
Femoral neck system (FNS) is a viable option for the treatment of femoral neck fractures in patients with above knee amputations.
Dr. Imran Gruhonjic, Department of Orthopedic Surgery, SSM Health St. Anthony’s Hospital, 1111 N Dewey Ave, Oklahoma City, OK 73103, United States. E-mail: Imran.gruhonjic@ssmhealth.com
Abstract
Introduction: Femoral neck fractures in patients with a history of above knee amputation present as a strain for orthopedic surgeons due to the difficulty of positioning and handling of the limb for proper reduction. Surgical treatment options typically involve open reduction internal fixation versus arthroplasty depending on patient factors such as age, surgeon skill, and available equipment.
Case Report: We present a case of a femoral neck fracture (OTA 31-B2) in a relatively active 89-year-old Caucasian male after a ground level fall that has been ambulating with a prosthesis since his teenage years. In this report, we describe the patient positioning, technique used to treat a femoral neck fracture (OTA 31-B2) using the femoral neck system, and the successful outcome of our patient 1 year from the injury.
Conclusion: We conclude that using the femoral neck system (FNS) is a viable option for patients with a high above knee amputation where, due to the length of the limb and potentially the lack of appropriately sized implants, dislocating and reducing the hip for total hip arthroplasties and hemiarthroplasties provide a challenge.
Keywords: Femoral neck fracture, geriatric trauma, open reduction internal fixation, femoral neck system, arthroplasty.
This article outlines the presentation of a femoral neck fracture in an above knee amputee. Femoral neck fractures are common injuries that occur in the elderly population. In this cohort, these injuries typically occur after a ground level fall. The patient presents with an inability to ambulate, pain, and a limb that is shortened and externally rotated. Femoral neck fractures in patients with a history of above knee amputation present as a strain for orthopedic surgeons due to the difficulty of positioning and handling of the limb for proper reduction [1]. Treatment options range from non-operative to operative, in which the surgical options are divided into open reduction internal fixation and arthroplasty. Many patient and fracture characteristics, including age, physiologic age, fracture propagation and location, length of femur available, in addition to many more are looked at carefully before selecting a treatment option. Common arthroplasty options are total hip arthroplasty and hemiarthroplasty. Open reduction internal fixation can occur using plates/screws, sliding hip screw, and the femoral neck system to name a few. Mobilizing the patient as soon as possible is the primary goal of treatment due to the increased risk of morbidity and mortality in patients with delayed or non-operative care [2].
An 89-year-old male with a right above knee amputation presented to the Emergency Department after sustaining a ground level fall. He had undergone an above knee amputation when he was a teenager after an accident involving a shotgun blast. He was carrying several guns he thought were unloaded when he tripped and dropped them causing one of the guns to fire, unloading into his right leg. It was deemed to be unsalvageable at that time, so an above knee amputation was performed. Since then, he had been ambulating with a prosthesis. Before the fall, he functioned independently for all activities of daily living. Our encounter with him began in the emergency department after he tripped over a pew while in church. The patient underwent a full clinical and radiographic evaluation. On examination, he was 74.8 kg, unable to ambulate, had pain with log roll of the residual limb, and had limited range of motion of his right hip due to pain. He was neurovascularly intact distally. Plain radiographs (Fig. 1, 2) demonstrated a status post above knee amputation with a displaced right femoral neck fracture (OTA 31-B2) and retained bullet fragments.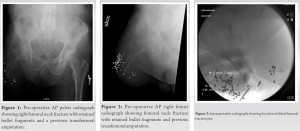 Due to the patient’s prior history of independence, he was counseled and surgical repair was recommended. Due to the length of the residual limb, the difficulty to manipulate it for proper dislocation and reduction, and the lack of appropriately sized implants for the length of femur remaining, open reduction internal fixation was chosen as the treatment option for the patient over arthroplasty. The patient was positioned supine on a standard fracture table with the non-operative leg in lithotomy position and C-arm on the contralateral side.
Due to the patient’s prior history of independence, he was counseled and surgical repair was recommended. Due to the length of the residual limb, the difficulty to manipulate it for proper dislocation and reduction, and the lack of appropriately sized implants for the length of femur remaining, open reduction internal fixation was chosen as the treatment option for the patient over arthroplasty. The patient was positioned supine on a standard fracture table with the non-operative leg in lithotomy position and C-arm on the contralateral side. To obtain proper reduction in the operative leg, a traction pin was placed in the distal femoral shaft paying careful attention to avoid any vascular structures (Fig. 3-8). A Kirschner bow was applied to the wire and a rope was attached and wrapped around the boot of the fracture table on the right side. Traction, rotation, and adduction were then applied under fluoroscopic guidance until appropriate reduction was obtained. A standard femoral neck system technique was then utilized for dissection and final implant insertion (Fig. 7, 8).
To obtain proper reduction in the operative leg, a traction pin was placed in the distal femoral shaft paying careful attention to avoid any vascular structures (Fig. 3-8). A Kirschner bow was applied to the wire and a rope was attached and wrapped around the boot of the fracture table on the right side. Traction, rotation, and adduction were then applied under fluoroscopic guidance until appropriate reduction was obtained. A standard femoral neck system technique was then utilized for dissection and final implant insertion (Fig. 7, 8). 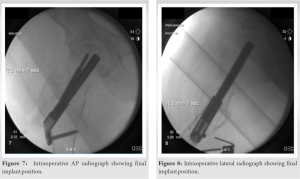 The wound was closed in layers and the patient had an uneventful post-operative course. Due to the proximity of the incision to where the patient’s prosthesis would be, he was made non-weight bearing until the incision had healed. Physical and Occupational Therapy was started on post-operative day 1 and the patient was discharged home on post-operative day 5 to a skilled nursing facility due to a lack of assistance at home. The patients’ first post-operative clinic visit was at 2 weeks after the operation. Radiographs were taken showing adequate placement of the FNS with appropriate initial healing. The incision was deemed to be healed, so staples were removed, and he was allowed to progress weight bearing to toe-touch until the subsequent visit in 6 weeks. At the next clinic visit, 2 months since the surgery, radiographs showed great alignment of the fracture without any changes. The patient was transitioned to weight bearing as tolerated and scheduled for follow-up in an additional 6 weeks. During the subsequent visit, the patient had been ambulating with the assistance of crutches. He reported that his pain was 0/10 and that he had not been taking any medications for pain and/or inflammation. Imaging was taken with his prosthesis in place that showed well healing fracture with intact instrumentation without evidence of failure or loosening. He was instructed to follow-up in 2 months. Six months after the surgery, the patient reported that he continued to do well. He presented with no complaints of pain or discomfort in his right hip, and he has continued to ambulate without difficulty. He had returned to his normal activities without any limitations. One year after the injury, the patient progressed well and reported no issues, complaints, or concerns with his hip.
The wound was closed in layers and the patient had an uneventful post-operative course. Due to the proximity of the incision to where the patient’s prosthesis would be, he was made non-weight bearing until the incision had healed. Physical and Occupational Therapy was started on post-operative day 1 and the patient was discharged home on post-operative day 5 to a skilled nursing facility due to a lack of assistance at home. The patients’ first post-operative clinic visit was at 2 weeks after the operation. Radiographs were taken showing adequate placement of the FNS with appropriate initial healing. The incision was deemed to be healed, so staples were removed, and he was allowed to progress weight bearing to toe-touch until the subsequent visit in 6 weeks. At the next clinic visit, 2 months since the surgery, radiographs showed great alignment of the fracture without any changes. The patient was transitioned to weight bearing as tolerated and scheduled for follow-up in an additional 6 weeks. During the subsequent visit, the patient had been ambulating with the assistance of crutches. He reported that his pain was 0/10 and that he had not been taking any medications for pain and/or inflammation. Imaging was taken with his prosthesis in place that showed well healing fracture with intact instrumentation without evidence of failure or loosening. He was instructed to follow-up in 2 months. Six months after the surgery, the patient reported that he continued to do well. He presented with no complaints of pain or discomfort in his right hip, and he has continued to ambulate without difficulty. He had returned to his normal activities without any limitations. One year after the injury, the patient progressed well and reported no issues, complaints, or concerns with his hip.
We present an atypical case of a femoral neck fracture in a patient with a history of a previous transfemoral amputation. Femoral neck fractures are common injuries in the United States with about 1.6 million occurring annually [3] While femoral neck fractures present as a common orthopedic injury most orthopedic surgeons encounter, femur fractures in amputees are an uncommon occurrence [4]. A thorough pre-operative evaluation including a detailed history, physical examination, and imaging should be completed. For most femoral neck fractures, radiographs may be enough for pre-operative planning. However, if needed, advanced imaging may also be conducted. When deciding on an operative plan, various factors such as the degree of fracture displacement and patient physical age/physiologic age, impact selection of different treatment options ranging from percutaneous screw fixation to open reduction internal fixation, and arthroplasty [5]. Occasionally, there are accentuating circumstances that may lead the surgeon toward one method of fixation over another. If a patient has had a previous limb amputation, whether it is transtibial or transfemoral, may impact final implants/fixation methods chosen. As one of the primary goals of femoral neck fracture management in previously ambulatory patients is to mobilize as early as possible to prevent complications such as deep vein thrombosis, pneumonia, and decubitus ulcers, arthroplasty (total versus hemiarthroplasty) is often chosen as the definitive fixation. However, depending on the size of the lever arm the residual limb provides for reduction, this may prove to be challenging [6]. Furthermore, the standard lengths of the arthroplasty implants may not be made short enough to fit in the residual femur. When minimal extremity rotation is required for fracture reduction, the technique used for our patient can be applied. Berg et al. described a similar technique in bilateral below knee amputees using a fracture table with skeletal traction and fixation with sliding hip screw [7]. Alternatively, Aqil et al. described that in situ fixation without traction/reduction can be done as well [8]. The Femoral Neck System (FNS) is a relatively novel method in treating femoral neck fractures. It has previously been studied as being superior to cannulated screws and comparable to sliding hip screws [9]. Furthermore, Jian-Xiong Ma et al. showed that fixed angle constructs such as the sliding hip screw had fewer post-operative complications and faster union rates when compared to cannulated screws [10]. The minimally invasive incision and ability to weight bear patients early with the FNS can be argued as an advantage found similarly in other femoral neck treatment options. In situations such as in this case report, where the length of the residual limb could not be justified in being used for dislocation and reduction of the hip for an arthroplasty, the FNS provided an alternative solution with similar benefits.
Our case highlights a novel method for treating femoral neck fractures when the lever arm is minimal and the residual limb is too short for arthroplasty. Our decision to proceed with the femoral neck system was based on studies showing increased mechanical stability of FNS and fixed angle devices over percutaneous screws and the desire to minimize potential reoperation if the screws were to fail. This case highlights one of the many successful ways to treat femoral neck fractures in amputees when proper preparation, knowledge of principles, and equipment are used.
Treating femoral neck fractures in above knee amputee patients can be challenging. Surgical interventions ranging from open reduction internal fixation to arthroplasty can be considered. Detailed planning and unique patient positioning may be necessary to treat these individuals successfully.
References
- 1.Boussakri H, Alassaf I, Hamoudi S, Elibrahimi A, Ntarataz P, ELMrini A, et al. Hip arthroplasty in a patient with transfemoral amputation: A new tip. Case Rep Orthop 2015;2015:593747. [Google Scholar | PubMed]
- 2.Koval KJ, Friend KD, Aharonoff GB, Zukerman JD. Weight bearing after hip fracture: A prospective series of 596 geriatric hip fracture patients. J Orthop Trauma 1996;10:526-30. [Google Scholar | PubMed]
- 3.Kazley J. Femoral Neck Fractures. Treasure Island (FL): StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537347 [Last accessed on 2020 Oct 10]. [Google Scholar | PubMed]
- 4.Mirdad T, Khan MR, Kazarah Y. Fracture of the femur in amputation stumps. Ann Saudi Med 1997;17:638-40. [Google Scholar | PubMed]
- 5.Lutnick E, Kang J, Freccero DM. Surgical treatment of femoral neck fractures: A brief review. Geriatrics (Basel) 2020;5:22. [Google Scholar | PubMed]
- 6.Ma C, Lv Q, Yi C, Ma J, Zhu L. Ipsilateral total hip arthroplasty in patient with an above-knee amputee for femoral neck fracture: A case report. Int J Clin Exp Med 2015;8:2279-83. [Google Scholar | PubMed]
- 7.Berg AJ, Bhatia C. Neck of femur fracture fixation in a bilateral amputee: An uncommon condition requiring an improvised fracture table positioning technique. BMJ Case Rep 2014;2014:bcr2013203504. [Google Scholar | PubMed]
- 8.Aqil A, Desai A, Dramis A, Hossain S. A simple technique to position patients with bilateral above-knee amputations for operative fixation of intertrochanteric fractures of the femur: A case report. J Med Case Rep 2010;4:390. [Google Scholar | PubMed]
- 9.Stoffel K, Zderic I, Gras F, Sommer C, Eberli U, Mueller D, et al. Biomechanical evaluation of the femoral neck system in unstable Pauwels III femoral neck fractures: A comparison with the dynamic hip screw and cannulated screws. J Orthop Trauma 2017;31:131-7. [Google Scholar | PubMed]
- 10.Ma JX, Kuang MJ, Xing F, Zhao YL, Chen HT, Zhang LK, et al. Sliding hip screw versus cannulated cancellous screws for fixation of femoral neck fracture in adults: A systematic review. Int J Surg 2018;52:89-97. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report
July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System September 1, 2025 Failure of the Femoral Neck System in a Young Patient: A Case Report
September 1, 2025 Failure of the Femoral Neck System in a Young Patient: A Case Report February 10, 2024 Peri-Implant Fracture Following Prior Fixation of Femoral Neck Fracture Using the Femoral Neck System: A Case Report
February 10, 2024 Peri-Implant Fracture Following Prior Fixation of Femoral Neck Fracture Using the Femoral Neck System: A Case Report