In cases with combined ACL and LCL injuries, both can be reconstructed using single STG graft and single femoral tunnel, thereby decreasing morbities, operative time and preserving bone
Dr. Bhagya R Shah, Department of Orthopaedics, Smt. B. K. Shah Medical Institute and Research Center, Sumandeep Vidyapeeth Deemed to be University, Vadodara, Gujarat, India. E-mail: bhagyashah.com@gmail.com
Introduction: Anterior cruciate ligament (ACL) injury is associated with various degrees of rotational deformity. About 15% have a positive pivot shift test after accurate ACL reconstruction. Unrepaired lateral collateral ligament (LCL) tear can lead to increase load on reconstructed ACL and lead to ligament failure.
Case Report: We present a case of combined ACL with LCL tear treated arthroscopically using a single femoral tunnel and asymmetric combined semitendinosus and gracilis (STG) graft. The patient had full range of motion at the knee joint and was able to squat and sit cross-legged and was able to carry out activities of daily living at 8 months of follow-up.
Conclusion: Our technique provides orthopedic surgeons with an alternative for combined ACL and LCL reconstruction with a single combined STG graft, thereby limiting additionally graft site morbidity and avoiding the need for allograft and preserving adequate femoral bone stock by preparing only a single femoral tunnel and thus limiting the cost to the patient using single implant for femur.
Keywords: Anterior cruciate ligament + lateral collateral ligament tear, single femoral tunnel reconstruction, multi-ligamentous knee injury, single semitendinosus and gracilis graft.
An anterior cruciate ligament (ACL) injury usually leads to rotating deformities, and a residual pivot shift has been reported in more than 15% of case studies following an accurate ACL reconstruction. Studies on the lateral collateral ligament (LCL) have improved understanding of its function and biomechanical function in providing rotational stability to the knee joint. To restore normal knee kinematics, this knowledge redirected and refocused attention on extra-articular reconstruction of the LCL in conjunction with intra-articular ACL reconstruction. Unrepaired LCL tear leads to increased load among reconstructed ACL, leading to its failure [1]. Therefore, careful assessment of all injured ligaments should to recognized and multi-ligament reconstruction should be considered. It has been shown in biomechanical studies that the lateral collateral ligament is an important anatomical structure that resists varus forces and external rotation [2]. Most common mechanism of the injury is varus forces across the knee, a direct blow on the medial side of the knee joint, or a non-contact injury like hyperextension stress, leading to multi-ligament injury in the knee joint. Grade III LCL injuries were seen in association with an ACL tear in approximately 57% of cases [3]. We present a case of combined ACL with LCL tear treated arthroscopically using a single femoral tunnel and asymmetric combined Semitendinosus and gracilis (STG) graft.
A 25-year-old male presented to SBKS MI&RC, Dhiraj Hospital with complaints of instability of the right knee joint with difficulty in walking, climbing upstairs, squatting, and cross-leg sitting for 1 month. The patient had a history of Road Traffic Accident (bike collision) 1 month back sustaining a right knee injury. On local examination effusion was noted and there was no tenderness around the knee joint. The knee range of movement was full and free. The tests for ligamentous instability (Lachman, etc.) are positive, suggesting a combined LCL and ACL injury clinically. MRI right knee is suggestive of near complete ACL tear with buckling of posterior cruciate ligament and Complete tear of lateral collateral ligament with mild knee joint effusion (Fig. 1). The patient was operated on for arthroscopic ACL reconstruction along with mini-open non-anatomic LCL reconstruction using asymmetric STG graft with a single femoral tunnel and had a successful outcome.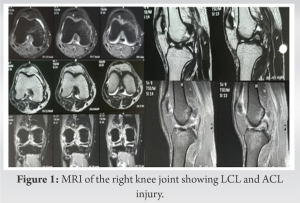
Surgical Technique
Patient positioning
Patient positioned supine with knee kept in 90º hanging at end of the table.
Graft harvesting
A 3 cm vertical incision was made anteromedially at 2.5 cm medial and 2.5 cm distal to the level of the tibial tuberosity. STG tendons were identified and harvested using an open-loop tendon stripper [4].
Graft preparation
Running whipstitch sutures were taken combining both grafts forming a single graft. The graft was made to have two arms, a short arm (triple strand) for ACL grafting and the larger one (single strand) used for lateral collateral ligament reconstruction (Fig. 2a). Graft with shorter arm (triple strand) had doubled strand of gracilis graft and single strand from semitendinosus graft with total short arm length being around 11 cm. Markings were made at a distance of 3.5 cm from both ends on the shorter arm for the femur and tibia with maintaining around 4 cm of joint space in between with a sterile marker. Graft with a longer arm was kept at its full length of 26 cm and prepared with whipstitch pull-out sutures. The diameter of the STG graft’s short arm was 9 mm [5].
Portals used
Two standard knee arthroscopy portals were made, one anterolateral and the other one anteromedial. An accessory medial portal was also made.
Tunnel preparation
A total of three tunnels were prepared, one femoral tunnel and two tibial tunnels for ACL reconstruction and LCL reconstruction, drilledfully as per graft diameter. The femoral tunnel was prepared by the inside-out technique and the tibial tunnel is prepared by the outside-in technique using the ACL Jig.
Tunnel preparation for ACL: Femoral tunnel preparation
Using inside out technique and knee in hyperflexion beath pin was passed at 10 o’clock position on ACL femoral remnant, over the medial border of the lateral femoral condyle in the intercondylar notch directing toward over the top position, the proximal end of the lateral femoral condyle, thereby locating its exit over the lateral femoral condyle and confirming under image intensifier guidance. Beath pin was made to penetrate out of the skin and clamped. As per the harvested graft diameter, the femoral tunnel was drilled with 9 mm, and then at the other end of the beath pin a suture loop was attached, which was later passed inside the joint. On the lateral aspect of the knee, where the beath pin was penetrating a vertical skin incision around 2.5 cm which was taken and the iliotibial band was identified and split and the femoral tunnel was identified, just proximal to the lateral femoral condyle.
Tibial tunnel preparation
Then, a tibial tunnel for ACL reconstruction was prepared with help of ACL Jig, in which a marking hook was placed at the crater of the ACL stump, posterior to the anterior horn of lateral meniscus, and Jig was angled at about 55º and the bullet was kept over the graft harvesting site at an angle of 30º medial to the mid-sagittal axis for outside-in technique. A guide pin was passed through the bullet and drilled with a 9 mm drill bit. The sutured loop attached to the beath pin passing through the femur, which was lying inside the joint was then pulled out from the outer end of the tibial tunnel with the help of a probe or grasper. Beath pin was removed from the loop, leaving one end of the loop suture outside the femoral tunnel and the other outside the tibial tunnel. Then, the STG graft with both the arms with whipstitch sutures was tied over the loop, followed by shuttling of the loop pulling the graft first through the tibial tunnel followed by femoral tunnel until the 3.5 cm marking on the short arm of the STG graft crosses the femoral tunnel entry inside and the long arm was pulled outside the femoral tunnel (Fig. 2b).
Fixation of ACL
Once both the long and short arms of the STG graft was through the femoral tunnel and crossed the 3.5 cm mark, a PEEK screw measuring 9 × 25 mm was inserted into the femoral tunnel using a guide wire. After cyclic knee loading, the graft was held in tension at the tibial side and knee in 30° flexion, and PEEK screw measuring 9 × 25 mm was inserted into the tibial tunnel using a guide wire and the remaining graft was sutured with the remnant of STG graft.
Tunnel preparation for LCL
A 3 cm vertical incision was taken just anterior to the fibula head centered between Gerdy’s tubercle and the fibula head. A short soft-tissue tunnel was prepared from the lateral aspect of the femoral condyle beneath the iliotibial band and passed distally to open out in front of the fibular head. Through this short tunnel STG graft, long arm was passed using long artery forceps (Fig. 2c). Beath pin was passed from the lateral aspect of the proximal tibia just posterior to Gerdy’s tubercle and anterior to the fibular head and directed medially and slightly distally so as to avoid ACL tibia tunnel and coming out through the graft harvesting incision. The tibial tunnel for LCL was prepared by drilling with STG graft long arm diameter, which was 4.5 mm. Again beath with shutting loop suture was used to pass STG graft long arm through the tunnel. The graft was tensioned by applying valgus force and 30° knee flexion and by pulling the whipstitch suture end of the graft medially (Fig. 2d).
Fixation of LCL graft
LCL fixation was done using a peek screw measuring 4.5 × 30mm from the lateral aspect of proximal tibia toward medially using a guide wire for rigid fixation (Fig. 2e-g). Postoperatively, the patient was given (Fig. 2f) an extension knee brace to immobilize the knee range of movements and was allowed partial weight-bearing walking with the help of a walker. Post-operative dressing was done at POD 2, POD 5, and POD 12, and suture removal was done on a post-operative day 12. According to the post-operative protocol for the ACL rehabilitation protocol, the patient was started on physiotherapy such as static quadriceps strengthening exercises, hamstring and quadriceps strengthening, and knee range of movements gradually. The patient in immediate post-operative period was made to walk partial weight bearing with the walker with an extension knee brace and complete weight bearing with extension knee brace following suture removal. After 3 weeks, close chain exercises were started. Moreover, at the end of 6 weeks, the patient was able to walk independently.
Follow-up
The total follow-up period was of 8 months postoperatively. At the final follow-up, the patient had a satisfactory range of movement in the operated knee. In addition to walking, climbing stairs, squatting, and sitting cross-legged, he is able to perform activities of daily living and is able to return to his occupational role as a labourer. There were no complications seen in the immediate post-operative and late post-operative period (Fig. 3).
Various techniques exist for the management of combined ACL and LCL/posterolateral corner (PLC) injuries as well as their management in a combined single-stage or two-staged manner [6]. The rate of failure for primary ACL reconstruction is between 0.7% and 8% and failure for graft revision is about 5% to 52% [7]. Many authors have suggested that the main cause of graft failure was untreated associated PLC ligament injury, so the reconstruction should be combined [1, 8, 9]. Our surgical technique uses a single tunnel in lateral femoral condyle in contrast to multiple tunnels used for multi-ligament reconstruction. Only a single STG graft with a single femoral tunnel was used in our technique for ACL and LCL reconstruction. Angelini et al. also described the use of a single femoral tunnel and combined STG graft for combined ACL and LCL injuries and emphasized the need for adequate graft size [10]. Our technique uses the regular hamstring tendon graft harvesting technique which includes STG graft with which most surgeons are familiar [4]. Moreover, the time loss associated with the graft harvesting is compensated by the time saved as only one femoral tunnel is required as compared to the two tunnels. Two tunnels technique used for combined ACL and LCL reconstruction have problems of getting converged over the lateral femoral wall [7]. The single tunnel has an advantage in revision surgery that it does not confluence in future surgery [10]. In this technique, we have used three strands for ACL and one strand for LCL. Native LCL has got tensile strength of about 295N, so according to Espejo-Baena et al., the reconstructed LCL has thrice the strength of the native LCL and has no chances of graft failure and thus making it a stable construct [11, 12]. Anatomic reconstruction of ACL is combined with non-anatomic reconstruction of LCL since LCL insertion is slightly anterior to the fibula head but posterior to Gerdy’s tubercle. Since we remain relatively far away from the peroneal nerve, this technique is safer than anatomic reconstruction and is more reliable, simpler, easier, and faster. For both the ACL and the LCL, peek screws were used for graft fixation. Using a peek screw ensures a good, stable fixation with a rigid structure. A femoral PEEK screw was placed inside-out, whereas a tibial PEEK screw was placed outside-in. Thus, two tibial PEEK screws and one femoral PEEK screw were used. A few authors advocate multi-staged reconstruction for chronic ACL and LCL injuries associated with genu varus malalignment [13]. According to Fanelli et al., patients with concomitant ACL and LCL reconstructions showed successful outcomes in 97.1% of cases and a mean Lysholm score of 91.8 [14]. There was a 38% failure rate reported in a systematic review for multi-staged reconstruction of acute grade III PLC injuries, compared to 9% for single-stage reconstructions with concurrent reconstructions of cruciate injuries [15]. According to Dhillon et al., knees with additional varus opening treated conservatively with significant adverse effects on reconstructed ACLs [16]. This technique fulfills the requirement of treatment of multi-ligament knee injury with a single combined graft and single femoral tunnel thus reducing the graft donor site morbidity, avoiding the need for multiple femoral tunnels and grafts, as well saving time, and providing a rigid construct.
Our technique provides orthopedic surgeons with an alternative for combined ACL and LCL reconstruction with a single combined STG graft, thereby limiting additionally graft site morbidity and avoiding the need for allograft, and also preserving adequate femoral bone stock by preparing only a single tunnel and limiting the cost to the patient using single implant for femur.
Treating ACL with LCL tear can be challenging. Introducing this technique can be helpful and relatively less traumatic for patients, decreases the operative time as well it is a bone preserving as only single tunnel is used.
References
- 1.LaPrade RF, Resig S, Wentorf F, Lewis JL. The effects of grade III posterolateral knee complex injuries on anterior cruciate ligament graft force. A biomechanical analysis. Am J Sports Med 1999;27:469-75. [Google Scholar]
- 2.Coobs BR, LaPrade RF, Griffith CJ, Nelson BJ. Biomechanical analysis of an isolated fibular (lateral) collateral ligament reconstruction using an autogenous semitendinosus graft. Am J Sports Med 2007;35:1521-7. [Google Scholar]
- 3.Geeslin AG, LaPrade RF. Location of bone bruises and other osseous injuries associated with acute grade III isolated and combined posterolateral knee injuries. Am J Sports Med 2010;38:2502-8. [Google Scholar]
- 4.Frank RM, Hamamoto JT, Bernardoni E, Cvetanovich G, Bach BR Jr., Verma NN, et al. ACL reconstruction basics: Quadruple (4-strand) hamstring autograft harvest. Arthrosc Tech 2017;6:e1309-13. [Google Scholar]
- 5.Vinagre G, Kennedy NI, Chahla J, Cinque ME, Hussain ZB, Olesen ML, et al. Hamstring graft preparation techniques for anterior cruciate ligament reconstruction. Arthrosc Tech 2017;6:e2079-84. [Google Scholar]
- 6.Fanelli GC, Edson CJ. Surgical treatment of combined PCL-ACL medial and lateral side injuries (global laxity): Surgical technique and 2-to 18-year results. J Knee Surg 2012;25:307-16. [Google Scholar]
- 7.Selim NM. Combined anterior cruciate ligament and posterolateral corner reconstruction by hamstring tendon autografts through a single femoral tunnel by graft-to-graft suspension and fixation. Arthrosc Tech 2018;7:e557-67. [Google Scholar]
- 8.Kannus P. Nonoperative treatment of grade II and III sprains of the lateral ligament compartment of the knee. Am J Sports Med 1989;17:83-8. [Google Scholar]
- 9.LaPrade RF, Hamilton CD, Engebretsen L. Treatment of acute and chronic combined anterior cruciate ligament and posterolateral knee ligament injuries. Sports Med Arthrosc Rev 1997;5:91-9. [Google Scholar]
- 10.Ange lini FJ, He lito CP, Tozi MR . Combined reconstruction of the anterior cruciate ligament and posterolateral corner with a single femoral tunnel. Arthrosc Tech 2013;2:e285-8. [Google Scholar]
- 11.LaPrade RF, Bollom TS, Wentorf FA, Wills NJ, Meister K. Mechanical properties of the posterolateral structures of the knee. Am J Sports Med 2005;33:1386-91. [Google Scholar]
- 12.Espejo-Baena A, Molano-Bernardino C, Espejo-Reina A, Espejo-Reina MJ, Rosa-Nogales JD. Associated anterior cruciate ligament and fibular collateral ligament reconstruction with single femoral tunnel and asymmetric hamstring tendon graft. Arthrosc Tech 2018;7:e797-804. [Google Scholar]
- 13.LaPrade RF, Johansen S, Agel J, Risberg MA, Moksnes H, Engebretsen L. Outcomes of an anatomic posterolateral knee reconstruction. J Bone Joint Surg Am 2010;92:16-22. [Google Scholar]
- 14.Fanelli GC, Fanelli DG, Edson CJ, Fanelli MG. Combined anterior cruciate ligament and posterolateral reconstruction of the knee using allograft tissue in chronic knee injuries. J Knee Surg 2014;27:353-8. [Google Scholar]
- 15.Geeslin AG, Moulton SG, LaPrade RF. A systematic review of the outcomes of postrolateral corner knee injuries, Part 2 surgical treatment of chronic injuries. Am J Sports Med 2016;44;1616-23. [Google Scholar]
- 16.Dhillon M, Akkina N, Prabhakar S, Bali K. Evaluation of outcomes in conservatively managed concomitant Type A and B posterolateral corner injuries in ACL deficient patients undergoing ACL reconstruction. Knee 2012;19:769-72. [Google Scholar]