
Importance of appropriate counseling of patients as well as the next of kin regarding follow up visits and procedures, keeping a high index of suspicion for infection in patients with retained cement and/ or implants, appropriate and timely management of any complications.
Dr. Gaurav B Mate, Department of Orthopaedics, B. J. Government Medical College, Pune, Maharashtra, India. E-mail: Gaurav.b.mate@gmail.com
Introduction: Chronic osteomyelitis is the bane of orthopedics. Along with being difficult to treat for surgeons, it also impacts the patient’s life immensely, severely restricting their life in all the aspects. Treatment with antibiotic coated cement spacers, which are removed after a duration of 6–8 weeks for the definitive surgery, is a frequently done procedure in conjunction with an adequate debridement of the necrotic tissues and prolonged IV antibiotics. We report a case of acute osteomyelitis superimposed on the chronic osteomyelitis of the left proximal humerus.
Case Presentation: An immunocompetent and otherwise healthy 14-year old Indian male who was operated 1 year ago for chronic osteomyelitis presented to us with an acute tense swelling, unbearable pain, and toxemia, with a cement spacer and multiple cement beads in situ. With regards to his initial injury, he had history of fall from height with a puncture wound, possible humerus fracture, treatment by local healers as well as surgical procedures in an outside facility with debridement and placement of cements spacer and beads. On presentation to our facility, removal of retained cement plus debridement was carried out, and after serial surgeries, the defect was successfully treated with the use of antibiotic loaded absorbable calcium sulfate.
Conclusion: A basic knowledge about the ideal practices for taking treatment is still inadequate in many population groups within India . It is important to spread awareness of proper healthcare seeking practices among people so that the disability associated time and loss of activity related to injury is significantly reduced. Furthermore, calcium sulfate can be an effective option for treatment of bone defects associated with chronic osteomyelitis.
Keywords: Chronic osteomyelitis, humerus shaft, antibiotic-loaded calcium sulfate.
Complete and easy access to modern medical facilities are limited in many rural areas in India [1]. A simple fracture can land up in osteomyelitis due to inadequate knowledge and treatment by quacks. Along with being difficult to treat for surgeons, osteomyelitis also impacts the patient’s life immensely, severely restricting their life in all aspects [2]. Through this case report, we want to emphasize that how the locally prevalent customs and lack of awareness regarding various orthopedic conditions can lead to dire consequences in ill-informed patients. The effectiveness of commercially available bone graft substitute as an option for bone defects is also emphasized through this study. While osteomyelitis requires a rigorous and long-term treatment, it inadvertently requires removal of long segments of bone [3]. The first necessary step of aggressive debridement of the local area leads to a defect and loss of structural support requiring further surgeries. Many options are available for filling the defect [4]. However, data on reconstruction of a humeral shaft defect by absorbable cement substitutes are poorly available. In this report, we aim to report our experience with one such case of an adolescent male with chronic osteomyelitis of humerus shaft caused due to lack of proper knowledge and facilities, and its treatment with bioabsorbable cement substitutes. We present a case of chronic post-traumatic osteomyelitis treated 1 year ago in outside facility, where antibiotic impregnated bone cement block and multiple bone cement beads were kept in situ after radical surgical debridement. Broad-spectrum antibiotics were administered. The patient never went for any follow-up visits and came directly to our hospital with clinical features of acute swelling, unbearable pain and toxemia.
A 14-year-old boy presented to us with an initial history of fall from height, puncture wound and deformity of the left upper arm. He was taken to local healers who used some sort of wooden splint for the deformity. After approximately 1 month’s time, the patient started having complains of recurring fever and discharge from old wound site with extrusion of small bits of bone. He was taken to a hospital for the same complaints, where after a thorough debridement of proximal humerus, antibiotic impregnated bone cement block and multiple beads were kept in situ. His second surgery for bone cement removal and definitive procedure was scheduled after 6 weeks. Due to lack of proper understanding regarding the condition and failure to recognize the need of second definitive procedure after the surgery, parents never took the patient back to that hospital. Child was asymptomatic for about a year when he started developing intermittent fever that was relieved by anti-pyretics and tepid-sponging. Over a period of 15 days, the patient developed gradually progressive swelling of the right arm which was caused discomfort in his day–to-day activities. Ultimately, when the patient presented to us at Government Medical College and Hospital, Aurangabad, he had excruciating pain, high-grade fever, and a large tense swelling of the left proximal arm with complete restriction of movement at shoulder joint. The rest of the distal joint functions were normal. No neurovascular deficit was observed. Laboratory studies revealed total leukocyte count of >20,000 cells/mm3 (hyper-leukocytosis) with 77% neutrophils. His hemoglobin levels were low and erythrocyte sedimentation rate (ESR) and C-reactive protein levels were quite high. His liver and renal function tests were within normal limits. X-ray of the left humerus was done which revealed a massive soft-tissue swelling, a large cement bone-block, and multiple bone cement beads. The proximal segment showed patchy sclerotic and lytic patches with areas of resorbed deformed head (Fig. 1). The patient was taken up for emergency incision and drainage procedure. 1.2 L of purulent greenish fluid was drained out. Fluid was sent for culture sensitivity. Drainage was followed by a thorough debridement and serial wash with removal of all cement particles. The humeral head was deemed viable and thoroughly debrided until paprika sign was positive. After preliminary fixation with intramedullary Rush nail (3.5 mm), wound was kept open and packed adequately (Fig. 2). No post-operative neurovascular deficit was observed. Patient’s general condition improved, pain and discomfort were greatly relieved and at post-operative day 3, leukocyte count dropped to 12,000.
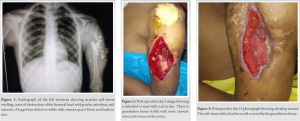
Daily dressing and local debridement of the open wound were done for 2 weeks under mild sedation and analgesia. The patient was started on intravenous Ceftriaxone 1gm twice a day immediately postoperatively, awaiting culture reports. Pus culture came positive for Pseudomonas aeruginosa sensitive to Piperacillin-Tazobactam, Vancomycin, Meropenem, and Ciprofloxacin. Parenteral treatment with Piperacillin-Tazobactam (Beta-Lactam) 4.5 g 8 hourly and Amikacin (Aminoglycoside) 500 mg 12 hourly combination was continued for 14 days. After the intravenous therapy, the patient was started on oral Ciprofloxacin 500 mg BD regimen for another 6 weeks. As the wound condition improved, counts dropped further to 6000, ESR normalized (Fig. 3). Throughout the postoperative period, the patient was started on grip strengthening exercises and passive elbow joint range of motion exercises as tolerated. At 6 weeks, when there was no radiological, clinical, and laboratory sign of active infection, the patient was taken for 2nd surgery where, through the previous wound tract, bioabsorbable bone cement substitute antibiotic carrier made of calcium sulfate (STIMULAN, Biocomposites, USA) mixed with Vancomycin and Tobramycin was used in conjunction with cancellous bone graft from iliac crest. Bone edges were refreshed after removing the previously placed rush pin. A thorough intramedullary serial wash was given. A new rush nail (4.5 mm) was introduced in proximal to distal direction. The calcium sulfate beads were prepared after mixing with the antibiotics. Beads were placed at the site of bone gap along with cancellous iliac crest bone graft chips along the nail. Adequate closure was done as much as possible as patient and relatives refused to undergo additional soft-tissue flap surgery. The arm was placed in a splint post operatively. The patient was started on hand and grip strengthening exercises and passive elbow range of motion as pain permitted immediately the next day. As the patient’s wound conditions improved, shoulder passive exercises were started after around 7 days. Grip strengthening exercises were continued and taught to the patient. The patient was gradually started on active shoulder motion from 12 weeks onward. The passive and active abduction was 0–45°, adduction was 0–10°, forward flexion was 0–90°, extension was from 0 to 5°, and internal and external rotation was about 5° at last follow-up (32 weeks). The patient was able to have full range in elbow and rest of the joints with some restriction to overhead activities.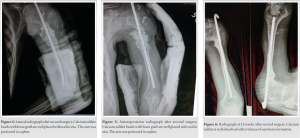
Post-operative X-ray showed well-placed beads along the length of nail in the defect (Fig. 4, 5). A follow-up radiograph at 12 weeks postoperatively showed complete absorption of the calcium sulfate beads and new bone formation along the site of defect (Fig. 6). The nail was removed after 20 weeks and at 32 weeks that the bone showed excellent healing (Fig. 7).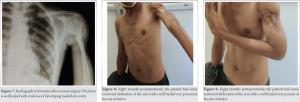
Debridement and reconstruction with complete clearance of osteomyelitis are quite a challenge, especially in sites where there is a lack of soft-tissue coverage. In this case, there was a defect of almost 6 cm in size. Various techniques have been described – the Papineau technique, the vascularized fibular transplant, the Ilizarov intercalary bone transport, and the IMT [5, 6]. Due to technical constraints, we opted for a bone cement substitute with cancellous autografts. The advantages of using synthetic bone substitutes are many besides overcoming the limitations of bone grafting [7, 8, 9]. The one disadvantage is that calcium sulfate is not able to provide structural support which was overcome by additional internal fixation with a nail [10]. The average time for resorption was around 14 weeks, and further, bone incorporation occurred in 8 months’ time. There was no incidence of repeat discharge/ wound healing problems at the site. Although calcium sulfate is prone to extrusion in lack of proper soft-tissue cover, we did not face such complications and the wound healed adequately. The patient had painless restricted mobility at the shoulder at 12 months, but it was well accepted by him and his relatives (Fig. 8, 9). The patient did not come for further follow-up.
This case is an important pointer about the lack of adequate knowledge in the general population regarding adequate care and access to proper healthcare. It provides an interesting view of how chronic osteomyelitis can have a varied presentation and the role of bone graft substitutes, especially antibiotic loaded calcium sulfate for its successful treatment. Additionally, it demonstrates its ability to successfully heal large bone defects (>5 cm). It can be a good option where there are cultural, technical, and logistical constraints, although cost may be a limiting factor. We need to revisit and reboot the already lacking knowledge, attitudes, and practices of rural Indian population with regard to orthopedic cases.
In today’s level of globalization and advances in the field of medicine, many of those who are on the downside of advantage, are still unaware of available health-care resources. When these people fall ill there is a loss of the healthy and working force for the country. A country’s wealth ultimately lies in the health of its people, therefore, until and unless a basic level of knowledge regarding minimal health-care options and the awareness regarding the importance of follow-up visits permeates to the grass-root levels of the population, these conditions will continue to be a cause of significant morbidity and mortality for these population groups . Furthermore, each case teaches some new techniques in the field of medicine, as this case demonstrates. When used diligently, calcium sulfate can be an ideal option to treat chronic osteomyelitis associated bone defects.
References
- 1.Barik D, Thorat A. Issues of unequal access to public health in India. Front Public Health 2015;3:245. [Google Scholar]
- 2.Tice AD, Hoaglund PA, Shoultz DA. Risk factors and treatment outcomes in osteomyelitis. J Antimicrob Chemother 2003;51:1261-8. [Google Scholar]
- 3.Hofstee MI, Muthukrishnan G, Atkins GJ, Riool M, Thompson K, Morgenstern M, et al. Current concepts of osteomyelitis: From pathologic mechanisms to advanced research methods. Am J Pathol 2020;190:1151-63. [Google Scholar]
- 4.Bezstarosti H, Metsemakers WJ, van Lieshout EM, Voskamp LW, Kortram K, McNally MA, et al. Management of critical-sized bone defects in the treatment of fracture-related infection: A systematic review and pooled analysis. Arch Orthop Trauma Surg 2021;141:1215-30. [Google Scholar]
- 5.Dinh P, Hutchinson BK, Zalavras C, Stevanovic MV. Reconstruction of osteomyelitis defects. Semin Plast Surg 2009;23:108-18. [Google Scholar]
- 6.Kerfant N, Valenti P, Kilinc AS, Falcone MO. Free vascularised fibular graft in multi-operated patients for an aseptic non-union of the humerus with segmental defect: Surgical technique and results. Orthop Traumatol Surg Res 2012;98:603-7. [Google Scholar]
- 7.Finkemeier CG. Bone-grafting and bone-graft substitutes. J Bone Joint Surg Am 2002;84:454-64. [Google Scholar]
- 8.Gazdag AR, Lane JM, Glaser D, Forster RA. Alternatives to autogenous bone graft: Efficacy and indications. J Am Acad Orthop Surg 1995;3:1-8. [Google Scholar]
- 9.Greenwald AS, Boden SD, Goldberg VM, Khan Y, Laurencin CT, Rosier RN, et al. Bone-graft substitutes: Facts, fictions, and applications. J Bone Joint Surg Am 2001;83:98-103. [Google Scholar]
- 10.Kumar CY, KB N, Menon J, Patro DK, Banerji BH. Calcium sulfate as bone graft substitute in the treatment of osseous bone defects, a prospective study. J Clin Diagn Res 2013;7:2926-8. [Google Scholar]






