
Synovial chondromatosis, though rare, can be a cause of shoulder pain in an adolescent athlete. Arthroscopic removal is generally successful.
Dr. Heather M Menzer, Department of Orthopedic Surgery, Phoenix Children’s Hospital, Phoenix, Arizona, United States. E-mail: heathermenzermd@gmail.com
Introduction: Synovial chondromatosis refers to a benign proliferative disease of the synovium. Reports in children are rare and reports involving the pediatric shoulder are even more rare. In this review of the literature and case report, we provide a summary of all published cases in children and a report of a case of shoulder synovial chondromatosis in an adolescent female athlete.
Case Presentation: A 15-year-old female cheerleader presented to the clinic with gradual onset right shoulder pain with a severity of 5/10. On physician examination, the patient had tenderness over the proximal humerus, limited abduction to 160°, limited forward flexion, and a total arc of motion of <180°. Radiograph of the shoulder demonstrated multiple calcific intra-articular loose bodies consistent with synovial chondromatosis. Arthroscopic removal resulted in resolution of symptoms at the 36-week follow-up.
Conclusions: Our literature search revealed only eight case reports on shoulder synovial chondromatosis in children. The location of the chondromatosis within the shoulder joint can be intra-articular, extra-articular, within the biceps sheath, or combined. In general, for chondomatoses confined to the glenohumeral joint space, open surgery is not required. Bony erosions can occur in the setting of chondromatosis though may not need to be addressed surgically. Although rare, this diagnosis should be considered when confronted with shoulder pain that is exacerbated during long athletic events with limited range of motion on physical examination in the adolescent athlete. Arthroscopic treatment in conjunction with physical therapy and early mobilization can lead to a successful outcome.
Keywords: Synovium resection, arthroscopy, shoulder, adolescent medicine, sports medicine.
Synovial chondromatosis refers to a benign proliferative disease of the synovium [1]. The pathology was originally described in three distinct phases: Early, transitional, and late, with late being marked by the presence of several loose bodies [2]. It can broadly be classified by anatomic location [1], by the stage of disease [2], or by involvement: Extra-articular, intra-articular, bursal, or tenosynovial [1]. The disease has a male:female ratio of 2:1 and most commonly occurs in adults ages 30–50. The knee is the most common location overall. Within the upper extremity, the elbow is the most common location [1].
Management is generally based on patient symptoms. Arthroscopic removal can be pursued in cases with progressive activity tolerance, mechanical symptoms, or excessive pain. In adults, age and concurrent osteoarthritis are important when considering surgery [3]. A recent case series demonstrated good clinical results for surgical removal in adults [3]. However, there are no studies exploring surgical removal in children.
Reports of shoulder involvement are sparse overall and even fewer in children [4, 5, 6, 7, 8, 9, 10, 11, 12]. Of these reports, only one study reports a bony deformity [11], which was in the setting of a concurrent osteochondritis dissecans lesion. In this review of the literature and case report, we provide a summary of all published cases in children (Table 1) and a report of shoulder synovial chondromatosis in a 15-year-old female cheerleader with bony erosions.
Clinical presentation
A 15-year-old female national POM cheer competitor with no known medical history presents to the clinic with a week of the right shoulder pain. The pain was described as a nagging ache over the anterolateral arm with the severity rated as 5/10. It was exacerbated by pressure, movement, and cheer events. The symptoms were partially alleviated by ibuprofen. The patient denied any recent injury, trauma, swelling, mechanical symptoms, or neuropathic symptoms.
On physician examination, the patient had point tenderness over the proximal humerus, limited abduction to 160°, and limited forward flexion to 120°.
Imaging studies
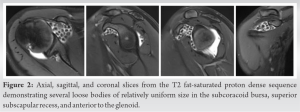
The patient’s primary care physician had ordered X-rays of the shoulder which demonstrated multiple calcified loose bodies in the axillary recess (Fig. 1). Erosions were also seen posteriorly on the scapular Y-view (Fig. 1c). MRI demonstrated several loose bodies in the subcoracoid bursa (Fig. 2).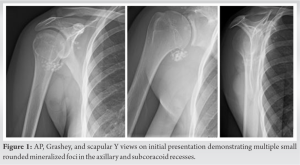
Treatment
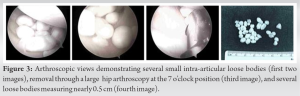
On diagnostic arthroscopy, no labral, rotator cuff, or biceps pathology were observed. Minor cartilage wear on the glenoid was noted. Several loose bodies were found intra-articularly (Fig. 3a, 3b). The loose bodies were removed through a large (hip arthroscopy) posteroinferior portal with a high inflow to act as a suction (Fig. 3c.) Extensive debridement around the rotator interval was performed to adequately remove all subcoracoid loose bodies. The same arthroscopic sequence was then repeated using both a 30° and 70° arthroscope. No loose bodies were found in the subacromial space. The specimens were sent for gross diagnosis to pathology and were described as multiple well-circumscribed gray-white portions of firm nodular tissue that was 3.5 cm in greatest dimension when aggregated (Fig. 3d).
Follow-Up
At 2 weeks postoperatively, the patient reported 0 out of 10 pain controlled with the use of naproxen only. The patient proceeded to discontinue all pain medications by 6 weeks postoperatively. Although the patient did initially note some discomfort with terminal flexion and abduction, this had completely resolved by 12 weeks postoperatively.
At the 7-month follow-up, the patient described aching within the shoulder and difficulty raising the arm over her head. The ache was recently aggravated as she was approaching her competitive cheer season. On physical examination, she had full range of motion, full strength, and no signs of instability. At this time, a diagnostic and therapeutic intra-articular shoulder steroid injection under ultrasound guidance was pursued. At 10 months postoperatively, the patient maintained 0 out of 10 pain at rest. The patient had returned to POM practices with no limitations. She did have some symptoms during prolonged POM practices with extended periods of overhead movement. She denied any symptoms of instability. On examination, the patient had full range of motion of forward flexion to 180°, abduction to 180°, external rotation to 80°, and internal rotation to L1. Five out of five strength in abduction, internal rotation, and external rotation were noted. Follow-up X-rays demonstrated resolution of the chondromatosis; however, bony erosions along the anterior and posterior humeral head were seen (Fig. 4).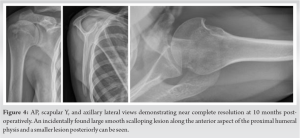
At the 49-month follow-up, the patient maintained complete resolution of symptoms. The patient did not report any pain or subjective instability. The patient maintained forward flexion to 180°, abduction to 180°, external rotation to 80°, and internal rotation to L1. Special testing did not reveal any signs of instability. Repeat radiographs demonstrated resolution of the synovial chondromatosis, yet the priorly seen bony erosions were again noticed (Fig. 5).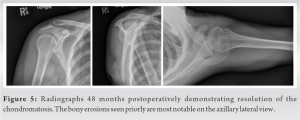
Shoulder synovial chondromatosis is rare and is especially rare in children. In this review of the literature and case report, we review all published cases of shoulder synovial chondromatosis in children and provide a unique case. Our literature review revealed only eight case reports on shoulder synovial chondromatosis in children (Table 1). One can note that only one of these eight cases was in self-reported athletes [11]. One can also note that seven of these eight cases were treated surgically, of which four involved open surgery due to the extent of the chondromatosis. There is a wide spectrum regarding the location of the chondromatosis in the pediatric population (Table 1). In our case, the chondromatosis was limited to the gleno humeral joint space (Fig. 1, 2, 3), and thus, an open surgical approach was not required.

Our case presents the unique features of concurrent bony erosions (Fig. 4) in the setting of shoulder synovial chondromatosis. However, our patient did not report any symptoms of instability nor was any instability noted on physical examination. Gill et al. 2017, presented the case of shoulder chondromatosis in a competitive golfer in the setting of a concave defect in the center of the humeral head [11]. On arthroscopy, this was diagnosed as concomitant osteochondritis dissecans. These two cases may highlight the fact that chondromatosis may alter the pressure environment within the shoulder and thus lead to bony erosions. To the best of our knowledge, there are no reports of other bony deformities in the setting of shoulder synovial chondromatosis in children. There are limited studies regarding arthroscopic synovectomy and loose body removal. A recent case series in adults demonstrated good clinical results (five out of five patients) with radiographic recurrence in two out of five patients [3]. The results of our review (Table 1) of the eight published cases in children demonstrate six out of eight cases reporting complete resolution of symptoms at last follow-up (two of eight cases did not have follow-up information.) Our case demonstrated good clinical results at 36 months, with a complete resolution of symptoms at rest, yet some symptoms during long POM practices were maintained.
Our case highlights the presentation of shoulder synovial chondromatosis in the adolescent athlete. Although rare, this diagnosis should be considered when confronted with shoulder pain that is exacerbated during long athletic events. Adolescent athletes with this condition may have full return to sport after arthroscopic treatment.
Arthroscopic removal and physical therapy may be the appropriate treatment for refractory shoulder synovial chondromatosis in adolescent athletes.
References
- 1.Ho YY, Choueka J. Synovial chondromatosis of the upper extremity. J Hand Surg Am 2013;38:804-10. [Google Scholar]
- 2.Milgram JW. Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801. [Google Scholar]
- 3.Urbach D, McGuigan FX, John M, Neumann W, Ender SA. Long-term results after arthroscopic treatment of synovial chondromatosis of the shoulder. Arthroscopy 2008;24:318-23. [Google Scholar]
- 4.Chillemi C, Marinelli M, De Cupis V. Primary synovial chondromatosis of the shoulder: Clinical, arthroscopic and histopathological aspects. Knee Surg Sports Traumatol Arthrosc 2005;13:483-8. [Google Scholar]
- 5.Kirchhoff C, Buhmann S, Braunstein V, Weiler V, Mutschler W, Biberthaler P. Synovial chondromatosis of the long biceps tendon sheath in a child: A case report and review of the literature. J Shoulder Elbow Surg 2008;17:e6-10. [Google Scholar]
- 6.Sprengers ME, Van Rijn RR. Diagnostic image (280). A female dancer with a painful shoulder. Ned Tijdschr Geneeskd 2006;150:1454. [Google Scholar]
- 7.Sinikumpu JJ, Sinikumpu SP, Sirniö K, Näpänkangas J, Sequeiros RB. Pediatric primary synovial chondromatosis of the shoulder, biceps tendon sheath and subcoracoid bursa. J Clin Orthop Trauma 2020;11:317-20. [Google Scholar]
- 8.Nashi M, Manjunath B, Banerjee B, Muddu BN. Synovial chondromatosis in a child: An unusual cause of shoulder pain case report. J Shoulder Elbow Surg 1998;7:642-3. [Google Scholar]
- 9.Miranda JJ, Hooker S, Baechler MF, Burkhalter W. Synovial chondromatosis of the shoulder and biceps tendon sheath in a 10-year-old child. Orthopedics 2004;27:321-3. [Google Scholar]
- 10.Ucpinar BA, Sahin C. Primary intra-articular and extra-articular synovial chondromatosis in a child: A rare cause of shoulder pain in children. J Coll Physicians Surg Pak 2020;30:1345-7. [Google Scholar]
- 11.Gill J, Tytherleigh-Strong G. Osteochondritis dissecans with associated secondary chondromatosis in an adolescent shoulder. Shoulder Elbow 2019;11:275-81. [Google Scholar]
- 12.Dwidmuthe SC, Nemade AS, Agrawal S, Pathak A. Rare case of extra-articular synovial chondromatosis of biceps tendon sheath in 8 years male child. J Orthop Case Reports 2014;4:33-6. [Google Scholar]








