
Cavernous medullary hemangiomas diagnosed in the appendicular skeleton can be successfully managed by thorough curettage and bone graft impaction, with supplementary stabilization using a hydroxyapatite block or PEEK plate.
Dr. Amyn M Rajani, Department of Orthopaedics, OAKS Clinic, 707 Panchshil Plaza, N S Patkar Marg, Opp. Ghanasingh Fine Jewels, Next to Dharam Palace, Gamdevi, Mumbai, Maharashtra, India. E-mail: dramrajani@gmail.com
Introduction: Intraosseous hemangiomas (IH) are one of the rarest bone tumors that an orthopedic surgeon comes across, more so in the long bones. It most often affects adult females, severely blunting their activities of daily living, coupled with potential debilitating complications such as pathological fracture.
Case Presentation: We present a case of a 38-year-old female who presented with long standing pain and swelling in the left knee. Radiology, in the form of plain radiographs and magnetic resonance imaging, narrowed the diagnosis down to a benign form of osteoblastoma or hemangioma. With this in mind, the patient underwent radical excision of the lytic lesion, along with a margin of the surrounding normal bone. The defect was filled with impaction bone grafting and supplemented by a hydroxyapatite block and a poly ethyl ether ketone plate. The patient had excellent clinical, functional, and radiological outcomes at 6 months follow-up.
Conclusion: With the inherent rarity of IH, especially when it affects the long bones, it has barely been reported in orthopedic literature. Subsequently, management protocols for such lesions are ill-defined, which can be deleterious to the patient as well as the surgeon. Through this case report, we show how to approach a patient presenting with associated complaints, and show a detailed outline of an efficacious management regime that gave excellent outcomes in our patient.
Keywords: Intraosseous hemangioma, medullary hemangioma, management, treatment, diagnosis, outcome, functional, clinical, radiological, presentation.
Intraosseous hemangioma (IH) by itself is not a frequently-encountered entity and even when it does present, it usually affects the vertebral body and skull vault. When found in these bones, the diagnosis is not difficult due to its typical appearance. However, it is challenging to make a firm diagnosis on imaging when IH presents in unusual locations such as a long bone [1, 2]. Osseous hemangioma accounts for <1% of all primary skeletal neoplasms with about 75% in the vertebra or skull and 15–20% in the scapula, ribs, clavicle, and pelvic bones [2, 3, 4, 5]. Occurrence in long tubular bones is rather rare. The lesion is asymptomatic most of the time but may produce symptoms in cases of hematoma formation, epidural extension, vertebral body expansion, or pathological fracture [6, 7, 8]. On plain radiography, vertebral hemangiomas show the typical corduroy appearance, presenting with thickened vertical trabeculae of bone. On computed tomography (CT) images, a typical “polka dot” pattern is seen with small foci of sclerosis which stands for the thickened, vertically oriented bony trabeculae, and areas of low-density soft tissues or abnormal vessels and lipid are intervening between the vertically-oriented trabecula. Hemangiomas have a typical high signal intensity on both T1WI and T2WI of magnetic resonance imaging (MRI) due to abundant adipocytes, blood vessels, and interstitial edema [9].
Contrary to the hemangioma in the skull and spine with typical clinical presentations, correct diagnosis of this neoplasm may be very challenging when it occurs in the long tubular bones or demonstrates atypical imaging features [10]. We present such a case of histologically-proven IH affecting the proximal tibial metaphysis, describe its clinical findings, and an effective approach for its management.
A 38-year-old female presented with the left knee pain for the past 6 months with difficulty in walking, sitting cross-legged, and bending the knee. On clinical examination, the left knee range of motion was full with negative Mcmurray’s test and normal anterior and posterior drawer tests. The patient showed tenderness over the pes anserinus bursa site. On inspection, the left medial proximal tibial region showed redness and swelling (Fig. 1). Clinical findings were confirmed by radiographs in anterior posterior (AP) and lateral views (Fig. 2). Radiographs were suggestive of a sclerotic lesion localized to proximal medial and posteromedial tibia. Hyperintensity of the lesion was suggestive of disorganized trabeculae in addition to a sharp delineation between the affected and normal bone showing its benign nature.
Further, definition of the lesion was obtained using MRI which showed hyperintensity on T2 images in the proximal tibial region extending to medial and posteromedial zone up to the subarticular margin. T1 images showed moderate hypointensity. Perilesional bone marrow edema was seen with associated pes anserinus bursitis. It was concluded that the lesion was suggestive of either an osteoblastoma or a hemangioma (Fig. 3).

Since the lesion appeared to be well localized on radiography, surgical excision followed by histopathological examination was planned. Under spinal anesthesia, with the patient in supine position, and by a medial incision, the affected bone was exposed. Thorough exposure of the involved portion was done and sclerotic striations over the bone were visualized along with ridges. The edges of the lesions were marked using K-wires in AP and lateral views of intraoperative fluoroscopy and a window was created on the medial cortex.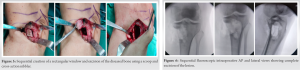
The excised bone from the window was removed and the underlying diseased bone was exposed. It had become calcified into presumptively dense trabeculae formed due to remodeling. Using a chisel, controlled resection of the affected bone was done. Further, deeper portions were removed using a cross-action nibbler and a scoop (Fig. 4, 5). Resection was confirmed sequentially on fluoroscopy (Fig. 6). Resection was done watchfully to avoid any iatrogenic fracture intraoperatively. Once the cavity was completely cleared of the diseased bone, thorough wash was given and allograft was impacted into it. After impaction of the allograft, breach in the cortical outline was supplemented using hydroxyapatite block and a three-hole medial support plate made of polyethyl ether ketone (PEEK) (Fig. 7). Fixation was done using three proximal and three distal titanium screws. Construct integrity was acceptable under fluoroscopy in AP and lateral views (Fig. 8). Skin was closed in layers. The patient was asked to resume active knee bending from the next day up to 90°. She was kept non weight-bearing on the operated side for 4 weeks. Histopathological examination was done of all the samples sent and a Cavernous Medullary IH was confirmed as the diagnosis. After 4 weeks, a repeat radiograph was performed. Radiographic union with incorporation of the bone allograft was observed (Fig. 9). Graduated weight-bearing was started and full range of motion exercises was done on the knee. At 8 weeks, the patient started walking with full weight-bearing and had regained almost full ranges of motion at the knee joint and was able to sit cross-legged too (Fig. 10). Pain at the surgical site subsided completely and the patient recovered with no complaints. The patient had been followed up for the next 6 months with no complaints and no recurrence of the lesion and the radiograph showing complete consolidation of the allograft with no obvious cortical defect (Fig. 9). Her functional outcome analysis was done using Musculoskeletal Tumor Society score at 2 months (88%) and 6 months (95%) postoperatively. Her International Knee Documentation Committee score at 6 months postoperatively was 81/87 (93.1%).
Presentation of cavernous medullary IH may vary, ranging from a completely asymptomatic lesion with an incidental finding on a radiograph to a painful, activity-limiting lesion requiring intervention. In our case, since the patient had severe pain with difficulty in carrying out the activities of daily living, intervention was required in the form of surgical excision and bone grafting with supplementary plating. At 6 months, the patient presented with a radiograph showing consolidation of the allograft and reformation of a continuous cortical outline.
Hemangioma is a rare bone lesion with a preponderance in 4th and 5th decade females [5]. Contrary to vertebral or calvaria hemangiomas which are mostly asymptomatic, extremity hemangiomas are symptomatic in most patients, with local swelling or a soft-tissue mass in 77% [2, 5, 10]. In our case too, the patient was a 38-year-old female with proximal tibial metaphysis involvement complaining of pain and having soft-tissue swelling. The medullary type of IH primarily occurs at the diaphysis or metaphysis with very little incidence of epiphyseal involvement. It usually presents as an osteolytic lesion with internal trabeculae showing a honeycomb or soap bubble appearance, due to the expansile proliferation of engorged vessels and thickened, remodeled bony trabeculae. Spiculated periosteal reaction may be present, and medullary hemangioma may also present as a completely lucent lesion on radiology [1]. The lesion in our case report was also a medullary IH of proximal tibial metaphysis. On exposure of the bone, there was an osteolytic lesion with formation of remodeled trabeculae which were very dense. Radiographically, the lesion in our case was radiopaque. Histologically, hemangiomas can be classified as cavernous, capillary, venous, or mixed, depending on the type of vascular involvement [5]. Cavernous hemangioma is the most common type in the peripheral bones and accounts for up to 50% of all cases reported [5]. They are predominant in the medullary and the intracortical portion of the bone and are not yet reported in the subarticular epiphyseal bone[5, 11, 12]. The lesion in our patient had its extension up to the subarticular margin which made its management further challenging. The differential diagnosis for a long bone hemangioma in juxta-articular location includes giant cell tumor, aneurysmal bone cyst, and plasmacytoma. IH can present with bizarre imaging appearances and should be included in the differential diagnosis of an osteolytic and expansile lesion of the epiphysis, especially in asymptomatic or mildly symptomatic patients [10]. In this case, however, radiographic appearance did not match any of the differentials mentioned and histopathological examination too confirmed the diagnosis as Cavernous Medullary IH. Satoh et al. believed that once bone hemangiomas have been diagnosed, the definitive treatment should be radical en bloc resection including surrounding intact tissue, to guarantee no recurrence and avoid the risk of massive bleeding [13]. However, we opted for a more conservative approach by excising only the affected bone along with some margin of surrounding normal bone so as to not leave back any pathological cell rests. After resection for solitary hemangioma in long bone diaphysis, a large defect is a challenge for the restoration of the biomechanics of the adjacent joints. Isacker et al. advocated the use of a bone allograft, because it allows for immediate restoration of the anatomy without harvesting or weakening another bone [14]. Same principles were used in our case for filling the void left behind by the excised diseased bone. After impaction of the allograft into the defect, we used an HA block to maintain cortical continuity and supplement the allograft impaction with a strong strut. Subsequently, stabilization and fixation using the biomaterial PEEK plate was done with the idea to retain as much local bio-integrity as possible. In a study by Li et al., the average MSTS functional score was 77% of normal function (53–90%) for all patients at 6 months postoperatively [15]. In our case, MSTS functional score was 88% at 2 months and 95% at 6 months postoperatively which was comparable, if not better.
Diagnosing Cavernous medullary hemangioma of proximal tibial metaphysis is really difficult due to its rare and variable presentations. We feel that MRI is the go-to investigation whenever such a lesion is suspected due to its consistent presentation of hyperintensity on T2WI and moderate hypointensity on T1WI. Based on the excellent functional and radiological outcomes in our patient, we suggest management of medullary IH by complete excision and debridement of the lesion and a margin of surrounding bone followed by impaction bone grafting (with or without supplementation by HA block) and plating for stabilization and fixation using a biomaterial such as PEEK for consistent results.
A high degree of suspicion in the susceptible population demographic and an aggressive diagnostic fervor is crucial for the detection of medullary IH even when it presents at unusual sites such as proximal tibial metaphysis. Radical resection of the lesion with bone grafting and if required, supplementary HA block insertion and plating gives excellent outcome.
References
- 1.Matsumoto K, Ishizawa M, Okabe H, Taniguchi I. Hemangioma of bone arising in the ulna: imaging findings with emphasis on MR. Skeletal Radiol 2000;29:231-4. [Google Scholar]
- 2.Shikhare S, Sittampalam K, Peh W, Shimpi T. Proximal ulna: A rare location for solitary intraosseous hemangioma. Oman Med J 2018;33:260-3. [Google Scholar]
- 3.Cao L, Wen JX, Han SM, Wu HZ, Peng ZG, Yu BH, et al. Imaging features of hemangioma in long tubular bones. BMC Musculoskelet Disord 2021;22:27. [Google Scholar]
- 4.Chandra SP, Singh P, Kumar R, Agarwal D, Tandon V, Kale SS, et al. Long-term outcome of treatment of vertebral body hemangiomas with direct ethanol injection and short-segment stabilization. Spine J 2019;19:131-43. [Google Scholar]
- 5.Kaleem Z, Kyriakos M, Totty WG. Solitary skeletal hemangioma of the extremities. Skeletal Radiol 2000;29:502-13. [Google Scholar]
- 6.Patnaik S, Jyotsnarani Y, Uppin SG, Susarla R. Imaging features of primary tumors of the spine: A pictorial essay. Indian J Radiol Imaging 2016;26:279-89. [Google Scholar]
- 7.Rodallec MH, Feydy A, Larousserie F, Anract P, Campagna R, Babinet A, et al. Diagnostic imaging of solitary tumors of the spine: what to do and say. Radiographics 2008;28:1019-41. [Google Scholar]
- 8.Theodorou DJ, Theodorou SJ, Sartoris DJ. An imaging overview of primary tumors of the spine: Part 1. Benign tumors. Clin Imaging 2008;32:196-203. [Google Scholar]
- 9.Abdel Razek AA, Castillo M. Imaging appearance of primary bony tumors and pseudo-tumors of the spine. J Neuroradiol 2010;37:37-50. [Google Scholar]
- 10.Chawla A, Singrakhia M, Maheshwari M, Modi N, Parmar H. Intraosseous haemangioma of the proximal femur: imaging findings. Br J Radiol 2006;79:e64-6. [Google Scholar]
- 11.Dorfman HD, Czerniak B. Vascular lesions. In: Bone Tumors. St. Louis, MO: Mosby; 1998. p. 729-814. [Google Scholar]
- 12.Wold LE, Swee RG, Sim FH. Vascular lesions of bone. Pathol Ann 1985;20:101-37. [Google Scholar]
- 13.Satoh K, Ohtsuka T, Abe T, Yokota K, Kunii K. Haemangioma of the forehead: Radiographic diagnosis and definitive surgical treatment in a Japanese series. Scand J Plast Reconstr Surg Hand Surg 2009;43:75-81. [Google Scholar]
- 14.van Isacker T, Barbier O, Traore A, Cornu O, Mazzeo F, Delloye C. Forearm reconstruction with bone allograft following tumor excision: A series of 10 patients with a mean follow-up of 10 years. Orthop Traumatol Surg Res 2011;97:793-979. [Google Scholar]
- 15.Zhaoxu LI, Tang J, Zhaoming YE. Solitary haemangioma of the shaft of long bones: Resection and reconstruction with autologous bone graft. Acta Orthop Belgica 2013;79:230-4. [Google Scholar]






