
In high demand patients with isolated rectus femoris tears, allograft reconstruction is a valid treatment option.
Dr. Jed Walsh, Department of Orthopaedic Surgery, Inspira Health Network, 1505 W Sherman Ave, Vineland, NJ 08360, US. E-mail: walshj2@ihn.org
Introduction: Quadriceps ruptures, especially isolated rectus femoris ruptures, are uncommon among young and healthy individuals.
Case Report: We describe an 18-year-old collegiate sprinter with a rectus femoris tendon rupture who continued to have significant pain and dysfunction despite non-operative management. He was concurrently found to have femoroacetabular impingement and a labrum tear as well. Following an extensive trial of non-operative management, operative fixation of the rectus femoris rupture with Achilles allograft reconstruction was performed in addition to arthroscopic labrum fixation and femoroplasty. Postoperatively, he returned to sport with improved mobility and decreased pain.
Conclusion: Surgical rectus femoris tendon reconstruction with Achilles allograft is a valid option for patients who fail conservative treatment.
Keywords: Isolated rectus femoris rupture, quadriceps rupture, Achilles allograft reconstruction
Quadriceps tendon ruptures (1.37/100,000) are uncommon among young and healthy individuals with most reported cases involving eccentric contraction and some form of direct trauma, iatrogenic injury, or illness [1, 2, 3, 4, 5, 6, 7]. In the rare event of a quadriceps muscles injury, the rectus femoris muscle is the most likely injured due to its superficial location, muscle fiber composition, and extension across two joints [8]. Quadriceps ruptures commonly occur within 1–2 cm of the superior pole of the patella in younger patients due to a relatively hypovascular zone [9]. An alternative injury pattern seen in the rectus femoris muscle is avulsions injuries to the proximal rectus femoris junction with surgical excision being a valid treatment option [10]. Few reports have described surgical treatment of a distal rectus femoris tendon rupture. Non-operative management of distal rectus femoris injuries can result in limited reduction of function. However, in cases with continued pain and dysfunction, surgical treatment is recommended to definitively treat these injuries. This may be the case in high-level athletes [11]. Femoroacetabular impingement (FAI) is common in young athletes, presenting with a higher prevalence than the general population [12, 13]. FAI has been shown to limit the range of motion of the hip joint and contribute to a wide variety of intra-articular pathologies. In this case report, we present a rupture of the rectus femoris, cam type FAI, and labrum tear. We discuss the patient’s clinical presentation, diagnoses, and ultimately successful surgical treatment.
An 18-year-old male, healthy collegiate sprinter, presented with a chronic tear of his right rectus femoris tendon. A year prior, he was running high school track when he felt a pop in his right thigh and developed an obvious deformity. Physical therapy was attempted with incomplete recovery and continued thigh and groin pain, resulting in an occasional antalgic gait. He also felt subjective limitation in his athletic ability. Due to his continued symptoms, he sought a second opinion with the primary investigator. Physical examination of the thigh demonstrated an obvious subcutaneous deformity, similar to a “Popeye” type sign seen in the proximal biceps, with a palpable defect in the quadriceps tendon. Knee range of motion was 0–120° and he was tender to palpation along the distal tendon stump. Hip range of motion was 110° of flexion, 15° of extension, 35° of internal rotation, and 45° of external rotation. Internal impingement sign was positive reproducing the patient’s pain in his groin.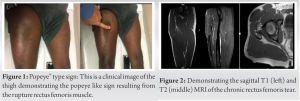
MRI of the right lower extremity and MR arthrogram of the right hip demonstrated a complete tear of the rectus femoris tendon without atrophic changes, a CAM lesion with an alpha angle of 70°, and anterior-superior labrum tearing. A trial of conservative management was attempted with activity modification, physical therapy, and an intra-articular hip injection for both diagnostic and therapeutic purposes. With the injection, we attempted to isolate the patient’s symptoms as coming from intra-articular hip pathology or from the rectus femoris rupture. The injection relieved his groin pain for approximately 1 week with continued irritation in the thigh, especially isolated around the tendon stump. An attempt was made with the patient to elucidate the true nature of the symptoms. He sincerely felt that the groin pain, which was temporarily relieved from the injection, was significant and independent pain from the pain, he experienced at the region of the tendon stump. The pain at the tendon stump continued to bother him during the week of relief from the groin pain. Furthermore, after the initial response to the injection, the patient felt that both areas of pain were significant to his overall limitations and symptoms. At this point, the patient had failed conservative therapy with both the intra-articular pathology and rectus femoris rupture deemed significant sources of his persistent symptoms. Surgery was recommended for both hip and tendon pathologies. The primary surgeon and patient jointly decided to address the rectus femoris rupture with reconstruction and the intra-articular hip pathologies through hip arthroscopy. For the rectus femoris, the patient was positioned supine on a traction table. A midline incision, in line with the quadriceps tendon, was made at the site of tendon rupture from the tendon stump to the proximal patella. The distal stump of the rectus femoris was isolated circumferentially. There was approximately 4 mm of relatively thin rectus femoris tendon stump remaining. The tendon stump was sutured with multiple loops of Fiberwire (Arthrex, Naples, FL). The Achilles allograft was then obtained and sutured medially and laterally in a running Krackow fashion. The Achilles graft was fanned out and tacked to the rectus femoris muscle belly utilizing approximately 15 simple interrupted #2 Ethibond (Ethicon, Cincinnati, OH) sutures. Fiberwire (Arthrex, Naples FL) was utilized to connect the tendon graft to the remaining rectus femoris tendon stump in a Krakow fashion medially and laterally. Attempting to balance anatomic location versus graft/tendon tension, the rectus femoris complex was pulled over the distal intact quadriceps tendon. While maintaining tension, #2 Fiberwire (Arthrex, Naples, FL) was passed in a running Krakow fashion medially and laterally through the graft and quadriceps tendon from musculotendinous margin to the proximal patella and back. Once completed, the graft and rectus femoris had excellent stability throughout knee range of motion.
For the hip arthroscopic procedure, the hip was placed under traction. Three portals were utilized: Anterolateral, mid-anterior, and distal anterolateral accessory. Diagnostic arthroscopy demonstrated a labral tear from the 12:30 to 3:00 position. The acetabular rim was decorticated. For the 1:00 position and 2:30 position, knotless Cinchlock anchors (Stryker, Kalamazoo, MI) were utilized to affix the labrum. Traction was then released and restoration of the suction seal nature of the labrum was confirmed. Attention was then turned to the arthroscopic femoroplasty. The convex protuberance of bone consistent with a CAM lesion was noted at the 1–3 o’clock position. A burr was used to recontour the femoral head-and-neck junction to a concave structure. This was confirmed by direct visualization and intraoperative radiographs. Following the arthroscopic procedure, the rectus femoris reconstruction was rechecked and intact. All skin incisions were then closed and dressed. Postoperatively, the patient was placed in a locked knee immobilizer and recommend toe-touch weightbearing for 3 weeks. Physical therapy was initiated after 2 weeks with a gradual progression of weightbearing after 3 weeks. Knee flexion was initiated at 2 weeks with 15 degrees per week until full motion. No quadriceps resistance was allowed until 3 months. Six months following the operation, the patient was cleared to return to sports. There were no complications encountered.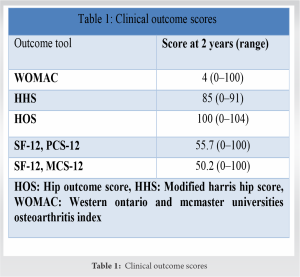
Isolated rectus femoris ruptures are uncommon injuries. Of the few reported cases, operative and non-operative modalities have been utilized in the treatment of these patients. Weber et al. utilized non-operative management with an emphasis on continued muscle strengthening and physical therapy. Their patient was a middle-aged male and non-professional triathlon athlete, without any perceived functional limitations. He had favorable outcomes with non-surgical management leading the authors to advocate for non-operative management [11]. Straw and Taylor et al. reported cases of young athletes in which surgical repair or reconstruction was utilized. In both instances, the patient complained of athletic limitation and difficulty returning to sport. Straw utilized surgical correction of the rectus femoris leading to a restoration of concentric and eccentric strength to the affected quadriceps [14]. Taylor et al. elected for surgical management with augmentation of their repair with a ligament repair and reconstructive solution (LARS) (Corin Group, Cirncester, UK) [15]. In both instances, the athletes were able to return to pre-injury levels of competition. Despite extensive physical therapy and non-operative modalities, our patient continued to have pain and subjective athletic limitation, leading to surgical management. Two years following the surgical reconstruction, the following clinical outcome measures were obtained: Western ontario and mcmaster universities osteoarthritis index, modified harris hip score, hip outcome score, and Short Form Survey (Table 1) [16, 17, 18, 19]. Overall, the patient’s functional status had improved with both decreased pain and decreased subjective limitation. These are similar clinical results to those seen in direct repair and LARS augmentation. Deep squatting, pivoting, and application of socks continued to give the patient slight difficulty, but the patient felt that his overall function had significantly improved. There are some clear limitations highlighted beyond that of a typical case report. Ideally, the case report would have involved isolated treatment of a single pathology. The authors acknowledge that the multiple pathologies complicate the clinical presentation, management, and eventual outcome. Each of these pathologies individually could have been managed operatively or nonoperatively. It is possible that managing simply the FAI and labrum tear would have provided sufficient relief to give the patient clinical benefit, but the decision was made based on attempts at isolating the contribution of each pathology. Both the patient and physician agreed that each of the two pathologies contributed to the patient’s overall experience of significant and limiting hip and thigh pain. Therefore, the decision was sound to address both conditions and the patient was able to return to activity with decreased symptoms following the management of both conditions. Furthermore, while the patient was able to successfully return to his sport, quantitative strength testing was not performed either preoperatively or postoperatively. The patient’s ability to return to sport and clinical improvements suggests that the surgical management of the ruptured tendon was successful regardless of the concurrent management of his impingement and labrum tear.
When considering the optimal treatment for rectus femoris injury, patient specific characteristics are important in deciding between operative and non-operative management. For patients who have failed non-operative treatment and whom experience significant pain and dysfunction from the rectus femoris, tendon reconstruction with Achilles allograft should be considered and may result in improved clinical outcomes.
Isolated complete rupture of the rectus femoris is an uncommon injury. Non-surgical and surgical modalities should be thoroughly discussed with the patient. In select patients, surgical reconstruction of the rectus femoris can provide beneficial outcomes.
References
- 1.Clayton RA, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury 2008;39:1338-44. [Google Scholar]
- 2.Gao X, Shao Z, Liu S, Xiang J. A case report of spontaneous rupture of the quadriceps tendon. Clin Case Rep 2017;5:1477-81. [Google Scholar]
- 3.Adolphson P. Traumatic rupture of the quadriceps tendon in a 16-year-old girl. Arch Orthop Trauma Surg 1992;112:45-6. [Google Scholar]
- 4.Alexander VA, Keilin S, Cohn BT. Adolescent quadriceps mechanism disruption. Orthopedics 2001;24:591-3. [Google Scholar]
- 5.Aydemir G, Cakmak S, Aydinoz S. Partial rupture of the quadriceps muscle in a child. BMC Musculoskelet Disord 2010;11:214. [Google Scholar]
- 6.Khanna G, El-Khoury G. Partial tear of the quadriceps tendon in a child. Pediatr Radiol 2008;38:706-8. [Google Scholar]
- 7.Shimba LG, Latorre GC, de Castro Pochini A, Astur DC, Andreoli CV. Surgical treatment of rectus femoris injury in soccer playing athletes: Report of two cases. Rev Bras Ortop 2017;52:743-7. [Google Scholar]
- 8.Figved W, Grindem H, Aaberg M, Engebretsen L. Muscle strength measurements and functional outcome of an untreated complete distal rectus femoris muscle tear. BMJ Case Rep 2014;2014:bcr2013203191. [Google Scholar]
- 9.Pengas I, Assiotis A, Khan W, Spalding T. Adult native knee extensor mechanism ruptures. Injury 2016;47:2065-70. [Google Scholar]
- 10.Sonnery-Cottet B, Barbosa NC, Tuteja S, Gardon R, Daggett M, Monnot D, et al. Surgical management of rectus femoris avulsion among professional soccer players. Orthop J Sports Med 2017;5:232596711668394. [Google Scholar]
- 11.Weber M, Knechtle B, Lutz B, Stutz G, Baumann P. Nonoperative treatment of a complete distal rectus femoris muscle tear. Clin J Sport Med 2010;20:493-4. [Google Scholar]
- 12.Lee WY, Kang C, Hwang DS, Jeon JH, Zheng L. Descriptive epidemiology of symptomatic femoroacetabular impingement in young athlete: Single center study. Hip Pelvis 2016;28:29-34. [Google Scholar]
- 13.Frank JM, Harris JD, Erickson BJ, Slikker W, Bush-Joseph CA, Salata MJ, et al. Prevalence of femoroacetabular impingement imaging findings in asymptomatic volunteers: A systematic review. Arthroscopy 2015;31:1199-204. [Google Scholar]
- 14.Straw R. Surgical repair of a chronic rupture of the rectus femoris muscle at the proximal musculotendinous junction in a soccer player. Br J Sports Med 2003;37:182-4. [Google Scholar]
- 15.Taylor C, Yarlagadda R, Keenan J. Repair of rectus femoris rupture with LARS ligament. Case Rep 2012;2012:bcr0620114359. [Google Scholar]
- 16.WOMAC-AUSCAN-Osteoarthritis Global Index. Available from: https://www.womac.com/womac/index.php [Last accessed on April 15th, 2021]. [Google Scholar]
- 17.Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am 1969;51:737-55. [Google Scholar]
- 18.Thorborg K, Roos EM, Bartels EM, Petersen J, Hölmich P. Validity, reliability and responsiveness of patient-reported outcome questionnaires when assessing hip and groin disability: A systematic review. Br J Sports Med 2010;44:1186-96. [Google Scholar]
- 19.Jenkinson C, Layte R. health survey). J Health Serv Res Policy 1997;2:14-8. [Google Scholar]






