
Multiple myeloma can present with osteosclerotic lesions and these are associated with POEMS syndrome and rarely with light chain myeloma.
Dr. Siddharth N Aiyer, Department of Spine, Sancheti Institute for Orthopaedics and Rehabilitation, Pune - 411 005, Maharashtra, India. E-mail: aiyer.siddharth@gmail.com
Introduction:Multiple myeloma is a plasma cell neoplasm that is commonly associated with lytic bone lesions; however, osteosclerotic multiple myeloma is a rare entity. Osteosclerotic multiple myeloma has been reported in association with POEMS syndrome.
Case Presentation: A 60-year-old female patient presented to us with low back pain for 2 months. The investigations revealed that the patient had multiple osteosclerotic lesions in the axial skeleton with a L4 ivory vertebra. The serum immunoelectrophoresis was negative. Positron emission tomography scan was done which showed multiple skeletal lesions in the right iliac bone, left femoral neck, thoracic vertebrae T1, T6, T12, and lumbar vertebra L4. Biopsy and immunohistochemistry of the lesion showed plasma cell proliferation; producing lambda light chains. However, there were no features of POEMS syndrome including polyneuropathy, organomegaly, endocrinopathy, and skin changes. The patient was started on chemoradiation and achieved clinical remission and was asymptomatic at 12 months follow-up.
Conclusion:Osteosclerotic myeloma without the features of POEMS syndrome is an extremely rare entity. This case reports documents a unique clinical scenario of osteosclerotic non-secretory light chain myeloma without POEMS syndrome.
Keywords: Osteosclerotic myeloma, multiple myeloma, oncology, POEMS syndrome, light chain disease.
Multiple myeloma is a common primary hematological malignancy arising due to proliferation of plasma cells, which secrete monoclonal immunoglobulins or immunoglobulin light chains (kappa/lambda) [1]. Plasma cell neoplasms constitute a common primary bone neoplasm and more than 90% of these tumors show the clinical and radiological features of multiple myeloma [2]. Multiple myeloma commonly forms osteolytic lesions, although in 1–3% of patients, it may be associated with osteosclerotic lesions. These osteosclerotic lesions have been reported in two groups; (a) focal osteosclerotic lesions associated with POEMS syndrome and (b) myeloma with diffuse osteosclerosis [3]. POEMS syndrome is an acronym to describe a spectrum of clinical features that occur in a subset of myeloma patients which include polyneuropathy, organomegaly, endocrinopathy, multiple myeloma, and skin changes [4].
The term “myeloma variant” is used to describe plasma cell neoplasms other than classical multiple myeloma. These variants are generally less aggressive and, in some instances, they are referred to as plasma cell dyscrasias because they may not be true neoplasms [2]. Although, most of the myeloma variants later develop into classical myeloma, this occurrence is rare in sclerotic variants [2]. The cause of osteosclerosis in POEMS syndrome has not been clearly understood, however, high serum levels of vascular endothelial growth factor (VEGF) which is an important cytokine produced by megakaryocytes and osteoblasts have been implicated [5]. We describe a rare case of light chain myeloma with multiple osteosclerotic lesions without features of POEMS syndrome in a 60-year-old female.
A 60-year-old female patient presented with low back pain of 4 months duration. Pain was diffusely spread over the entire low back and buttocks. There was no radiculopathy, neurogenic claudication, constitutional symptoms, or previous history of any malignancy.
On physical examination, the patient had tenderness over the lumbar region with a normal neurological examination. There was no lymphadenopathy, organomegaly, or skin abnormality. The patient was investigated with plain radiographs and MRI of the lumbar spine, which showed an osteosclerotic lesion in the L4 vertebra and iliac bone (Fig. 1). The laboratory test results revealed a normal result for a complete hemogram, thyroid function tests, renal function tests, and liver function tests. Erythrocyte sedimentation rate (ESR) was 6 mm/h, C-reactive protein <4 mg/dl, and normal serum calcium is 9.4 mg/dl. Serum triglycerides were high at 391 mg/dl, Vitamin D3 was 29.4 ng/ml, serum phosphorus was 4.5 mg/dl, and serum parathormone levels were raised 157 pg/ml. Urine Bence–Jones protein test was negative. Positron emission tomography (PET) scan was done which showed multiple osteosclerotic skeletal lesions in the right iliac bone, left femoral neck, thoracic vertebrae T1, T6, T12, and lumbar vertebra L4.
The patient underwent a transpedicular biopsy from L4 vertebra using a Jamshidi needle, as it showed the highest metabolic activity (SUV max 10.2) on PET scan. Two bone cores were obtained from the L4 vertebral body and sent for histopathological examination (HPE). Bone marrow was aspirated from the right iliac crest at the same time and sent for analysis. Bone marrow aspirate showed hypercellular marrow with increase in plasma cells at 9%. Serum immunoelectrophoresis was negative for M-band isolation.
Immunohistochemistry of the bone core sample was positive for CD138, CD38, MUM-1, lambda light chains, and negative for kappa light chains suggesting the diagnosis of plasma cell dyscrasias producing lambda light chains (Fig. 2). The serum light chain assay showed increased levels of lambda chains. The patient was started on chemotherapy for light chain myeloma and underwent clinical remission. She had relief of symptoms and was asymptomatic at last follow-up of 12 months.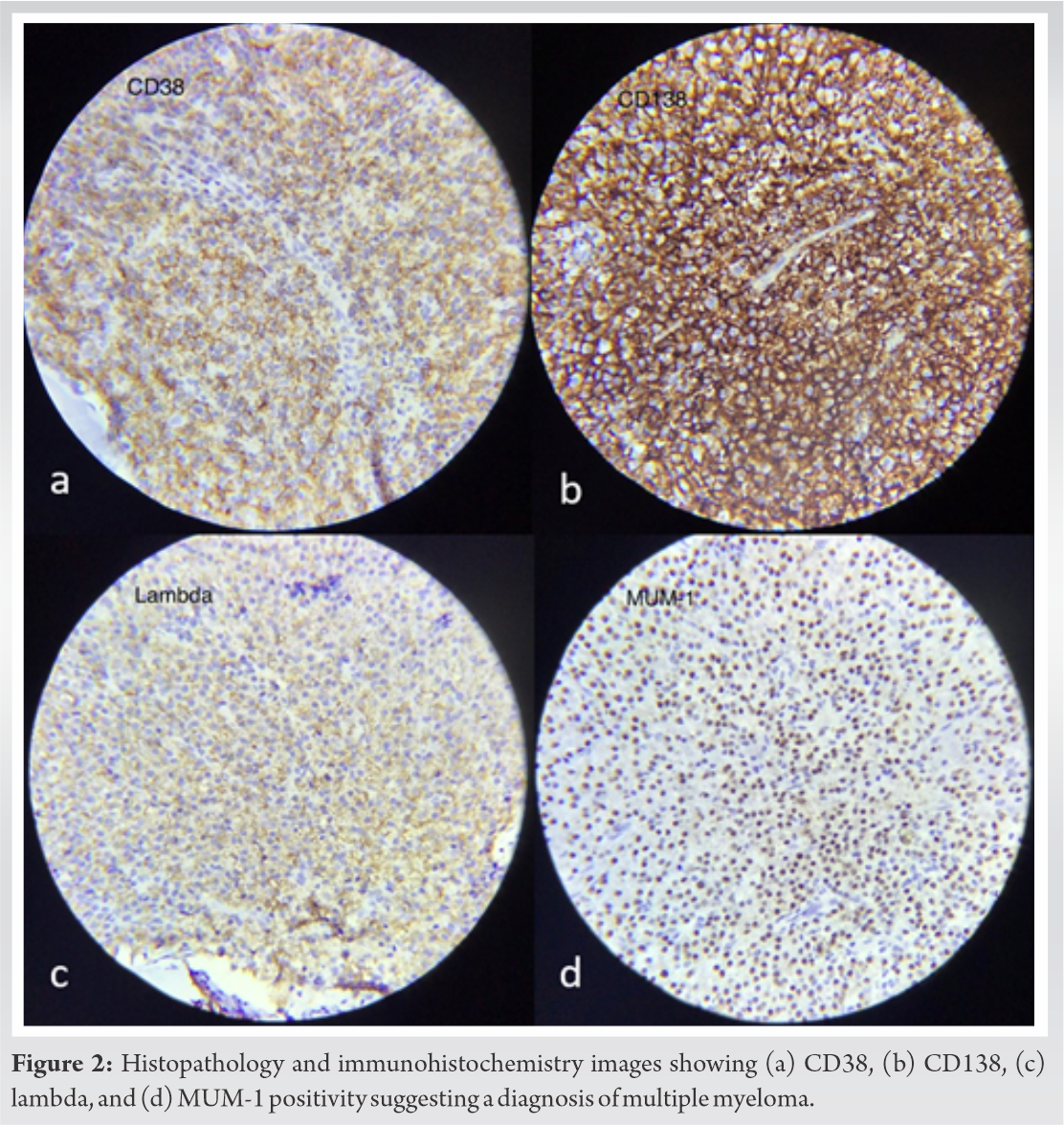
Multiple myeloma results from a neoplastic proliferation of plasma cells in the marrow which secretes monoclonal immunoglobulins [6]. This condition is usually associated with osteolytic skeletal lesions due to increased osteoclastic activity. The common symptoms in multiple myeloma include hypercalcemia, renal failure, anemia, and lytic bone lesions [7].
The histopathology findings of increased plasma cells and immunohistochemistry confirmed the presence of a plasma cell neoplasm in our patient. Osteosclerotic myeloma differs from multiple myeloma, with the affected patients being younger and the disease course is more indolent [5]. Almost 95% of cases of osteosclerotic myeloma show lambda chain restriction and neuropathy and rarely have significant bone pain arising out of bony destruction [8, 9]. In comparison, our patient was the elderly, presenting with diffuse low back pain without any neuropathy, which made clinical diagnosis of osteosclerotic myeloma difficult. Osteosclerotic myeloma often has a slow and chronic progression [10], as observed in our case, in which the symptoms gradually developed over a period of 4 months.
The patient radiographs showed a maximum density osteosclerotic lesion at L4; however, discrete sclerotic lesions were also seen in the right iliac bone, left femoral neck, and thoracic vertebrae which first raised our suspicion toward a possible osteosclerotic myeloma. The HPE and immunohistochemistry showed increased plasma cells which are positive for CD138, CD38, MUM-1, and lambda chains confirming the diagnosis of non-secretory myeloma. These findings are supported by literature reported osteosclerotic myeloma which frequently affects the thoracic, lumbar spine, and the axial skeleton. Osteosclerosis takes the form of fluffy, irregular, and spiculated areas of osseous proliferation that are characteristic of this condition [11].
Erythrocytosis and thrombocytosis are common, while hypercalcemia and renal insufficiency are rare in patients with osteosclerotic myeloma [10]. Osteosclerotic cases usually have a low ESR, almost normal hemoglobin concentration, low concentration of M-protein, and absence of Bence-Jones proteinuria which was noted in our patient [10].
Multiple myeloma is a part of the spectrum of the plasma cell disorders ranging from asymptomatic monoclonal gammopathy of unknown significance to POEMS syndrome. POEMS syndrome is a paraneoplastic syndrome which occurs in underlying plasma cell disorder which affects multiple organ systems. Although skeletal lesions in myeloma are usually osteolytic, in 80–90% of cases of POEMS syndrome, skeletal lesions are osteosclerotic [9]. In their study, Miralles et al. reported 95% of cases of POEMS with bone involvement of which 86% were osteosclerotic [12]. Osteosclerosis in POEMS is thought to be associated with high levels of serum VEGF [5]. Osteosclerotic myeloma is postulated to be due to invasion of the periosteum by the neoplastic plasma cells, leading to the production of new bone [13]. In our case, multifocal osteosclerotic lesions were observed without any other features of POEMS syndrome which makes it unique.
Osteosclerotic myeloma without the features of POEMS syndrome is an extremely rare entity, and only a few cases have been reported in literature till date [8]. To the best of our knowledge, osteosclerotic myeloma in a light chain myeloma without POEMS syndrome has not been reported previously in the literature.
References
- 1.Rajkumar SV. Multiple myeloma. Curr Probl Cancer 2009;33:7. [Google Scholar]
- 2.Hall FM, Gore SM. Osteosclerotic myeloma variants. Skeletal Radiol 1988;17:101-5. [Google Scholar]
- 3.Mulleman D, Gaxatte C, Guillerm G, Leroy X, Cotten A, Duquesnoy B, et al. Multiple myeloma presenting with widespread osteosclerotic lesions. Joint Bone Spine 2004;71:79-83. [Google Scholar]
- 4.Clark MS, Howe BM, Glazebrook KN, Mauermann ML, Broski SM. Osteolytic-variant POEMS syndrome: An uncommon presentation of “osteosclerotic” myeloma. Skeletal Radiol 2017;46:817-23. [Google Scholar]
- 5.Terao T, Matsue K. Osteosclerotic myeloma without features of POEMS syndrome. Int J Hematol 2019;110:517-8. [Google Scholar]
- 6.Palumbo A, Anderson K. Multiple myeloma. N Engl J Med 2011;364:1046-60. [Google Scholar]
- 7.Dispenzieri A, Kyle RA. Multiple myeloma: Clinical features and indications for therapy. Best Pract Res Clin Haematol 2005;18:553-68. [Google Scholar]
- 8.Lacy MQ, Gertz MA, Hanson CA, Inwards DJ, Kyle RA. Multiple myeloma associated with diffuse osteosclerotic bone lesions: A clinical entity distinct from osteosclerotic myeloma (POEMS syndrome). Am J Hematol 1997;56:288-93. [Google Scholar]
- 9.Dispenzieri A. POEMS syndrome: 2019 Update on diagnosis, risk‐stratification, and management. Am J Hematol 2019;94:812-27. [Google Scholar]
- 10.Reitan JB, Pape E, Fosså SD, Julsrud OJ, Slettnes ON, Solheim OP. Osteosclerotic myeloma with polyneuropathy. Acta Med Scand 2009;208:137-44. [Google Scholar]
- 11.Schey S. Osteosclerotic myeloma and ‘POEMS’ syndrome. Blood Rev 1996;10:75-80. [Google Scholar]
- 12.Miralles GD, O’Fallon JR, Talley NJ. Plasma-cell dyscrasia with polyneuropathy. The spectrum of POEMS syndrome. N Engl J Med 1992;327:1919-23. [Google Scholar]
- 13.Rodriguez AR. Osteosclerotic myeloma. JAMA 1976;236:1872-4. [Google Scholar]







