
Any patient of any age with proportionate dwarfism being investigated for endocrine abnormalities should also have a screening radiograph of the pelvis to rule out SCFE.
Dr. Amit Kumar Yadav, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: amit_aur09@yahoo.com
Introduction: Slipped capital femoral epiphysis (SCFE) is rare in adults and is often associated with endocrine pathology.
Case Report:We report a case of a 21-year-old male presenting with an acute on chronic left hip SCFE who was diagnosed with primary hypothyroidism on the investigation. The patient was treated for hypothyroidism and positional reduction with in-situ fixation was carried out with two cannulated cancellous screws for the SCFE. At the latest follow-up of 30 months, patient remains asymptomatic, euthyroid, with a nearly full range of motion in the hips, significant functional improvement, fused physis on radiographs, and no signs of avascular necrosis.
Conclusion: SCFE is a potentially devastating but avoidable complication in children/adults with the endocrine disorder and there may be a possible role for a screening pelvic radiograph in detecting this condition earlier.
Keywords: Hypothyroidism, slipped capital femoral epiphysis, adult slipped capital femoral epiphysis.
Slipped capital femoral epiphysis (SCFE) is a misnomer; it is the femoral neck and shaft that displaces relative to the femoral epiphysis and the acetabulum. The incidence of SCFE is approximately 2/1000,000 and typically occurs in adolescence, an average of about 13 years in boys and 11 years in girls [1]. About 20–40% of patients have bilateral involvement at presentation [2]. Patients <10 years or more than 16 years of age are the atypical presentation of SCFE. SCFE in adults occurs due to delayed maturation of the skeleton. The etiology of SCFE is multifactorial including idiopathic, trauma, genetic, endocrine, radiation, renal failure, and drugs. The most common endocrine abnormality is hypothyroidism and growth hormone deficiency.
A 21–year-old man presented to the outpatient department with complaints of dull aching intermittent pain over the left hip and difficulty in walking for 1 year. Two weeks before the presentation, the patient had a trivial fall and was unable to mobilize without support. The patient had a history of delayed developmental milestones and had to drop out of school because of bullying for short stature. The patient also complained of general fatigue and inability to do any kind of manual work resulting in lack of employment. On general examination, the patient had short stature (Height -158 cm), normal weight (53 kg, body mass index [BMI]-21.2 kg/m2) with coarse facial features. On local examination, there was tenderness anteriorly over the left hip with wasting of the thigh muscles associated with restriction of abduction, flexion, and internal rotation. External rotation of the hip was increased especially in flexion. The patient had a severely antalgic gait with external rotation of the left hip.
An anteroposterior and lateral plain radiograph of pelvis with both hips showed a left hip SCFE with still open proximal femoral physis (Fig. 1a, b). In addition, the pelvis x-ray showed a bone age of Risser stage 0 and open triradiate cartilage. In view of the clinical and radiological signs, a detailed endocrine workup was carried out by the pediatric endocrine team. Blood examination showed normal triiodothyronine [T3] (1.37 ng/ml; normal: 0.5–1.6), low thyroxin [T4] (3.7 ng/ml; normal: 4.9–11.6), and elevated thyroid-stimulating hormone [TSH] (45.79 ng/ml; normal: 0.4–6.16). The rest of the laboratory parameters including renal function tests, growth hormone, testosterone, and cortisol were within normal limits. The patient was diagnosed with Primary hypothyroidism. He was commenced on levothyroxine tablet 100 mcg once a day for 5 days in a week and a half tablet for 2 days a week. After 1.5 months of treatment, normal T4 and TSH levels were achieved.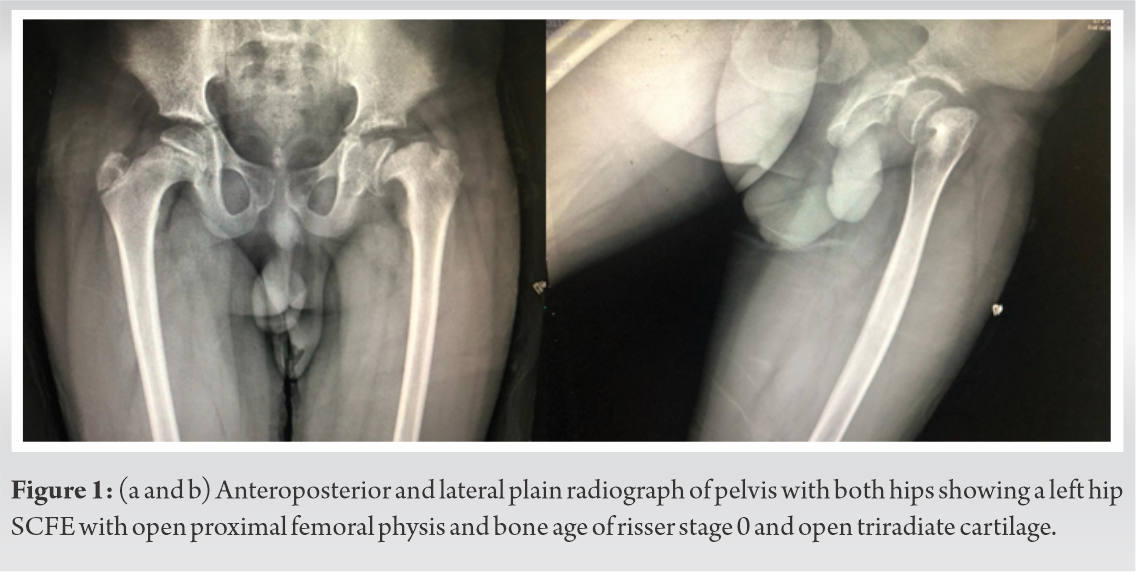
The patient was planned for surgery urgently due to the SCFE being unstable. The positional reduction was achieved by gentle positioning of the patient on the traction table. Although reduction was not complete, no attempts at closed reduction were made and in-situ fixation was carried out with two 6.5 mm partially threaded Cancellous Cannulated screws, ensuring the screws remained perpendicular to the physis (Fig. 2a, b). At the last follow-up of 30 months, the patient remains asymptomatic, with a nearly full range of motion in the hips, significant functional improvement, fused physis on radiographs, no signs of avascular necrosis, and normal thyroid function (Fig. 3a, b). Although there is coxa magna, coxa breva, and possible cam impingement on the radiograph, this is simply being observed as the patient remains asymptomatic.
At the last follow-up of 30 months, the patient remains asymptomatic, with a nearly full range of motion in the hips, significant functional improvement, fused physis on radiographs, no signs of avascular necrosis, and normal thyroid function (Fig. 3a, b). Although there is coxa magna, coxa breva, and possible cam impingement on the radiograph, this is simply being observed as the patient remains asymptomatic.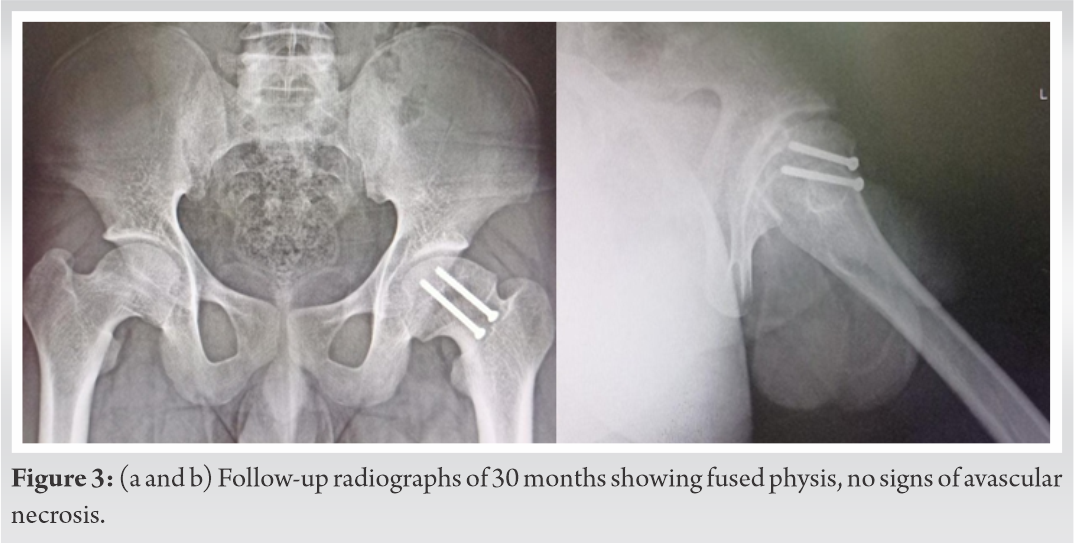
SCFE is usually associated with obesity, especially in hypothyroidism but our patient had a normal BMI for his height. Thyroid hormone activates the synthesis of bone matrix by increasing the secretion of growth hormone and insulin-like growth factor (IGF). Hypothyroidism leads to delay in ossification and inactivation of growth hormone and IGF resulting in short stature. Hypothyroidism also leads to decreased gene expression of proteoglycans and type X collagen on physis resulting in weakening of the epiphysis and delayed closure [3]. Short stature indicates that hypothyroidism was present for several years before the current episode of SCFE.
SCFE usually does not occur after 15–17 years of age because the proximal physis of the femur is closed by this age in boys. Endocrine disorder (hypothyroidism) leading to delayed closure of physis can cause SCFE in adults. It is, therefore, advisable to always investigate for endocrine pathology in adult SCFE. Kadowaki et al. reviewed 42 patients of SCFE with hypothyroidism and found the mean age of onset of SCFE 13.5 years (7–28), five patients had the disease after 18 years, two patients had onset before 9 years of age and short stature was present in 80% [4].
Macía-Villa et al. reviewed 60 cases of SCFE in adults and observed the most common cause to be idiopathic followed by endocrine (hypophyseal >hypothyroidism) [5]. Song reviewed 30 hips of adult SCFE, six cases of their own, 24 from previously published studies with an average age of 25 years (18–34), and observed the most common underlying pathology to be panhypopituitarism followed by hypothyroidism [2].
The importance of this case lies in the fact that this was primarily a medical disorder of primary hypothyroidism that remained undiagnosed and untreated for several years despite repeated visits by the patient to several doctors. The slipped femoral capital epiphysis was a fully preventable final hit that ultimately led to the diagnosis of this patients ailment and appropriate treatment. It was this belief that led us not to fix the contralateral hip prophylactically as treating his hypothyroidism resulted in physeal closure within 6 months on both sides [6]. Huang et al. managed a 29-year-old male with congenital hypopituitarism with open reduction and Dunn procedure without prophylactic fixation of the contralateral hip [7].
While it is the norm to rule out endocrine abnormalities in SCFE, we believe the converse is also true. Any patient of any age with proportionate dwarfism being investigated for endocrine abnormalities should also have a screening radiograph of the pelvis to rule out SCFE.
There may be a possible role for a screening pelvic radiograph in detecting SCFE with hypothyroidism.
References
- 1.Loder RT. The demographics of slipped capital femoral epiphysis. An international multicenter study. Clin Orthop Relat Res 1996;322:8-27. [Google Scholar]
- 2.Song KS, Lim YW, Ok IY, Lee SW. Delayed-onset of slipped capital femoral epiphysis. J Orthop Sci 2015;20:78-86. [Google Scholar]
- 3.Yen PM. Physiological and molecular basis of thyroid hormone action. Physiol Rev 2001;81:1097-42. [Google Scholar]
- 4.Kadowaki S, Hori T, Matsumoto H, Kanda K, Ozeki M, Shirakami Y, et al. Prepubertal onset of slipped capital femoral epiphysis associated with hypothyroidism: A case report and literature review. BMC Endocr Disord 2017;17:59. [Google Scholar]
- 5.Macía-Villa CC, Sanchez-Lite I, Medina-Luezas J. Slipped capital femoral epiphysis in adults: Case report and review of literature. Reumatismo 2016;68:40-7. [Google Scholar]
- 6.Kocher MS, Bishop JA, Hresko MT, Millis MB, Kim YJ, Kasser JR. Prophylactic pinning of the contralateral hip after unilateral slipped capital femoral epiphysis. J Bone Joint Surg Am 2004;86:2658-65. [Google Scholar]
- 7.Huang YF, Wang LS, Zhang S, Gao YH, Liu JG, Qi X. Slipped capital femoral epiphysis in an adult with congenital hypopituitarism: A case report. Medicine (Baltimore) 2019;98:e13997. [Google Scholar]








