The in vivo demonstration of the principle of dynamic compression and its importance in the healing of a patellar fracture treated by modified tension band wiring.
Dr. Gautam Rava, Department of Orthopaedics, GNRC Hospital, Dispur - 781 005, Assam, India. E-mail: gautamrava@outlook.com
IntroductionModified tension band wiring (MTBW) using two cannulated cancellous screws which also achieve a horizontal figure of eight patterns of tension band is established as a superior fixation to using Kirschner wires for type 34-C1 fracture of the patella. We are describing a case where this method was used for failed MTBW using two Kirschner wires where an impending failure in the early post-operative period proceeded to complete bony union without any implant failure or functional deficit following a period of conservative management.
Case PresentationWe are describing a 67-year-old man with type 34-C1 fracture of patella treated by MTBW using Kirschner wires and a stainless steel (SS) wire, with fixation failure after around 6 weeks, which was revised by MTBW using two vertically placed cannulated partially threaded cancellous screws and SS wire as a tension band. In the early post-operative period, a routine X-ray of the operated part showed fracture fragment separation with a slight sack in the tension band wire without any signs of implant failure. To our surprise, the fracture proceeded to complete bony union while continuing gradually increased active knee range of motion exercises.
ConclusionThis case report presents how an impending failure proceeded to complete fracture healing because of dynamic compression of the fracture provided by the tension band construct.
KeywordsFixation failure, modified tension band wiring, dynamic compression.
Modified tension band wiring (MTBW) of acute transverse patellar fracture is an acceptable and reproducible technique originally described by the Association for the Study of Internal Fixation (AO) group [1], the success of this construct is because of its ability to convert the shear or distraction force over a patellar fracture, due to its anatomic location, to effective compressive force when there is knee flexion [2]. This is an example of dynamic compression achieved at the fracture site [3]. MTBW using two vertical cannulated cancellous screws (CCSs) and tension band wire (TBW) through it, which also achieves a horizontal figure of eight configurations, has been found to have a higher load to failure [4] and hence provide immediate stability which allows early mobilization. Our case presentation is about how an impending failure of fixation by this technique, probably due to the early start of active range of motion (AROM) exercise leading to dynamic fracture compression along with good stability provided by the implant construct finally proceeded to complete fracture healing in a failed MTBW. To the best of our knowledge, this unusual course in the healing process of a patellar fixation has not been described in the literature before.
A 67-year-old gentleman, non-hypertensive, and non-diabetic presented to our emergency department with an alleged history of slip and fall while walking at home followed by injury to the left knee joint. On examination, the knee was swollen and slightly warm with fluctuation probably due to hemarthrosis, without any neurovascular deficit. The rest of the other systemic examinations were unremarkable. A roentgenogram was obtained in both AP and lateral views (Fig. 1) showing transverse fracture of patella (AO type 34-C1). After taking informed consent and relevant pre-operative investigation, the patient was taken for open reduction and internal fixation by K-wires and MTBW (Fig. 2) using a longitudinal midline incision under regional (spinal) anesthesia. Two 2 mm Kirschner wires and 18 Gauge (1.02 mm) stainless steel (SS) wire as tension band were used. Medial and lateral retinaculum inspected and repair performed meticulously. Wound closure done in layers without drain. Postoperatively, a rigid knee brace was applied. Immediate rehabilitation protocol followed include static quadriceps exercises, active straight leg raising exercises (SLR),and gentle knee AROM exercises 0–45° immediately. A partial weight-bearing 3-point gait was allowed using bilateral axillary crutches. The hospital stay went uneventfully and the patient was discharged 2 days after the operation. A routine check-up was performed after 2 weeks for wound inspection, which was unremarkable. Knee AROM was also increased to 0–90°.
After around 6 weeks, the patient presented to us with a history of mild pain in the operated area, more at night. There was no history of any falls or injuries. On inspection, the surgical scar was well healed, without any signs of inflammation, on palpation tenderness was present, the temperature was normal, and a palpable gap of around 1 cm was noted at the fracture site. Immediately, an X-ray was obtained which revealed distraction at the fracture site due to pulling out of the medial sided K-wire, leading to loosening of the construct (Fig. 3). After counseling the patient regarding fixation failure, and after obtaining informed consent, planning was done for revision fixation of the fracture. Pre-operative investigations and pre-anesthetic clearance were obtained as routine protocol, then the patient was taken for the operation. After sterile draping of the part, the previous incision was used and 4.0 mm CCS and SS wire (18 Gauge) was used to fix the fracture under spinal anesthesia. Wound closure was done without drain and an absorbable stitch for skin was applied.
Immediate post-operative X-ray showed a very satisfactory reduction (Fig. 4). The patient was discharged uneventfully from the hospital after the 2nd day and the same rehabilitation protocol was started as used previously after the first operation.
After around 3 weeks, the patient presented to us again with a history of sudden slip without any fall and pain and mild swelling over the operated area. On examination, the knee was mildly swollen, the surgical wound completely healed, the temperature normal, and tenderness over the fracture site. Immediately, an X-ray was obtained (Fig. 5) which showed mildly distracted fracture without any signs of implant failure. This time we were in a dilemma whether to treat it or just wait and watch.
However, due to the patient’s request, a second opinion from a senior Orthopedic surgeon was sought, who advised just to continue with conservative management and physiotherapy. The patient agreed to that and physiotherapy was continued, with gradually increasing AROM exercises 0–140° in a few weeks.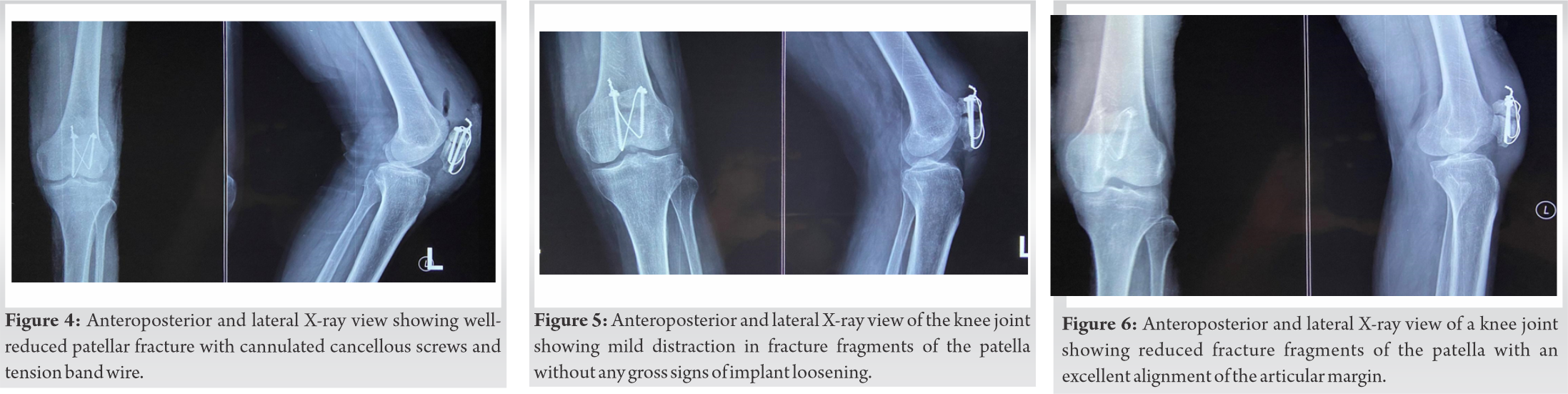
The patient was routinely followed up after a month, and to our surprise, X-ray showed a very satisfactorily reduced fracture (Fig. 6). At this time, active SLR also improved and the patient was allowed to walk with a walking stick only.
Subsequently, the patient appeared again after a year for a check-up, during which time, he gradually improved the function of the knee joint. At this time, X-ray showed a completely healed fracture (Fig. 7).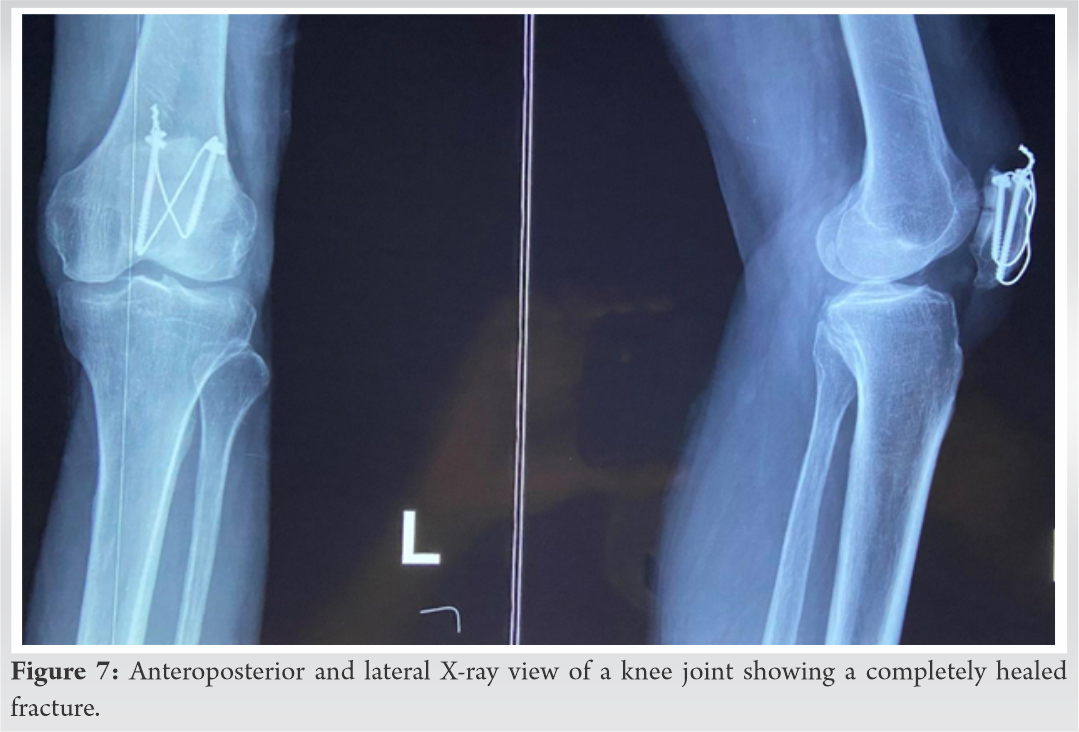
Transverse fractures of the patella are known to occur after a direct blow over the knee joint or by an indirect method of fall on the feet and eccentric contraction of the quadriceps muscle [5]. In our patient, it was the second, that is, indirect mechanism. Patellar fractures constitute 1% of all skeletal injuries and around 50–80% of patellar fractures are transverse [6].
Various fixation methods for a transverse fracture of the patella have been described using non-metallic implants [6], newer implants like anterior fixed-angle plate [7], and fragment fixation system [8].
MTBW is the most common method of fixation of a displaced transverse fracture of the patella. Compression at the fracture site is obtained by an anterior wire/cable passed behind the K-wires superior and inferior to the patella. Both figure 0 and figure of 8 tension band construct have been described to achieve compression. The main component achieving stability by this technique is the tension band, that is, wire/cable, while the K-wires act like a tough structure supporting the tension band while tightening to achieve fracture compression [9]. Some other important points highlighted by Baran et al. in their study of anatomical and biomechanical evaluation of tension band wiring [9] are – (i) horizontally oriented figure of 8 achieves more stability than vertically oriented, (ii) flexibility of the tension band material SS wire in this case and wire twisting technique are important for good force distribution, (iii) the initial compression while applying the tension band if leading to bending of wires also leads to displacement, (iv) for increasing the stability of this construct, the tension force should be placed as close to the bone as possible, and (v) placing two twists in adjacent corners can increase compression by 18% than a single twist.
A study comparing various patellar fixation devices has found that in general, 25–42% of patients treated by this method suffer from some form of complications such as implant failure, K-wire migration, and hardware prominence requiring removal [6].
In our case, we have passed the K-wires through the quadriceps tendon, the tension band behind the K-wires through the quadriceps tendon, and inferiorly through the patellar tendon by making longitudinal stab incisions over the tendons. In the proximal part of our construct, K-wires are bent 180° after the tension band is tightened and pushed inferiorly by a longitudinal split in the quadriceps tendon. If we analyze (Fig. 3), there is a pull out of the medial sided K-wire, which subsequently led to the loosening of the TBW construct, leading to fracture separation.
MTBW using two parallel CCSs, Berg EE in his 10 patients found this method to have good to excellent outcomes with no loss of reduction or implant failure [10]. He also concluded that the construct was low profile with lesser degrees of implant irritation to local soft-tissue structures. He also used this construct to salvage three cases in which tension band wiring failed to maintain an anatomic reduction in osteoporotic bone and also found this construct compatible with the use of early restricted motion. MTBW using cannulated screw and titanium cable has shown superior performance in terms of improved fracture reduction, reduced healing time, and better Iowa score, compared with the modified tension band group in a study by Tian et al. [4].
We believe in our case we achieved a satisfactory reduction by the MTBW using CCS construct as evident on the immediate post-operative X-ray (Fig. 4). However, we have observed that there was a slack in the tension band probably due to its rigidity and slight protrusion of the tip of the cancellous screw from the distal end of the patella, which finally led to the loosening of our construct and impending failure. However, as the construct was stable and knee bending was gradually increased, thereby leading to gradual compression and bony union at the fracture site finally as evident in (Fig. 6, 7), respectively.
Our case gives us an opportunity to demonstrate the concept of dynamic compression at fracture using the principle of tension band wiring in vivo, from slight distraction to compression of the fracture on AROM exercises of the knee joint. And after this case and following the evidence from the literature, we recommend MTBW with CCSs in the revision setting. The advantages which we believe are as follows –
(i) The entire construct is through the metallic implant, thereby reducing its dependence on the bone quality and soft-tissue structure
(ii) The tension band can be directly seated closer to the bone through the cancellous screws than just passing behind the K-wires, thereby increasing the stability of the construct
(iii) While passing the tension band through cannulated screws, we achieve a horizontal figure of 8 configurations, thereby achieving more stability [10].
The main disadvantage is that there may be only a limited amount of bone to accommodate two cannulated screws and if a hardware failure occurs, revision may become difficult.
Finally, for early fracture consolidation, equally important is the AROM exercises, as the construct converts the distracting forces to dynamic compression at the fracture site.
The importance of dynamic compression in the healing of a patellar fracture treated by the principle of tension band wiring, using the most appropriate construct which allows immediate active movement of the knee joint.
References
- 1.Muller ME, Allgower M, Schneider R, Willengger H. Manual of Internal Fixation: Techniques Recommended by AO-ASIF Group. 3rd ed. Berlin, Heidelberg: Springer-Verlag; 1991. p. 226. [Google Scholar]
- 2.Yang TY, Huang TW, Chuang PY, Huang KC. Treatment of displaced transverse fractures of the patella: Modified tension band wiring technique with or without augmented circumferential cerclage wire fixation. BMC Musculoskelet Disord 2018;19:167. [Google Scholar]
- 3.Schatzker J. In: Schatzker J, Tile M, editors. The Rationale of Operative Fracture Care. 3rd ed. Berlin, Heidelberg: Springer-Verlag; 2005. p. 443. [Google Scholar]
- 4.Tian Y, Zhou F, Ji H, Zhang Z, Guo Y. Cannulated screw and cable are superior to modified tension band in the treatment of transverse patella fractures. Clin Orthop Relat Res 2011;469:3429-35. [Google Scholar]
- 5.Gwinner C, Märdian S, Schwabe P, Schaser KD, Krapohl BD, Jung TM. Current concepts review: Fractures of the patella. GMS Interdiscip Plast Reconstr Surg DGPW 2016;5:Doc01. [Google Scholar]
- 6.Heusinkveld MH, Den Hamer A, Traa WA, Oomen PJ, Maffulli N. Treatment of transverse patellar fractures: A comparison between metallic and non-metallic implants. Br Med Bull 2013;107:69-85. [Google Scholar]
- 7.Thelen S, Schneppendahl J, Jopen E, Eichler C, Koebke J, Schönau E, et al. Biomechanical cadaver testing of a fixed-angle plate in comparison to tension wiring and screw fixation in transverse patella fractures. Injury 2012;43:1290-5. [Google Scholar]
- 8.Dargel J, Gick S, Mader K, Koebke J, Pennig D. Biomechanical comparison of tension band- and interfragmentary screw fixation with a new implant in transverse patella fractures. Injury 2010;41:156-60. [Google Scholar]
- 9.Baran O, Manisali M, Cecen B. Anatomical and biomechanical evaluation of the tension band technique in patellar fractures. Int Orthop 2009;33:1113-7. [Google Scholar]
- 10.Berg EE. Open reduction internal fixation of displaced transverse patella fractures with figure-eight wiring through parallel cannulated compression screws. J Orthop Trauma 1997;11:573-6. [Google Scholar]