
Despite substantial advances in ceramic materials, catastrophic failure of fourth generation ceramic head components can occur in dual mobility constructs.
Dr. Michael J. Patetta, Department of Orthopaedics, University of Illinois at Chicago, 835 S. Wolcott Avenue., E270 MSS MC 844, Chicago 60612, Illinois. E-mail: michaelpatetta@gmail.com
Introduction: Rare cases of Biolox® delta ceramic head fractures in ceramic-on-polyethylene bearings have been reported in the literature. Virtually none of these catastrophic injuries have been documented in dual mobility constructs.
Case Report:We report a case of fourth-generation delta ceramic head fracture 4.5 years after implantation in a dual mobility total hip replacement constructs as a result of a ground-level fall. The patient underwent revision arthroplasty with another delta ceramic dual mobility construct and was able to return to work in custodial services 2 weeks after the revision procedure.
Conclusion:In summary, we presented an extremely uncommon case of a fractured fourth generation, Biolox® delta ceramic head in a dual mobility total hip arthroplasty (THA), as a result of a ground-level fall. The patient underwent successful revision surgery to another dual mobility delta ceramic THA. Despite substantial advances in ceramic materials, catastrophic failure of 4th generation ceramic head components can still occur even in dual mobility constructs and require revision arthroplasty surgery.
Keywords:Total hip arthroplasty, revision total hip arthroplasty, ceramic femoral head, dual mobility cup.
While each successive generation of ceramic design had led to reductions in fracture rate, little is known about fracture incidence in fourth-generation components [1]. Rates of fourth-generation ceramic head fractures are reported at <0.01, and evaluation of rates in dual-mobility constructs are even more scarce [2, 3].
A 45-year-old African American male presented with right hip pain secondary to avascular necrosis of the femoral head, with collapse (Fig. 1). The patient failed conservative treatment including physical therapy, non-steroidal anti-inflammatory medications, and a fluoroscopic-guided intra-articular corticosteroid injection, and elected to proceed with total hip arthroplasty (THA).
The index THA was performed through a standard posterolateral approach. A Stryker modular dual mobility (MDM) THA construct was selected. A Stryker Accolade 2, size #6, 132° neck angle femoral component was paired with a Biolox® delta ceramic 28 mm head, 0mm neck length. The stem is made of a titanium-based alloy which includes aluminum and vanadium and has a 5˚40’ taper with a smooth surface finish. The dual mobility polyethylene inserts measured 28 mm in inner diameter and 48 in outer diameter and articulated with the MDM cobalt-chromium liner. A 54 mm titanium acetabular shell was impacted into the bony acetabulum using press-fit technique and two 6.5 mm cancellous screws were used. At the conclusion of the case, all components were deemed well-fixed, and the patient demonstrated appropriate leg length and range of motion intraoperatively (Fig. 2). Upon discharge, the patient maintained standard post-operative hip precautions and attended outpatient physical therapy. He was seen in clinic for routine post-operative care at the 3-week, 6-week, 3-month, and 9-month marks.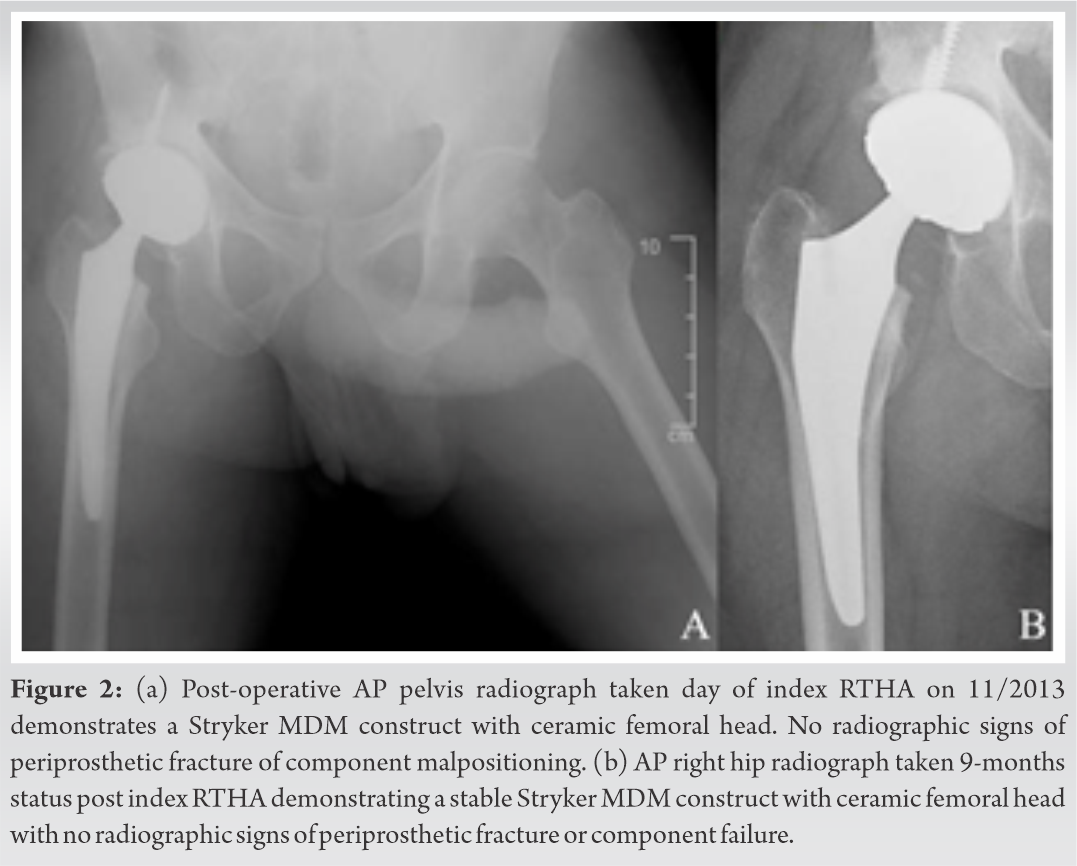
At 28 months, the patient returned to clinic with “mild right hip pain”. Infectious workup was negative and a bone scan failed to identify any evidence of component losing. The patient was subsequently lost to follow-up until 4.5 years post-operative, when he presented to the emergency department after tripping and falling onto his right hip. He reported severe pain in the right groin immediately after falling with an inability to bear weight. Radiographs revealed gross deformity of the right femoral head, with fine, radiopaque particles adjacent to the joint (Fig. 3). CT scan confirmed fragmentation of the delta ceramic head without signs of other component failure or loosening (Fig. 3). At the time, the patient refused urgent surgical management before agreeing to revision THA at his outpatient follow-up 2 days later.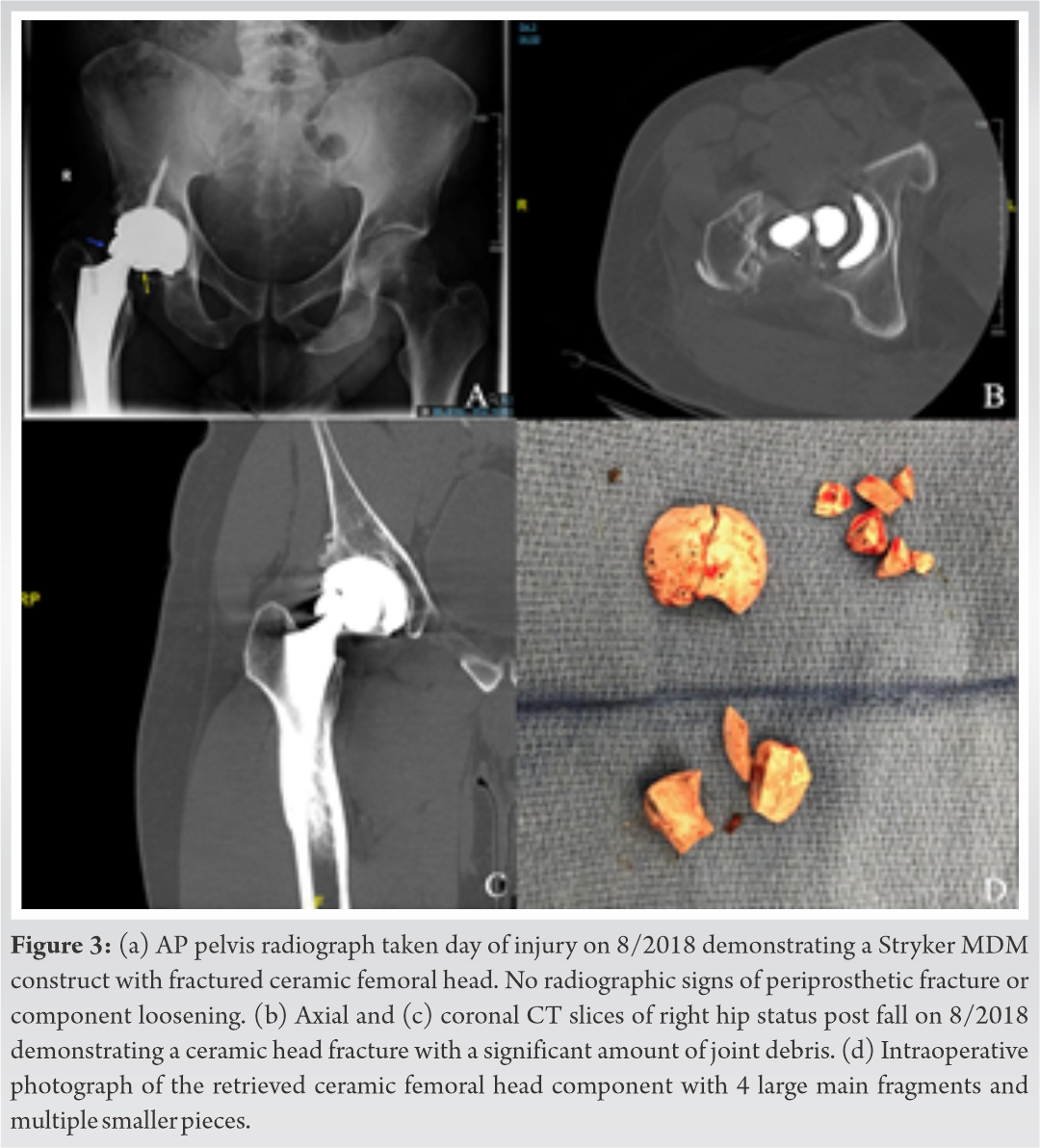
The previous posterolateral incision was utilized for the revision. Examination of the ceramic femoral head revealed 4 large main fragments with multiple smaller pieces (Fig. 3). After removal of the polyethylene and fragmented ceramic components, the metallic liner was evaluated and deemed to be securely fixed in place. The acetabular shell and femoral stem components were ingrown and well-fixed. The femoral component taper did not show any severe corrosion. Extensive synovectomy and irrigation were performed to ensure the removal of any remaining ceramic fragments. Trials of the original sized components demonstrated good stability. Thus, replacement 28 mm +0 Biolox® delta ceramic femoral head, Stryker Universal Titanium Taper Adapter, and Restoration MDM polyethylene liner (inside diameter 28 mm, outside diameter 48 mm) were implanted. At the 2-week follow-up, the patient expressed his pain was well controlled. He was able to ambulate without an assistive device and felt well enough to return to his occupation in custodial services. He was still doing well based on follow-up telephone encounter 2 years post revision THA without any significant hip pain or functional limitations.
One of the challenges remaining in total joint arthroplasty is creating a device capable of withstanding the higher demand and greater chronic wear associated with younger patients. Many combinations of ultra-high molecular weight polyethylene (UHMWPE), metal, and ceramic components are currently available, with variation in alloys, composition, and manufacturing techniques in each of these materials [4]. By principle, ceramic bearings feature the most favorable volumetric wear properties. However, poor intrinsic toughness leaves ceramics more susceptible to fracture and catastrophic failure than their UHMWPE and metallic counterparts.
Modern ceramics, such as the fourth-generation Biolox® delta component used in this case, feature additions of zirconium (17%), chromium oxide (0.3%), and strontium (0.6%) to increase toughness and limit fracture propagation. Analysis of the French National Agency for Safety of Drugs and Medical Products (ANSM) registry revealed a rate of head fractures of 0.0013% for 4th generation ceramic, compared with a rate of 0.002% reported by the manufacturer [2]. In a review of the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man, fractures in 7 of 79,442 implanted Biolox® delta heads (0.009%) were reported in ceramic-on-ceramic THA [3]. Both studies reported improved head fracture rates compared to 3rd generation ceramic implants. In addition, a recent retrieval study also demonstrated retention of burst strength of Biolox® delta heads after several years of in-vivo use, with the lowest of 28 heads tested failing at a burst load over forty times the force generated by a 75 kg adult during stair ascent [5]. Rare cases of delta ceramic head fractures in ceramic-on-polyethylene THA have been reported, but to our knowledge, this is the first report of delta ceramic head fracture in a dual mobility primary THA construct [1, 6, 7]. Dual mobility acetabular components were initially designed to reduce post-operative dislocation, to better restore range of motion of the hip, and to reduce prosthesis stresses in THA [8]. As opposed to conventional THA, which features articulation of a femoral head component into a fixed insert component, dual mobility prostheses allow mobility of the polyethylene insert, which, in addition to articulating with the femoral head inside it, articulates with a fixed acetabular shell component, with or without a fixed metal liner. Long-term data demonstrates a significantly decreased revision rate in dual mobility THA when matched with conventional THA [9]. Additionally, dual mobility constructs have shown promising short-term results in patients requiring replacement due to osteonecrosis of the femoral head, as was seen in our patient [10]. Our case demonstrates rare catastrophic failure of a Biolox® delta femoral head in a dual mobility THA construct. While atraumatic failures have been reported, our case was likely secondary to a traumatic etiology [11]. Our revision procedure including copious irrigation and debridement, selection of new ceramic component with titanium taper sleeve, and retention of stable hardware, was consistent with previous suggestions on how to address this atypical scenario [12]. Severe, complication rates of ceramic head fracture revision procedures have been reported to be as high as 29% [13].
In summary, we presented an extremely uncommon case of a fractured fourth generation, Biolox® delta ceramic head in a dual mobility THA, as a result of a ground-level fall. The patient underwent successful revision surgery to another dual mobility delta ceramic THA. Despite substantial advances in ceramic materials, catastrophic failure of 4th generation ceramic head components can still occur even in dual mobility constructs and require revision arthroplasty surgery.
Orthopedic surgeons must recognize that fractures of ceramic femoral heads remain a rare, but devastating complication despite advancements in Biolox® delta engineering and in a dual mobility implant systems.
References
- 1.Rankin CS, Robinson PG, Beattie N, Gaston P. Fracture of a BIOLOX delta ceramic femoral head: A case report and update of the literature. JBJS Case Connect 2019;9:1-5. [Google Scholar]
- 2.Massin P, Lopes R, Masson B, Mainard D. Does Biolox® Delta ceramic reduce the rate of component fractures in total hip replacement? Orthop Traumatol Surg Res 2014;100:S317-21. [Google Scholar]
- 3.Howard DP, Wall PD, Fernandez MA, Parsons H, Howard PW. Ceramic-on-ceramic bearing fractures in total hip arthroplasty. Bone Joint J 2017;99B:1012-9. [Google Scholar]
- 4.López-López JA, Humphriss RL, Beswick AD, Thom HH, Hunt LP, Burston A, et al. Choice of implant combinations in total hip replacement: Systematic review and network meta-analysis. BMJ 2017;359:j4651. [Google Scholar]
- 5.Nguyen TM, Weitzler L, Esposito CI, Porporati AA, Padgett DE, Wright TM. Zirconia phase transformation in zirconia-toughened alumina ceramic femoral heads: An implant retrieval analysis. J Arthroplast 2019;34:3094-8. [Google Scholar]
- 6.Pomeroy E, Rowan F, Masterson E. Atraumatic fracture of a BIOLOX delta ceramic femoral head articulating with a polyethylene liner. JBJS Case Connect 2015;5:1-6. [Google Scholar]
- 7.Heiner AD, Mahoney CR. Fracture of a BIOLOX delta ceramic femoral head articulating against a polyethylene liner: A case report. JBJS Case Connect 2014;4:1-6. [Google Scholar]
- 8.Neri T, Philippot R, Klasan A, Putnis S, Leie M, Boyer B, et al. Dual mobility acetabular cups for total hip arthroplasty: Advantages and drawbacks. Expert Rev Med Devices 2018;15:835-45. [Google Scholar]
- 9.Jobory A, Kärrholm J, Overgaard S, Pedersen AB, Hallan G, Gjertsen JE, et al. Reduced revision risk for dual-mobility cup in total hip replacement due to hip fracture: A matched-pair analysis of 9,040 cases from the nordic arthroplasty register association (NARA). J Bone Joint Surg Am 2019;101:1278-85. [Google Scholar]
- 10.Assi C, Kheir N, Samaha C, Kouyoumdjian P, Yammine K. Early results of total hip arthroplasty using dual-mobility cup in patients with osteonecrosis of the femoral head. Sicot J 2018;4:37. [Google Scholar]
- 11.Kocadal O, Ozler T, Bolukbasi AE, Altintas F. Non-traumatic ceramic head fracture in total hip arthroplasty with ceramic-on-ceramic articulation at postoperative 16th years. Hip Pelvis 2019;31:124. [Google Scholar]
- 12.Traina F, Tassinari E, De Fine M, Bordini B, Toni A. Revision of ceramic hip replacements for fracture of a ceramic component: AAOS exhibit selection. J Bone Joint Surg A 2011;93:1-9. [Google Scholar]
- 13.Koo KH, Ha YC, Kim SY, Yoon KS, Min BW, Kim SR. Revision of ceramic head fracture after third generation ceramic-on-ceramic total hip arthroplasty. J Arthroplast 2014;29:214-8. [Google Scholar]






