
Pediatric patients presenting with closed anterior elbow dislocation can be managed by closed reduction successfully with good functional outcome if neurovascular and other surrounding bony injuries are ruled out.
Dr. Divya Tomer, Department of Orthopaedics, BJ Government Medical College and Sassoon General Hospital, Pune, Maharashtra, India. E-mail: tomerdivya@gmail.com
Abstract
Introduction: Anterior transolecranon fracture dislocation of the elbow is rarely found in pediatric patients, with very few cases reported till now, and very less literature available on its management.
Case Report: We hereby present a rare case of trauma to the left elbow in a 9-year-old female child who sustained anterior transolecranon dislocation without neurovascular deficit. Such fracture dislocations are managed usually by surgical methods with or without osteosynthesis. However, we present a report of closed reduction of the condition with good clinical outcomes.
Conclusion: Closed reduction can be a safe method of treatment of anterior dislocation of the elbow if no neurovascular deficit is present. This case report aims to highlight this possible treatment method which in itself is unusual for this uncommon pediatric injury.
Keywords: Anterior dislocation, pediatric elbow dislocation, transolecranon dislocation.
Anterior transolecranon dislocation of the elbow is a rare injury in children, although not uncommon in adults [1,2,3,4]. The most common elbow dislocation in children is posterior, and is due to indirect forces transmitted on falling on an outstretched hand [1, 5,6 ]. On the contrary, anterior dislocation is due to direct trauma to the proximal ulna after a fall on the elbow in flexion. Isolated transolecranon as well as accompanying medial epicondyle of humerus and radial head fractures can occur, which require osteosynthesis [7]. Here, we describe a case of isolated transolecranon dislocation managed by closed reduction with good results.
A 9-year-old female came to the emergency room with a history of self-fall at home 2 h ago complaining of trauma to the left elbow. There was swelling over the elbow and the patient was not able to actively move the elbow due to pain. There was a palpable step deformity with anterior dislocation of the elbow, with tenderness over the olecranon. Distal pulses were well felt and all the nerves were normal on testing. Radiographs performed showed left anterior transolecranon fracture dislocation without radial head injury (Fig. 1, 2). The child was given analgesics and slab and after stabilization, an attempt of closed reduction was given under local anesthesia. The elbow could not be reduced. The child was subsequently posted under general anesthesia after a few hours and closed reduction was performed successfully by giving a backward thrust to the forearm with a hyperflexed elbow with counterforce applied over the distal arm (Fig. 3). Distal neurovascular status was rechecked and found normal and elbow stability was confirmed by continuous passive motion under fluoroscopy (Fig. 4, 5). The child was given a slab in 70° flexion and discharged on the next morning. An MRI was done which showed diffuse bone edema in the distal humerus and head of radius and olecranon, without any osseous separation. Moderate joint effusion was seen with a sprain of the annular ligament and medial and lateral collateral ligaments. The elbow was immobilized in a cast for 4 weeks, which was removed, and physiotherapy and elbow range of motion were given. The child showed full flexion and extension on 2 months of follow-up (Fig. 6, 7).
The child was given analgesics and slab and after stabilization, an attempt of closed reduction was given under local anesthesia. The elbow could not be reduced. The child was subsequently posted under general anesthesia after a few hours and closed reduction was performed successfully by giving a backward thrust to the forearm with a hyperflexed elbow with counterforce applied over the distal arm (Fig. 3). Distal neurovascular status was rechecked and found normal and elbow stability was confirmed by continuous passive motion under fluoroscopy (Fig. 4, 5). The child was given a slab in 70° flexion and discharged on the next morning. An MRI was done which showed diffuse bone edema in the distal humerus and head of radius and olecranon, without any osseous separation. Moderate joint effusion was seen with a sprain of the annular ligament and medial and lateral collateral ligaments. The elbow was immobilized in a cast for 4 weeks, which was removed, and physiotherapy and elbow range of motion were given. The child showed full flexion and extension on 2 months of follow-up (Fig. 6, 7).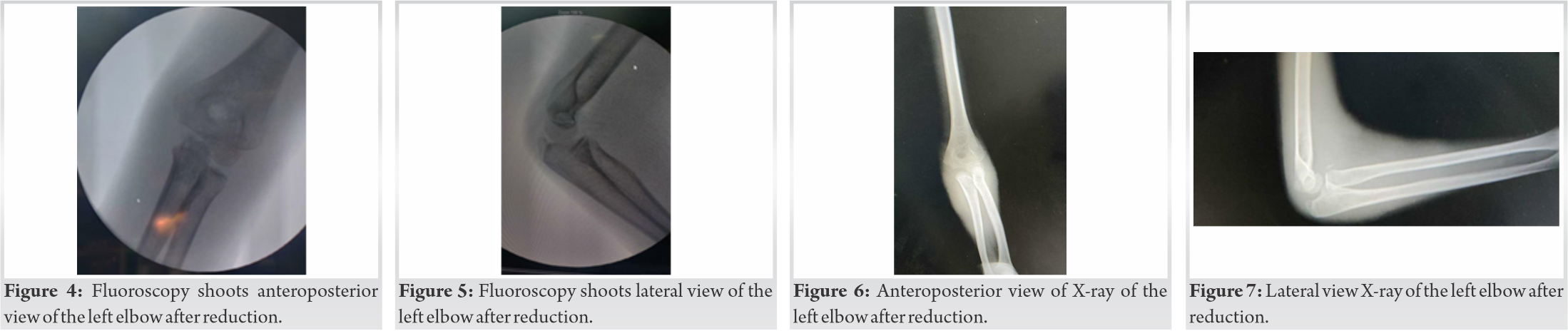
Anterior transolecranon fracture dislocation is rare, and its management has been described by many by open reduction [1,3,4,7]. Closed reduction maneuvers may fail if an annular ligament is completely torn with anterior dislocation of olecranon and radial head [1,8]. Buttonholing of the radial head, in that case, may occur through the anterior elbow joint capsule, which may have to be released under vision, preferably via a lateral surgical approach [9]. The reduction can then be verified under fluoroscopy and stability can be checked. If the joint is found to be stable, internal fixation may not be required. If the joint is found unstable or if found associated with other fractures, an internal fixation device may be useful, like tension band wiring or plating [4,10,11]. Associated medial epicondyle fractures may need screw fixation [7]. A slab is given for 4 weeks and good functional and radiological recovery can be expected in most cases [1]. Anterior dislocation is often having fractures around the elbow, with some cases having neurovascular injury [12,13]. Brachial artery can be thrombosed or torn and should be explored early if the distal flow is found to be absent [12]. These fracture dislocations have been classified into 4 types by aversano [14] and Tiemdjo [15]. However, they proposed employing open reduction and internal fixation for all types which may be unnecessary, as demonstrated in our case. Aggressive physiotherapy is advised to avoid post-immobilization stiffness and lack of normal extension.
Anterior transolecranon dislocation is a rare injury of the elbow. It needs to be reduced on an emergency basis and closed reduction can be attempted. However, open reduction may be required due to soft-tissue block or neurovascular or accompanying surrounding bone fractures.
It is important to note that if the case is isolated fracture dislocation without neurovascular or other bony injuries, a conservative management can be offered to the patients. Closed reduction of anterior elbow dislocation is safe, preferably performed under anesthesia.
References
- 1.Bouaziz W, Guidara AR, Trabelsi A, Bardaa T, Hammami M, Ellouz Z, et al. Anterior transolecranon dislocation of the elbow in a child: A case report and review of literature. World J Orthop 2018;9:100-4. [Google Scholar | PubMed]
- 2.Ring D, Jupiter JB, Sanders RW, Mast J, Simpson NS. Transolecranon fracture-dislocation of the elbow. J Orthop Trauma 1997;11:545-50. [Google Scholar | PubMed]
- 3.Arain AR, Haddad S, Anderson M, Murtaza H, Rosenbaum A. Isolated pediatric transolecranon fracture-dislocation of the elbow managed nonoperatively: A case report and review of literature. Clin Case Rep 2019;7:1435-8. [Google Scholar | PubMed]
- 4.Guitton TG, Albers RG, Ring D. Anterior olecranon fracture-dislocations of the elbow in children. A report of four cases. J Bone Joint Surg Am 2009;91:1487-90. [Google Scholar | PubMed]
- 5.Kaziz H, Naouar N, Osman W, Ayeche M. Outcomes of paediatric elbow dislocations. Malays Orthop J 2016;10:44-9. [Google Scholar | PubMed]
- 6.Altuntas AO, Balakumar J, Howells RJ, Graham HK. Posterior divergent dislocation of the elbow in children and adolescents: A report of three cases and review of the literature. J Pediatr Orthop 2005;25:317-21. [Google Scholar | PubMed]
- 7.Butler MA, Martus JE, Schoenecker JG. Pediatric variants of the transolecranon fracture dislocation: Recognition and tension band fixation: Report of 3 cases. J Hand Surg Am 2012;37:999-1002. [Google Scholar | PubMed]
- 8.Takase K, Mizuochi J. Irreducible dislocation of the radial head with undisplaced olecranon fracture in a child: A case report. J Pediatr Orthop B 2011;20:345-8. [Google Scholar | PubMed]
- 9.Patel NN, Bruce RW. Transcapsular buttonholing of the proximal ulna as a cause for irreducible pediatric anterior elbow dislocation. Case Rep Orthop 2018;2018:8986230. [Google Scholar | PubMed]
- 10.Yang Z, Feng C, Bian Z, Lu M, Zhou D. Trans-olecranon fracture-dislocation of the elbow in children. Int Orthop 2021;45:2025-31. [Google Scholar | PubMed]
- 11.Yamaura K, Inui A, Mifune Y, Nishimoto H, Kataoka T, Kurosawa T, et al. Anterior transolecranon fracture dislocation with an associated avulsion fracture of coronoid process of ulna in a child: A case report. JSES Int 2021;5:9-12. [Google Scholar | PubMed]
- 12.Kailash S, Shanmuganathan S. Anterior dislocation of elbow with neurovascular injury: A rare case report. J Orthop Case Rep 2017;7:91-4. [Google Scholar | PubMed]
- 13.Ashar NA, Liew SK, Azmi NS, Yeak RD, Lingam R, Chen RA. Anterior elbow fracture dislocation with ulnar nerve palsy in a six-year-old child. Pediatr Traum Orthop Reconstr Surg 2020;8:207-12. [Google Scholar | PubMed]
- 14.Aversano F, Kepler CK, Blanco JS, Green DW. Rare cause of block to reduction after radial head dislocation in children. J Orthop Trauma 2011;25:e38-41. [Google Scholar | PubMed]
- 15.Tiemdjo H, Kinkpe C, Coulibaly NF, Sane A, Ndiaye A, Seye SI. Anterior transolecranon fracture-dislocations of the elbow in children: A case report and review of the literature. Arch Pediatr 2015;22:737-40. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2018 Enchondroma with Osteopoikilosis Coexisting Together –A Rare Clinical and Radiological Case Report
January 10, 2018 Enchondroma with Osteopoikilosis Coexisting Together –A Rare Clinical and Radiological Case Report January 19, 2013 Fat Embolism Syndrome in Fracture Tibia Treated By Unreamed Interlocking Nail
January 19, 2013 Fat Embolism Syndrome in Fracture Tibia Treated By Unreamed Interlocking Nail May 9, 2017 Guest Editorial – Minimally Invasive Joint Replacement Surgery: Where Are We Now?
May 9, 2017 Guest Editorial – Minimally Invasive Joint Replacement Surgery: Where Are We Now? January 10, 2018 The Challenges of the Femoral Bone Loss in the Management of the Floating Knee IIB According Fraser: A Case Report
January 10, 2018 The Challenges of the Femoral Bone Loss in the Management of the Floating Knee IIB According Fraser: A Case Report