
Glenohumeral instability may be accurately graded even in obese or well-built individuals, in whom other tests may be challenging, using the mechanical advantage of a Class 3 lever through the shoulder lever test.
Dr. Viraj Gandbhir, Department of Orthopaedics B.Y.L. Nair Ch. Hospital, Dr. A. L. Nair Road, India. E-mail: drvirajg@gmail.com
Introduction:The classical shoulder tests for instability of the glenohumeral joint are the load and shift and drawer tests. Here, the humeral head is gripped between fingers and thumb to assess translation. This can be challenging to perform accurately in obese individuals and muscular athletes.
Technical Tip:The shoulder and upper arm is utilized as a Class 3 lever. By fixing the patient’s elbow (fulcrum) and applying translational force on the humerus (force), the instability at the glenohumeral joint (load) can be accurately judged. The mechanical advantage of a Class 3 lever is utilized to generate maximal displacement at the glenohumeral joint by applying minimal translational force at the humerus. The translation can be graded with the modified Hawkins scale.
Conclusion:The shoulder lever test obviates the need to grip the humeral head in obese and well-built individuals to accurately judge the translation at the glenohumeral joint, improving the clinical yield.
Keywords:Shoulder, shoulder instability, load and shift test, drawer test, athletes, anterior instability, posterior instability, obese, clinical test, class 3 fulcrum, glenohumeral instability, fulcrum.
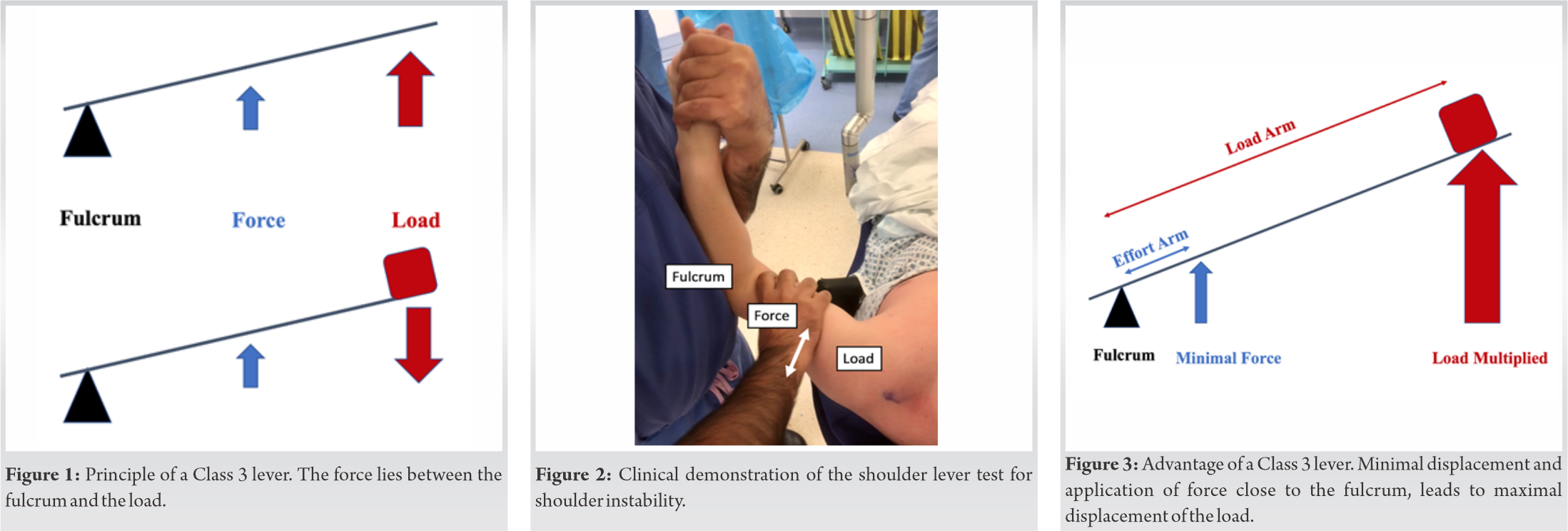
The glenohumeral joint is the most commonly dislocated major joint in the human body [1]. The dislocation episode is often considered to be an extreme end event with subluxation episodes more common and accounting for about 85% of the instability cases [2]. Rather than being two distinct and dichotomous scenarios, the glenohumeral instability often exists on a spectrum, ranging from subtle subluxations, in which the articular contact is lost only partially, to frank dislocations. Although the clinical diagnosis of instability may be obvious after an episode of dislocation, it becomes more challenging in patients with subtle instability. Accurate identification of instability and subsequent treatment has been shown to drastically decrease the rate of recurrent dislocations [3]. A survey of experienced senior shoulder surgeons in the United States revealed that the classical load and shift test remained one of the most commonly used clinical test for instability [4]. The classical load and shift test involve abduction and axial loading of the humeral head onto the glenohumeral joint followed by assessment of the humeral head translation by gripping it between the thumb posteriorly and the fingers anteriorly [5]. The patient may be in sitting or supine position [6]. This test has been shown to be both reliable and valid for diagnosing anterior and posterior shoulder instability, with good interobserver reliability [7, 8]. It is however challenging to perform in large muscular or obese individuals as one may not be able to satisfactorily grip the humeral head between the thumb and fingers. Without the ability to securely hold onto the humeral head, the load and shift test cannot measure translation and loses its value [2]. We describe a shoulder lever test; a test for glenohumeral instability, utilizing the leverage of the humerus as a Class 3 lever (Fig. 1), obviating the need to grip the humeral head.
The patient is appropriately exposed and placed in a beach chair position. The examiner stands on the side of the shoulder, grasping the patient’s hand whilst fixing the patient’s elbow between the examiner’s arm and trunk (Fulcrum). The shoulder is then placed in 30° of flexion and 90° of abduction. The examiner’s other hand holds the patient’s upper arm, to apply translation (Force). As the anterior or posterior forces are applied, translation of the humeral head relative to the glenoid is evaluated (Load) (Fig. 2). The translation is compared to the contralateral side and graded on the modified Hawkins scale (Table 1). The test can be performed in outpatient setting or in the operating theater under anesthesia.
Existing clinical tests for instability are challenging to perform reliably in large muscular individuals, such as Rugby players or obese individuals [9, 10]. The shoulder lever test utilizes the mechanical advantage of a Class 3 lever in the shoulder’s’ most vulnerable position.
In a Class 3 lever, the force lies between the fulcrum and the load. With the force applied, the load moves further than the force (Fig. 3). This property of a Class 3 lever is utilized in the shoulder lever test, where minimum effort, that is, translational force on the upper arm, leads to maximum translation at the glenohumeral joint which can be easily assessed. The mechanical advantage can be further increased by moving the force toward the fulcrum (translational force as close to the elbow joint as possible). Thus, humeral head translation and the instability can easily and accurately be judged in large and bulky individuals. Unlike the binary results of the apprehension test, jerk test, or relocation test, the shoulder lever test can also help grade the instability with the modified Hawkins scale (Table 1).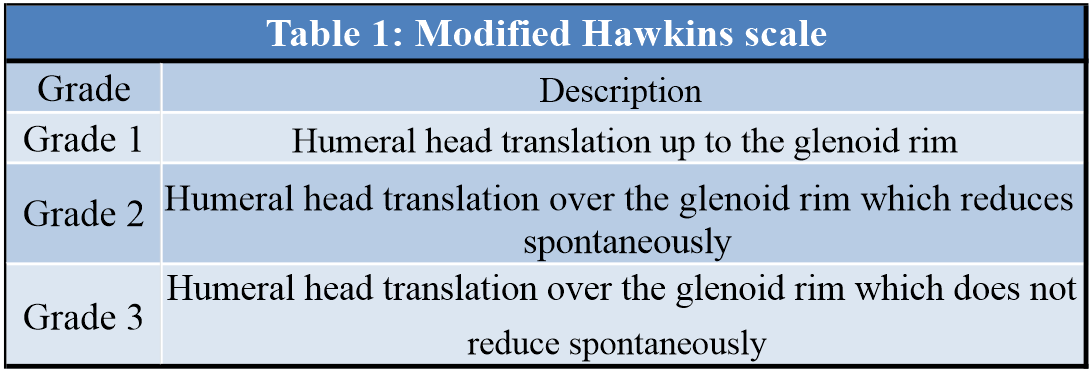
The glenohumeral joint is inherently unstable and relies on static and dynamic stabilizers to maintain congruity. The most important static stabilizer is the inferior glenohumeral ligament (IGHL), which is the primary restraint in 90o of abduction and external rotation [11]. Our test, by placing the shoulder in 90o of abduction, tests for the IGHL laxity, which can be encountered in roughly 90% of traumatic anterior shoulder dislocations [11].
The shoulder lever test improves the clinical yield by utilizing the leverage provided by the humerus in the position of vulnerability. This test is especially useful in detecting instability in muscular and obese patients, where grasping the humeral head with the load and shift test is challenging.
Glenohumeral instability may be accurately graded even in obese or well-built individuals, in whom other tests may be challenging, using the mechanical advantage of a Class 3 lever.
References
- 1.Cutts S, Prempeh M, Drew S. Anterior shoulder dislocation. Ann R Coll Surg Engl 2009;91:2-7. [Google Scholar]
- 2.DeFroda SF, Owens BD. Arthroscopic load-shift technique for intraoperative assessment of shoulder translation. Arthrosc Tech 2018;7:e211-4. [Google Scholar]
- 3.Lizzio VA, Meta F, Fidai M, Makhni EC. Clinical evaluation and physical exam findings in patients with anterior shoulder instability. Curr Rev Musculoskelet Med 2017;10:434-41. [Google Scholar]
- 4.Sciascia AD, Spigelman T, Ben KW, Uhl TL. Frequency of use of clinical shoulder examination tests by experienced shoulder surgeons. J Athl Train 2012;47:457-66. [Google Scholar]
- 5.Silliman JF, Hawkins RJ. Classification and physical diagnosis of instability of the shoulder. Clin Orthop Relat Res 1993;291:7-19. [Google Scholar]
- 6.Cotter EJ, Hannon CP, Christian D, Frank RM, Bach BR. Comprehensive examination of the athlete’s shoulder. Sports Health 2018;10:366-75. [Google Scholar]
- 7.Tzannes A, Paxinos A, Callanan M, Murrell GA. An assessment of the interexaminer reliability of tests for shoulder instability. J Shoulder Elb Surg 2004;13:18-23. [Google Scholar]
- 8.Morita W, Tasaki A. Intra-and inter-observer reproducibility of shoulder laxity tests: Comparison of the drawer, modified drawer and load and shift tests. J Orthop Sci Off J Japanese Orthop Assoc 2018;23:57-63. [Google Scholar]
- 9.Hippensteel KJ, Brophy R, Smith MV, Wright RW. Comprehensive review of provocative and instability physical examination tests of the shoulder. J Am Acad Orthop Surg 2019;27:395-404. [Google Scholar]
- 10.Silliman JF, Hawkins RJ. Current concepts and recent advances in the athlete’s shoulder. Clin Sports Med 1991;10:693-705. [Google Scholar]
- 11.Owens BD, Nelson BJ, Duffey ML, Mountcastle SB, Taylor DC, Cameron KL, et al. Pathoanatomy of first-time, traumatic, anterior glenohumeral subluxation events. J Bone Joint Surg Am 2010;92:1605-11. [Google Scholar]





