
Optimal clinicoradiological outcome in such uncommon fracture phenotype depends on accurate pre-operative planning with CT scan and rigid anatomical reconstruction of the tuberosities for faster rehabilitation.
Dr. Sameer Panchal, Department of Orthopedics, Grant Government Medical College & Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: panchalsameer1992@gmail.com
Introduction: Combined fracture of greater and lesser tuberosity is an extremely rare injury. Such fracture pattern has not been described in the Neer’s, AO Muller, and Jakob’s classification system.
Case Presentation:We report a unique fracture pattern consisting of combined greater and lesser tuberosity of the proximal humerus (PH) with intact humeral head and shaft in a 32-year-old female. Routine radiographs and computed tomography scan with three-dimensional reconstruction were advised for better understanding of the fracture pattern, later managed by open reduction and fixation with PH locking plate. The patient has excellent clinical, radiological, and functional outcome at the end of 2 years follow-up.
Conclusion: This is one among the few case reports highlighting this unique variant of PH fracture, not much has been described in the literature about this injury. Anatomic reconstruction of the fractured tuberosities combined with stable construct by PH locking plate facilitates optimum bone healing and aggressive shoulder rehabilitation.
Keywords: Greater tuberosity, humeral head, lesser tuberosity, proximal humerus fracture.
Combination of greater and lesser tuberosity fracture in isolation with head shaft continuity is an infrequent phenomenon [1]. Combined tuberosity fractures are often seen concomitantly with anterior or posterior shoulder dislocations. Precise diagnosis and assessing the degree of displacement of lesser tuberosity are difficult on plain radiographs, hence, multiple slice computerized tomography (CT) scan is must for lucid understanding of fracture morphology. Accurate appreciation of such fracture patterns aids in faultless surgical planning and execution. We report a case of displaced fracture of greater as well as lesser tuberosity of the proximal humerus (PH) with no evidence of shoulder dislocation and discontinuity between humeral head and shaft.
A 32-year-old right hand dominant female, housemaid by occupation, presented to our outpatient department with pain in the right shoulder and restricted range of motion for 1.5 months. She had a history of fall from stairs 1.5 months back and sustained direct blow to the right shoulder for which she was managed conservatively at local hospital. On clinical examination, she had tenderness over the anterolateral aspect of the right shoulder and abduction, internal rotation and external rotation movements were restricted. There was no associated neurovascular deficit.
Initial impression on plain radiograph anteroposterior (AP) view of the right shoulder showed displaced greater tuberosity fracture with no other obvious bony injury (Fig. 1). CT scan with sagittal and axial cuts demonstrated comminuted greater tuberosity fracture and displaced lesser tuberosity fracture with head shaft in continuity (Fig. 2a-d). CT scan with three-dimensional reconstruction (3-D) was done for further understanding of fracture configuration which confirmed fracture of greater tuberosity which was displaced 10 mm superiorly and 5 mm posteriorly, furthermore, to our surprise, lesser tuberosity fracture displaced 6 mm medially was also noticed (Fig. 3). It also confirmed that there was no impacted fracture between the humeral head and shaft. Open reduction and rigid internal fixation and anatomical reconstruction of tuberosities were the pre-operative plan. The patient underwent surgery under general anesthesia through deltopectoral approach after obtaining written informed consent. The greater tuberosity was displaced superiorly and posteriorly due to the pull by supraspinatus. The lesser tuberosity was displaced medially due to subscapularis attachment. Ethibond (polyester) suture no. 5 was passed through the subscapularis tendon and lesser tuberosity was secured. Greater tuberosity was reduced anatomically with the help of Ethibond no.5 passed through the supraspinatus bone tendon junction. The reduction of greater tuberosity was held temporarily with Kirschner wires. PH locking plate was applied and the Ethibond sutures were passed through islets of the plates (Fig. 4). Reconstruction of both the tuberosities and stability of the construct was confirmed under fluoroscopy.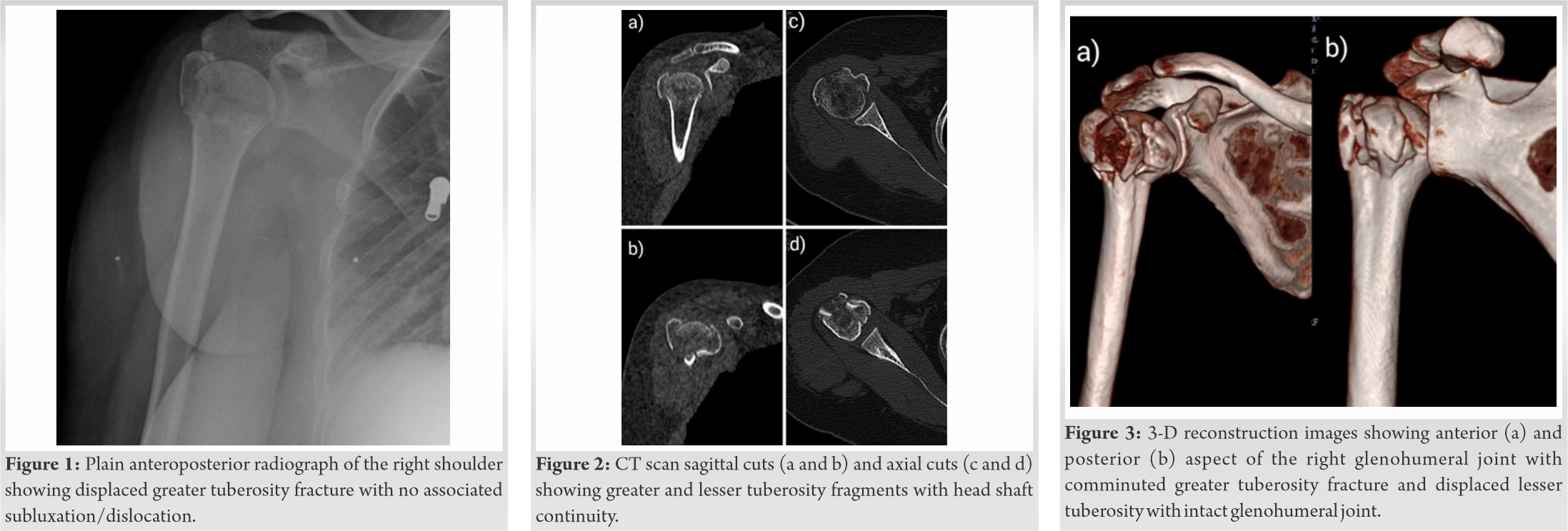
Postoperatively, pendulum exercises were started from the 2nd post-operative day. Shoulder range of motion exercises (active and passive) were started from the 2nd week. At 2 years follow-up, plain radiographs of the right shoulder confirmed united greater and lesser tuberosities (Fig. 5a, 5b). Functional outcome assessed by shoulder range of motion during final follow-up revealed abduction of 160°, flexion of 140° and 30° degrees of internal and external rotations, and excellent UCLA score of 30 (range 16–35).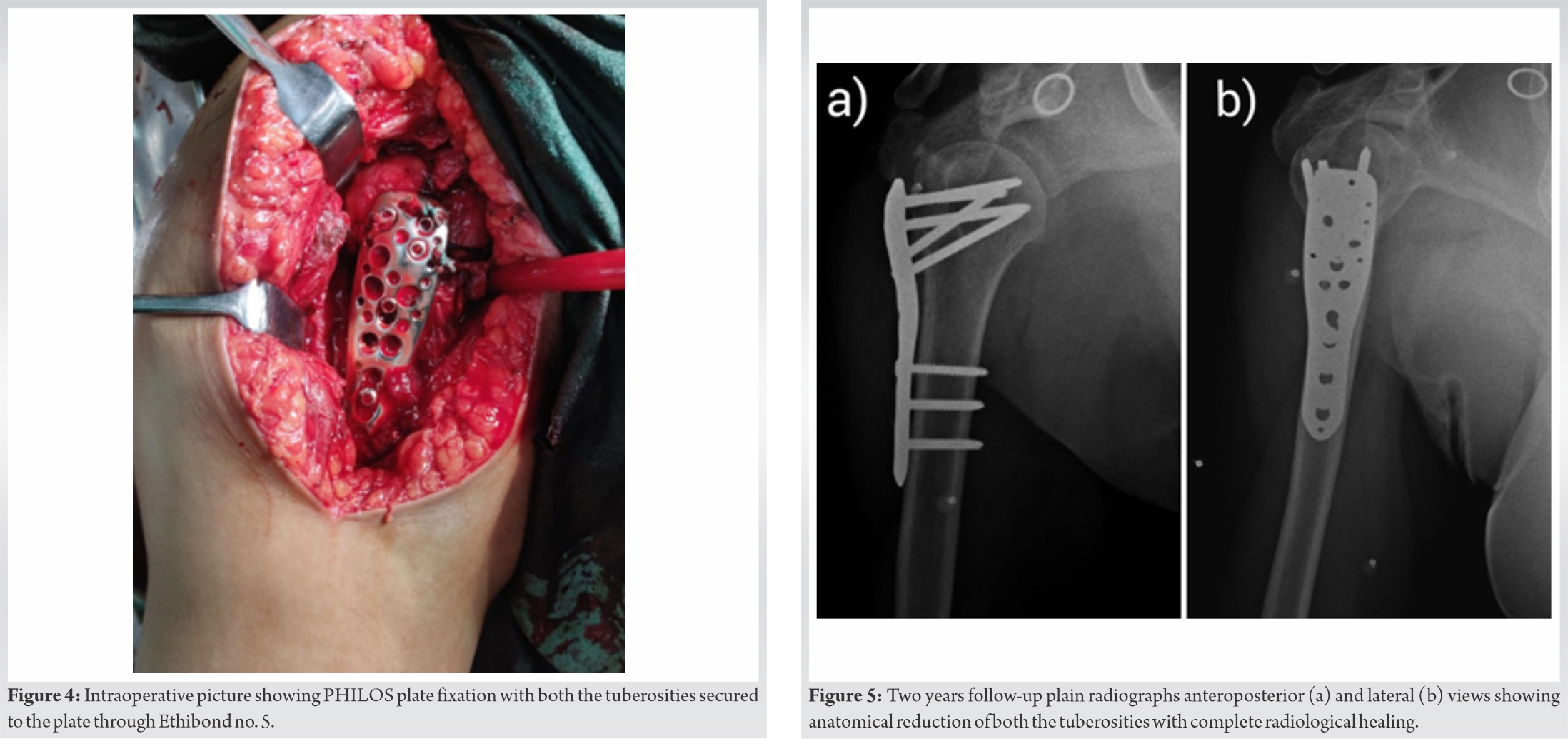
A combined fracture of greater and lesser tuberosity is an extremely uncommon injury due to different injury mechanisms for both. Lesser tuberosity fractures which are commonly associated with posterior glenohumeral dislocation usually occur due to contraction of subscapularis muscle when the arm is forced into abduction and external rotation. Approximately 5–30% of anterior shoulder dislocations are complicated by greater tuberosity fractures [2]. Greater tuberosity fracture occurs with a fall on the outstretched hand with the elbow in full extension or flexion or after a direct blow to the lateral aspect of the shoulder. Another reason for their rarity is that they predominantly occur in the young age group, elderly people with osteoporosis usually had three- or four-part PH fracture (PHF) or associated rotator cuff tendon tear [3]. Combined tuberosity fracture with intact humeral shaft is not mentioned in Neer, AO Muller, and Jakob classification [4, 5, 6], few of the commonly followed classification systems for PHFs. In 1934, Codman divided PH into four separate fragments – head, greater tuberosity, lesser tuberosity, and shaft. According to his classification, there are 14 different fracture types possible [7]. This unique fracture pattern can be allocated under Codman’s classification system. Operative treatment is indicated if greater tuberosity is displaced by 5 mm or displaced by 3 mm in the case of athletes due to the risk of rotator cuff dysfunction [8]. In lesser tuberosity, fracture operative treatment is recommended for fragment displacement by 5 mm or 45° of angulation, mechanical block to internal rotation, and weakness of terminal internal rotation [9]. The majority of lesser tuberosity fractures are often missed on initial plain radiographs so CT scan with 3-D helps to confirm diagnosis [10]. There are few case reports of combined tuberosity fracture mentioned in the literature [1, 10, 11, 12]. Takase et al. reported a case of combined fracture of greater and lesser tuberosity with head shaft continuity which was managed with screws [13]. Arthroscopic evaluation of the affected glenohumeral joint was done simultaneously to further understand the mechanism of injury and the examination did not reveal any defects, thinning or damage to the articular cartilage, or superior labrum AP lesions. Based on the above findings, they concluded that this rare fracture pattern was not associated with shoulder dislocation. Pauly et al. managed a similar case by arthroscopic fixation of both the tuberosities through suture anchors [11]. They concluded that in such rare scenario, arthroscopic fixation allows for better visualization and anatomical refixation of the fractured tuberosity as well as therapy for concomitant intra-articular lesions. Meyer et al. reported a similar case a combined tuberosity fracture in a 44-year-old female managed by open reduction and internal fixation using two screws and anatomical reconstruction of tuberosities by reattaching them with sutures [12]. The mechanism of injury in their case was road traffic accident. In our case, the patient presented to us 1.5 months after the index injury with poor shoulder function and imaging revealed comminuted greater tuberosity fragment, hence, open reduction with stable internal fixation by PHILOS plate and anatomic reconstruction of fractured tuberosities with Ethibond sutured over the plate were planned to promote aggressive post-operative rehabilitation which has ultimately led to acceptable clinical, radiological, and functional outcome at the end of 2-year follow-up.
Combined tuberosity fracture is a distinctive fracture pattern not described well in literature that requires biomechanical in vitro studies to appreciate mechanism of injury, better radiological imaging modalities to understand the fracture anatomy, and meticulous execution of surgical procedure, leading to anatomical reconstruction of both the tuberosities for optimal clinical and functional outcome.
This rare fracture configuration requires surgical intervention in the form of anatomical reconstruction of greater and lesser tuberosity for optimal functional outcome. Understanding the pathomechanics and diagnosing this fracture type by various radiological modalities allow for pertinent surgical planning and execution.
References
- 1.Robinson M, Teoh KH, Baker A, Bell L. Fractures of the lesser tuberosity of the humerus. J Bone Joint Surg Am 2009;91:512-20. [Google Scholar]
- 2.George MS. Fractures of the greater tuberosity of the humerus. J Am Acad Orthop Surg 2007;15:607-13. [Google Scholar]
- 3.Bahrs C, Rolauffs B, Stuby F, Dietz K, Weise K, Helwig P. Effect of proximal humeral fractures on the age-specific prevalence of rotator cuff tears. J Trauma 2010;69:901-6. [Google Scholar]
- 4.Jakob RP, Kristiansen T, Mayo K, Ganz R, Muller ME, Bateman JE, et al. Surgery of the Shoulder. Philadelphia, PA: BC Decker; 1984. [Google Scholar]
- 5.Müller ME, Koch P, Nazarian S, Schatzker J. The Comprehensive Classification of Fractures of Long Bones. Berlin, Heidelberg: Springer; 1990. [Google Scholar]
- 6.Neer CS 2nd. Displaced proximal humeral fractures. I. Classification and evaluation. J Bone Joint Surg Am 1970;52:1077-89. [Google Scholar]
- 7.Codman EA. Fractures in relation to the subacromial bursa. In: Codman EA, editors. The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in or About the Subacromial Bursa. Boston, MA: Thomas Todd; 1934. p. 313-33. [Google Scholar]
- 8.Park TS, Choi IY, Kim YH, Park MR, Shon JH, Kim SI. A new suggestion for the treatment of minimally displaced fractures of the greater tuberosity of the proximal humerus. Bull Hosp Jt Dis 1997;56:171-6. [Google Scholar]
- 9.Gruson KI, Ruchelsman DE, Tejwani NC. Isolated tuberosity fractures of the proximal humeral: Current concepts. Injury 2008;39:284-98. [Google Scholar]
- 10.Ogawa K, Takahashi M. Long-term outcome of isolated lesser tuberosity fractures of the humerus. J Trauma 1997;42:955-9. [Google Scholar]
- 11.Pauly S, Herrmann S, Perka C, Greiner S. Arthroscopic refixation of a combined fracture of the greater and lesser tuberosity of the proximal humerus. Knee Surg Sports Traumatol Arthrosc 2013;21:1171-5. [Google Scholar]
- 12.Meyer DC, Espinosa N, Hertel R. Combined fracture of the greater and lesser tuberosities with intact connection of the humeral head to the shaft. J Trauma 2006;61:206-8. [Google Scholar]
- 13.Takase K, Shinmura K, Yamamoto K. A combined fracture of the greater and lesser tuberosity with head shaft continuity in the proximal humerus. Arch Orthop Trauma Surg 2007;127:895-8. [Google Scholar]







