant space in the tibia due to grafting of the resected bone block after surgery, and the bone stock in the tibia does not change after surgery. Therefore, it only accounts for 6% delayed union in iVHTO as compared with that of 23% in CWHTO [13]. Besides, there is less likelihood of occurrence of leg length discrepancy in iVHTO [8]. For better or worse, iVHTO does not change the posterior tibial slope (PTS) angle. In the current case, pre-operative PTS in medial tibial plateau was 20°, which did not change postoperatively. Therefore, there is limitation in multi-planar angular correction like external fixator in two- dimensional HTO, even in iVHTO.
Successful post-operative outcome was obtained by iVHTO in a severely obese and highly active young patient with severe genu varum caused by Blount disease. Although the required correction angle was quite large, employing iVHTO could be successfully corrected, with minimal limitations.
Inverted V-shaped HTO would be selected as one of the effective treatments for a severely obese, young, and highly active patient suffering from severe genu varum caused by Blount disease.
Inverted V-shaped HTO would be selected as one of the effective treatments for severe genu varum caused by Blount disease.
References
- 1.Blount WP. Tibia vara. J Bone Joint Surg 1937;19:1-29. [Google Scholar | PubMed]
- 2.Janoyer M. Blount disease. Orthop Traumatol Surg Res 2019;105:S111-21. [Google Scholar | PubMed]
- 3.Griswold B, Gilbert S, Khoury J. Opening wedge osteotomy for the correction of adolescent tibia vara. Iowa Orthop J 2018; 38:141-6. [Google Scholar | PubMed]
- 4.Coventry MB. Osteotomy of the upper portion of the tibia for degenerative arthritisof the knee. A preliminary report. J Bone Joint Surg Am 1965;47:984-90. [Google Scholar | PubMed]
- 5.Kuwashima U, Yonekura A, Itoh M, Itou J, Okazaki K. Tibial condylar valgus osteotomy-indications and technique. J Exp Orthop 2020;7:30. [Google Scholar | PubMed]
- 6.Levy M, Pauker M, Lotem M, Seelenfreund M, Fried A. High tibial osteotomy: A follow-up study and description of a modified technic. Clin Orthop Relat Res 1973;93:274-7. [Google Scholar | PubMed]
- 7.Goldhahn S, Takeuchi R, Nakamura N, Nakamura R, Sawaguchi T. Responsiveness of the knee injury and osteoarthritis outcome score (KOOS) and the Oxford knee score (OKS) in Japanese patients with high tibial osteotomy. J Orthop Sci 2017;22:862-7. [Google Scholar | PubMed]
- 8.Kondo E, Yasuda K, Yabuuchi K, Aoki Y, Inoue M, Iwasaki N, et al. Inverted V-shaped high tibial osteotomy for medial osteoarthritic knees with severe varus deformity. Arthrosc Tech 2018;7:e999-1012. [Google Scholar | PubMed]
- 9.Abe D, Hamai S, Okazaki K, Yoshimoto M, Komatsu T, Nakashima Y. Inverted V-shaped high tibial osteotomy for severe tibia vara associated with Turner syndrome: A case report and review of literature. Int J Surg Case Rep 2018;42:128-32. [Google Scholar | PubMed]
- 10.Yasuda K, Kondo E, Ueda D, Onodera J, Yabuuchi K, Tanabe Y, et al. An acute oblique osteotomy and suture ligation procedure to shorten the fibula in lateral closing-wedge high tibial osteotomy. Arthrosc Tech 2020;9:e1299-308. [Google Scholar | PubMed]
- 11.Cheng X, Liu F, Xiong F, Huang Y, Paulus AC. Radiographic changes and clinical outcomes after open and closed wedge high tibial osteotomy: A systematic review and meta-analysis. J Orthop Surg Res 2019;14:179. [Google Scholar | PubMed]
- 12.Sun H, Zhou L, Li F, Duan J. Comparison between closing-wedge and opening-wedge high tibial osteotomy in patients with medial knee osteoarthritis: A systematic review and meta-analysis. J Knee Surg 2017;30:158-65. [Google Scholar | PubMed]
- 13.Aoki Y, Yasuda K, Mikami S, Ohmoto H, Majima T, Minami A. Inverted V-shaped high tibial osteotomy compared with closing-wedge high tibial osteotomy for osteoarthritis of the knee. Ten-year follow-up result. J Bone Joint Surg Br 2006;88:1336-40. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 April 10, 2023 A Rare Presentation of Transient Osteoporosis of the Talus: Case Report
April 10, 2023 A Rare Presentation of Transient Osteoporosis of the Talus: Case Report January 10, 2020 A Case Report of Acute Exertional Compartment Syndrome with Peroneal Nerve Palsy in an Adolescent Athlete
January 10, 2020 A Case Report of Acute Exertional Compartment Syndrome with Peroneal Nerve Palsy in an Adolescent Athlete September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report
September 1, 2025 Massive Tendo Achilles Xanthoma Treated with en bloc Excision and Reconstruction with Flexor Hallucis Longus Tendon Transfer: A Case Report July 1, 2026 Correlation between Magnetic Resonance Imaging Modic Endplate Changes and Histopathological Inflammatory Activity in Lumbar Degenerative Disc Disease
July 1, 2026 Correlation between Magnetic Resonance Imaging Modic Endplate Changes and Histopathological Inflammatory Activity in Lumbar Degenerative Disc Disease