Anomalies of the laminae of the axis are rare, MRI and reconstructed CT scans are recommended as useful tools to develop treatment strategies.
Dr. Koki Kato, Department of Orthopaedic Surgery, Gifu Municipal Hospital, 7-1 Kashima-Cho, Gifu City, Gifu 500-8513, Japan. E-mail: koki.k.co@gmail.com
Introduction: Cervical myelopathy due to anomalies of the posterior elements of the axis is rare, and limited cases have been reported. This study reports such a unique case of congenital anomaly of the laminae of the axis, which is treated by partial removal of the anomalous bony structure surgically, and provides a comprehensive review of the present literature on this pathological condition.
Case Presentation:A 65-year-old man presented with a 3-year history of numbness in both arms with a sensory change in the right arm. Six months before admission, he noticed weakness in his right upper extremities and stiffness of the right lower extremity. Magnetic resonance imaging (MRI) showed a bilaterally compressed spinal cord with an anomalous bony structure at the C2-3 level. Computed tomography (CT) showed an invaginated abnormal bony structure at the C2-3 level and an abnormal lateral mass on the right side at the C2-3 level. The patient underwent posterior decompression surgery using the conventional open approach. One year after surgery, his myelopathy partially ameliorated, with his cervical radiograph showing no signs of the secondary instability and MRI showing sufficient decompression of the spinal cord. The age of onset, symptoms, and surgical treatment in our case was similar to those in the 14 previously reported cases; however, the morphology of the anomaly had variations.
Conclusion:This is a report of a rare anomaly in the laminae of the axis. MRI and reconstructed CT scans were useful for the treatment of this case. Partial surgical removal was an appropriate treatment for this patient, resulting in a satisfactory outcome.
Keywords: Cervical myelopathy, anomaly of axis, decompression.
Invaginated anomalies of the laminae of the axis are a rare cause of cervical myelopathy. To the best of our knowledge, 14 cases of invaginated anomalies of the laminae of the axis have been reported in the literature [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. However, there are many variations in this anomaly, and the pathology is still unclear. We describe an additional case of cervical myelopathy caused by invaginated laminae of the axis and present a comprehensive review of the literature.
A 65-year-old man presented with a 3-year history of numbness in both arms, with sensory changes in the right arm. Six months before admission, he noticed weakness in his right upper extremity and stiffness in the right lower extremity. No history of major trauma or viral infection was noted. Physical examination at admission revealed grade IV weakness of the right upper extremity, negative bilateral Hoffmann sign, positive Wartenberg sign on the right side, and hypoactive deep tendon reflexes in both the upper extremities.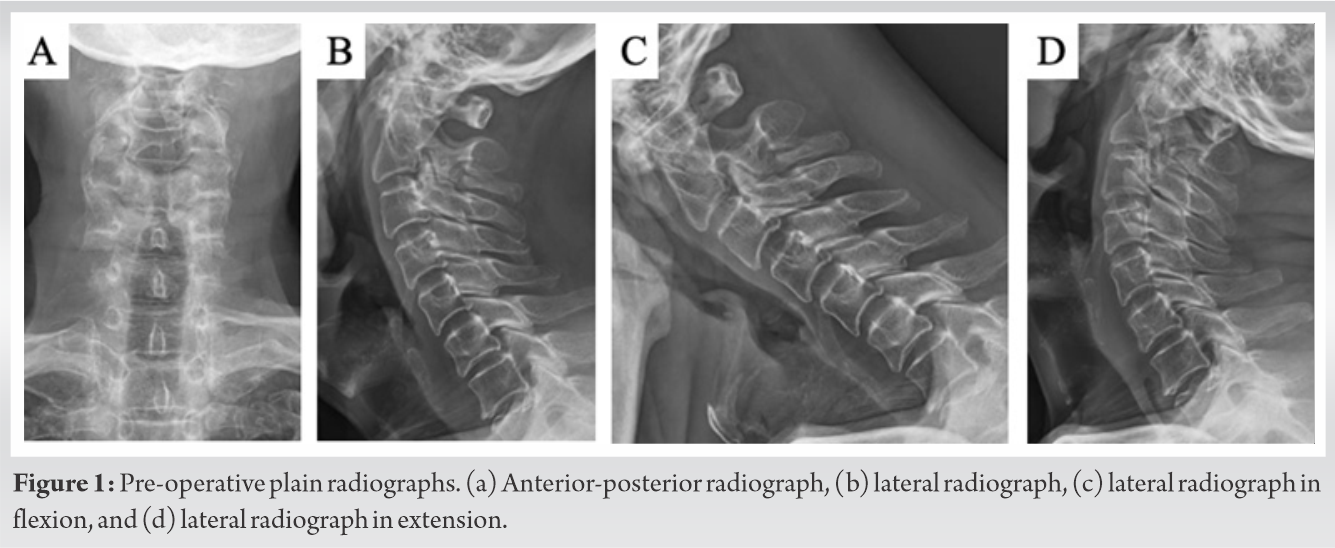
Anterior-posterior and lateral radiographs of the cervical spine showed an abnormal structure at the C2-3 level and did not show spina bifida at the cervical spine (Fig. 1-a, b). Lateral flexion-extension radiographs did not show instability of the cervical spine (Fig. 1-c, d). Magnetic resonance imaging (MRI) showed a bilaterally compressed spinal cord with an anomalous bony structure at the C2-3 level (Fig. 2-A, b, c). Computed tomography (CT) showed an invaginated abnormal bony structure at the C2-3 level and an abnormal lateral mass on the right side at the C2-3 level (Fig. 3-a, b, c, d, e). We did not perform nerve conduction studies or electromyography. The patient was diagnosed with cervical compressive myelopathy based on an anomaly between C2 and C3. The patient decided to undergo decompression surgery for removing the abnormal portion.
During surgery using the conventional posterior open approach, an abnormal bony structure was found at the C2-3 level. The connection between the abnormal bony structure and the C2/C3 laminae was not bony but fibrous. To decompress the dura mater, the abnormal bony structure was removed using a high-speed drill until 50% AP diameter of the dura mater was exposed, and sufficient decompression was confirmed. There were no adhesions between the dura mater and abnormal bony structure. After the removal of this fragment, we evaluated for intraoperative instability of the cervical spine at the C2-3 level by grasping and maneuvering the spinous process of C2 and C3. No instability was observed at this level, and instrumented fusion was not performed. One year after surgery, his myelopathy partially ameliorated, with his cervical radiograph showing no signs of the secondary instability, and MRI showing sufficient decompression of the spinal cord.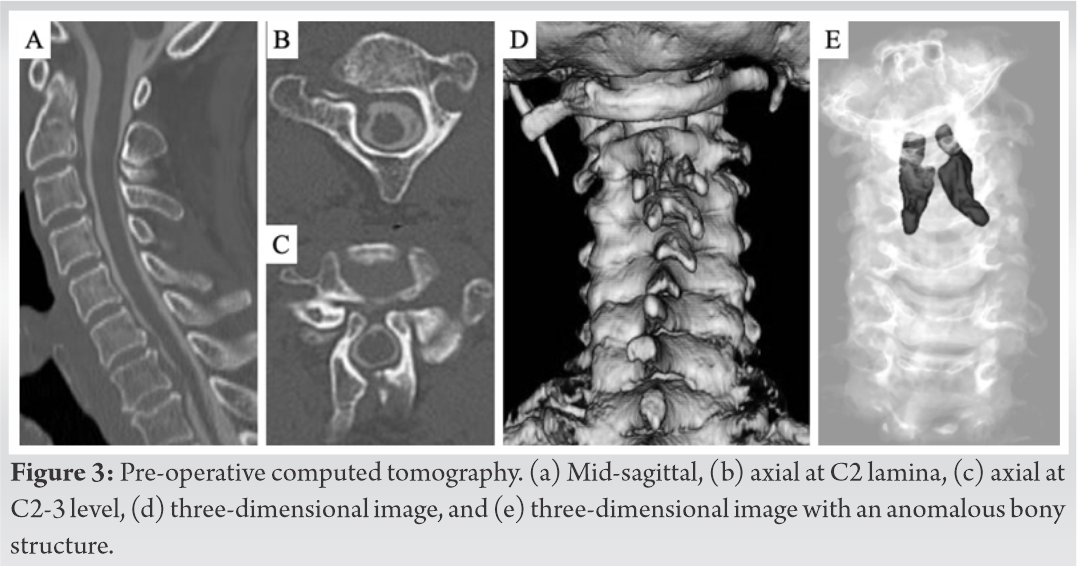
Congenital abnormalities of the axis are occasionally encountered and are categorized into irregular atlantoaxial segmentation, dens dysplasia, os odontoideum, hypoplasia and aplasia, and segmentation failure of C2 and C3 [14]. While these anomalies are located anteriorly, anomalies of the posterior elements of the axis are rare. Koyama et al. first reported a separated lamina of the axis invaginated into the canal in 1986 [1]. Subsequently, 14 cases of myelopathy caused by invaginated lamina of the axis were reported (Table 1) [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. While most anomalies of the axis are in combination with other anomalies (e.g., spina bifida and ossification of the posterior longitudinal ligament), cases of anomalies involving the axis alone are very rare [2, 7, 10]. Thus, reporting this case, along with a discussion, is worthwhile. Embryologically, anomalies of the lamina can be formed at the age of 7, when the posterior ossification centers fail to fuse to the body [7]. However, the data from 14 other cases and our case show that the manifestation of symptoms due to the anomaly of the axis occurs at later stages of life. In the previous reports, most patients were male and became aware of their symptoms at the fourth, fifth, sixth, or seventh decades of life [1, 2, 3, 4,7, 8, 9, 10, 12, 13]. Consistent with these reports, myelopathy developed in the fifth decade in our case. In contrast, Chau reported a case of a 14-year-old boy with aplasia of the atlas and defects of the posterior elements of the axis [5]. Similarly, Jiang et al. also reported a case of a 16-year-old boy with invaginated laminae of the axis in a spina bifida occulta and hypoplasia of the arch of the atlas [6]. Xu also reported a case of a 28-year-old man with invaginated laminae of the axis into the spinal canal and occipitalization of the atlas [11]. Although these cases had similar radiographic characteristics to ours, the patients were younger. The anomalies in these cases were found incidentally (two of them had a traumatic history). Therefore, age-related processes (such as chronic movement of the abnormal bone structure, ligament hypertrophy, and spondylotic change) in combination with the anomaly may cause myelopathy. In addition, since most reports are from Asia, it can be hypothesized that race may be a factor affecting this condition.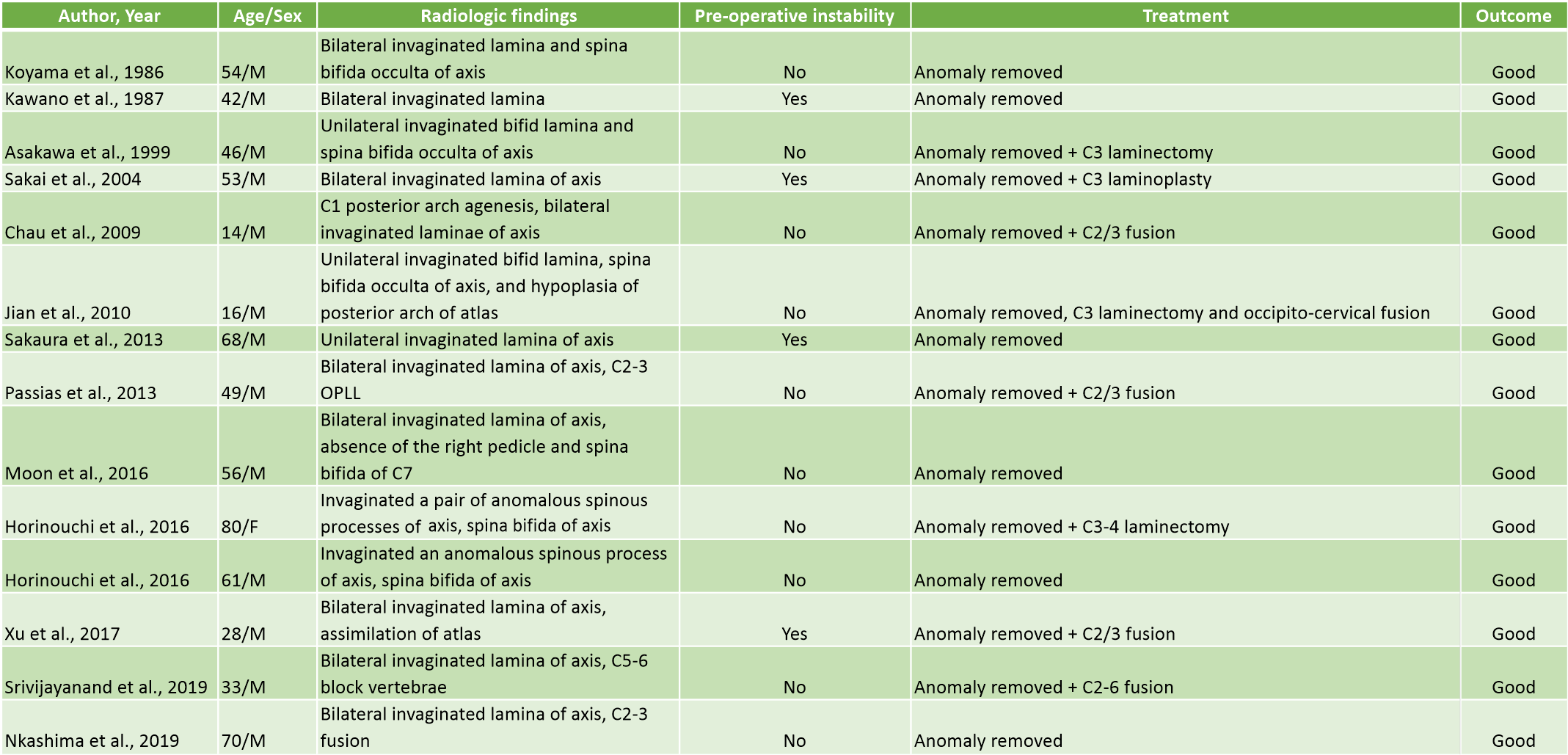 Most patients underwent decompressive surgery by removing the abnormal structure, with good outcomes [12, 3, 4, 6, 7, 9, 10, 13]. In the present case, the abnormal bone structure was partially removed. It was difficult to remove the abnormal bone en bloc, because the abnormal bone structure grew into the ventral side of the dura mater. However, four patients underwent decompressive and fusion surgery [5, 8, 11, 12]. Whether fusion surgery has to be performed seems to depend on segmental stability, age, patient’s expectation, surgeons’ experience, and so on [11]. Fusion surgery was not performed in our case, because there was no instability. Although the short-term outcome was satisfactory, and the patient’s cervical radiograph showed no signs of secondary instability, careful long-term follow-up is needed.
Most patients underwent decompressive surgery by removing the abnormal structure, with good outcomes [12, 3, 4, 6, 7, 9, 10, 13]. In the present case, the abnormal bone structure was partially removed. It was difficult to remove the abnormal bone en bloc, because the abnormal bone structure grew into the ventral side of the dura mater. However, four patients underwent decompressive and fusion surgery [5, 8, 11, 12]. Whether fusion surgery has to be performed seems to depend on segmental stability, age, patient’s expectation, surgeons’ experience, and so on [11]. Fusion surgery was not performed in our case, because there was no instability. Although the short-term outcome was satisfactory, and the patient’s cervical radiograph showed no signs of secondary instability, careful long-term follow-up is needed.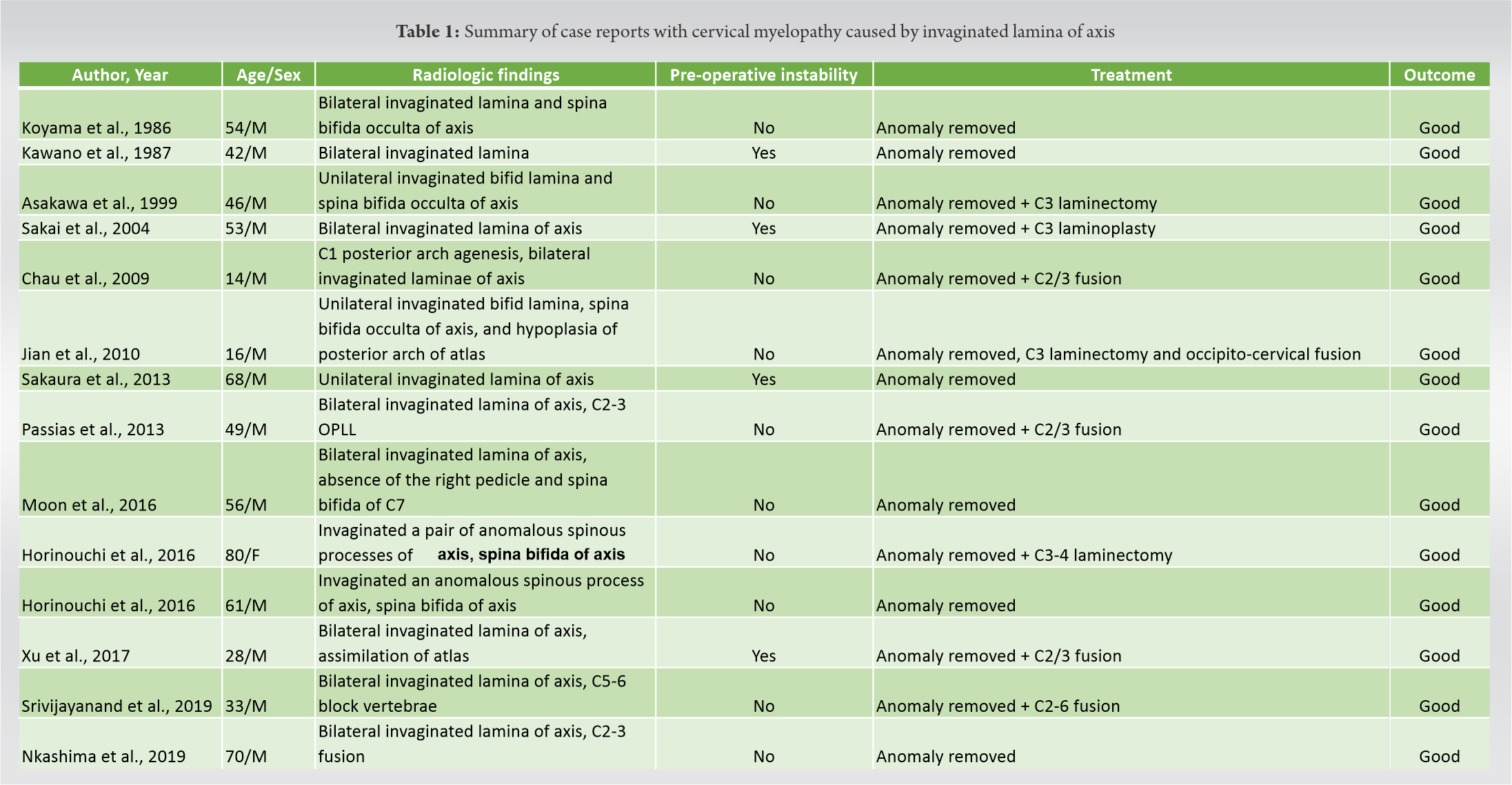
This is a report of a rare anomaly in the laminae of the axis. MRI and reconstructed CT scans are useful for the treatment of this case. Partial removal is an appropriate treatment for this patient, resulting in a satisfactory outcome.
Anomalies of the laminae of the axis are rare. MRI and reconstructed CT scans are recommended as useful tools to develop treatment strategies. The age-related process, in combination with an anomaly, may cause myelopathy.
References
- 1.Koyama T, Tanaka K, Handa J. A rare anomaly of the axis: Report of a case with shaded three-dimensional computed tomographic display. Surg Neurol 1986;25:491. [Google Scholar]
- 2.Kawano K, Uehara S, Nagata Y. A case of myelopathy due to a peculiar anomaly of the axis. No Shinkei Geka 1987;15:543. [Google Scholar]
- 3.Asakawa H, Yanaka K, Narushima K, Meguro K, Nose T. Anomaly of the axis causing cervical myelopathy. Case report. J Neurosurg 1999;91:121. [Google Scholar]
- 4.Sakai S, Sakane M, Harada S, Kaneoka K, Amano K, Ochiai N. A cervical myelopathy due to invaginated laminae of the axis into the spinal canal. Spine (Phila Pa 1976) 2004;29:E82. [Google Scholar]
- 5.Chau AM, Wong JH, Mobbs RJ. Cervical myelopathy associated with congenital C2/3 canal stenosis and deficiencies of the posterior arch of the atlas and laminae of the axis: Case report and review of the literature. Spine (Phila Pa 1976) 2009;34:E886. [Google Scholar]
- 6.Jiang Y, Xi Y, Ye X, Xu G, He H, Zhu Y. A cervical myelopathy caused by invaginated anomaly of laminae of the axis in spina bifida occulta with hypoplasia of the atlas: Case report. Spine (Phila Pa 1976) 2010;35:E351. [Google Scholar]
- 7.Sakaura H, Yasui Y, Miwa T, Yamashita T, Ohzono K, Ohwada T. Cervical myelopathy caused by invagination of anomalous lamina of the axis. J Neurosurg Spine 2013;19:694. [Google Scholar]
- 8.Passias PG, Wang S, Wang S. Combined ossification of the posterior longitudinal ligament at C2-3 and invagination of the posterior axis resulting in myelopathy. Eur Spine J 2013;22:S478. [Google Scholar]
- 9.Moon BJ, Choi KY, Lee JK. Cervical myelopathy caused by bilateral laminar cleft of the axis: Case report and review of literature. World Neurosurg 2016;93:487.e11. [Google Scholar]
- 10.Horinouchi Y, Tachibana T, Maruo K, Inoue S, Arizumi F, Kusuyama K, et al. A cervical myelopathy associated with an anomaly of the axis: Two case reports of invaginated spinous process of the axis with spina bifida into the spinal canal. J Orthop Sci 2016;21:557. [Google Scholar]
- 11.Xu JX, Wang CG, Zhou CW, Tang Q, Li JW, Xu HZ, et al. Cervical myelopathy caused by invaginated laminae of the axis associated with occipitalizaion of the atlas: Case report and literature review. Medicine (Baltimore) 2017;96:e9156. [Google Scholar]
- 12.Srivijayanand KS, Vivekanandaswamy AN, Shetty AP, Kanna RM, Rajasekaran S. Progressive hemiparesis due to spino-laminar anomaly of the axis-a case report and literature review. Spinal Cord Ser Cases 2019;5:69. [Google Scholar]
- 13.Nakashima T, Otsuki B, Shimizu T, Fujibayashi S, Murata K, Matsuda S. Cervical myelopathy caused by invagination of floating anomalous C2 and C3 laminae in the spinal canal. Spine Surg Relat Res 2020;4:274. [Google Scholar]
- 14.Vangilder JC, Menezes AH. Craniovertebral junction abnormalities. Clin Neurosurg 1983;30:514. [Google Scholar]