
Augmenting the femoral neck system with two additional cannulated cancellous screws provides enhanced rotational stability and favourable clinical outcomes in unstable femoral neck fractures.
Dr Shreeram Jayant Gokhale, Department of Orthopaedics, Dr D. Y. Patil Medical College and Hospital, Nerul, Navi Mumbai, Maharashtra, India. E-mail: gokhaleshreeram@gmail.com
Abstract
Introduction: Femoral neck fractures in young adults require urgent anatomical reduction and stable fixation to preserve the native femoral head and prevent complications, such as avascular necrosis and non-union. The femoral neck system (FNS) provides angular stability, but its effectiveness may be limited in vertically orientated unstable fractures.
Case Report: We report a case of a 42-year-old male with a Pauwels type III femoral neck fracture managed using a hybrid construct consisting of the FNS augmented with two additional cannulated cancellous screws. The patient underwent surgery within 15 h of injury following pre-anaesthetic evaluation. Anatomical reduction and stable fixation were achieved. Progressive fracture healing was observed with complete union at 3 months and an excellent functional outcome.
Conclusion: Augmenting the FNS with additional cannulated cancellous screws enhances rotational stability and may improve outcomes in unstable vertical femoral neck fractures.
Keywords: Femoral neck fracture, femoral neck system, cannulated cancellous screws, Pauwels type III, augmented fixation.
Femoral neck fractures in young adults are high-energy injuries that continue to pose significant challenges to orthopaedic surgeons. Unlike elderly patients in whom arthroplasty is commonly preferred, preservation of the native femoral head remains the primary goal in younger individuals because of their higher functional demands and longer life expectancy. These fractures are associated with serious complications, such as avascular necrosis (AVN), non-union, fixation failure, femoral neck shortening, and post-traumatic osteoarthritis. Failure rates following internal fixation have been reported between 7% and 22% due to these complications [1,2,3]. The vascular anatomy of the femoral head makes femoral neck fractures particularly time-sensitive injuries. Displacement of the fracture can compromise the retinacular vessels supplying the femoral head, thereby increasing the risk of AVN. Several studies have emphasised the importance of early surgical intervention, preferably within 24 h of injury, to minimise vascular compromise and improve outcomes. In addition to early surgery, anatomical reduction is considered one of the most important prognostic factors influencing fracture union and femoral head survival. Inadequate reduction can lead to persistent shear forces, rotational instability, altered hip biomechanics, and eventual fixation failure. Pauwels type III femoral neck fractures are especially unstable because of their vertical orientation, which subjects the fracture to high shear stress rather than compressive forces. Stable fixation in these fractures remains technically demanding. The femoral neck system (FNS) was developed to provide angular stability through a minimally invasive approach with improved biomechanical characteristics compared with multiple cancellous screws alone [4,5,6]. Recent systematic reviews and comparative studies have demonstrated favourable clinical outcomes and improved stability with FNS compared with conventional cannulated cancellous screw fixation [5,7,8,9,10]. However, in highly vertical fracture patterns, rotational and shear instability may still persist despite standard FNS fixation [4,8,9]. We present a case of an unstable Pauwels type III femoral neck fracture in a young adult managed using a hybrid construct consisting of the FNS augmented with two additional cannulated cancellous screws to improve rotational and axial stability.
A 42-year-old male presented with severe pain in the right hip following a road traffic accident. The patient had no other associated injuries and no significant medical comorbidities, such as diabetes mellitus, hypertension, asthma, hyperlipidaemia, or ischaemic heart disease. On clinical examination, the right lower limb was positioned in flexion, abduction, and external rotation with localised tenderness over the right hip region. Painful restriction of hip movements was present. Radiographs revealed a Pauwels type III fracture of the right femoral neck (Figs. 1 and 2).

Figure 1: Pre-operative pelvis with both hips anteroposterior radiograph.

Figure 2: Pre-operative right hip anteroposterior radiograph showing a Pauwels type III fracture of the right femoral neck.
Considering the patient’s young age, vertical fracture configuration, and need for preservation of the femoral head, urgent surgical fixation was planned. The patient underwent surgery within 15 h of injury following routine investigations and pre-anaesthetic evaluation.
Surgical technique:
The surgery was performed under spinal anaesthesia with the patient positioned supine on a fracture table. The affected limb was placed in gentle traction with slight internal rotation, while the contralateral limb was abducted to facilitate fluoroscopic visualisation in both anteroposterior and lateral views. Closed reduction was achieved under image intensifier guidance using traction, internal rotation, and slight adduction. Anatomical reduction was confirmed fluoroscopically before fixation. A standard lateral proximal femoral incision was made. The FNS (Synthesiser) was inserted according to the manufacturer’s technique. A K-wire was passed, avoiding the future path of the FNS guidewire, to temporarily stabilise the fracture during reaming. A central guidewire was placed in the femoral neck and head under fluoroscopic guidance. After appropriate reaming, a single-hole FNS plate with a 90 mm bolt and a bicortical distal locking screw was used for plate fixation. In the end, an anti-rotation screw was inserted. Due to the vertical orientation and unstable nature of the Pauwels type III fracture, augmentation with two additional 6.5 mm × 85 mm partially threaded cannulated cancellous screws was performed to improve rotational and axial stability. Both screws were inserted superior to the FNS construct. One screw was placed anteriorly and the other posteriorly in parallel configuration under fluoroscopic guidance while maintaining adequate screw spread within the femoral head. Final fluoroscopic images confirmed satisfactory fracture reduction, restoration of neck-shaft alignment, appropriate implant positioning, and adequate tip-apex distance (Figs. 3 and 4). Thorough saline wash was given, and the wound was closed in layers.

Figure 3: Intraoperative fluoroscopic images showing insertion of the femoral neck system.
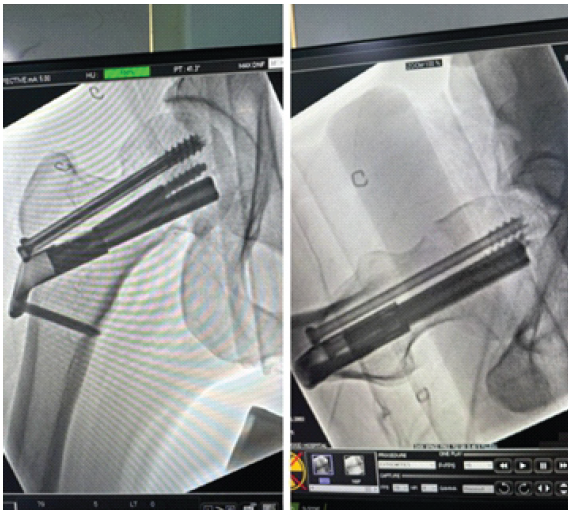
Figure 4: Final intraoperative fluoroscopic images showing augmentation with two cannulated cancellous screws.
The post-operative period was uneventful. The patient experienced satisfactory pain relief with a gradual reduction in Visual Analogue Scale (VAS) scores during follow-up. The surgical wound healed well without infection or wound complications. Static quadriceps exercises and ankle pump exercises were initiated on the 1st post-operative day. Gradual hip and knee range-of-motion exercises were started as tolerated. The patient was mobilised initially with non-weight-bearing ambulation using a walker, followed by partial weight-bearing at 6 weeks and progression to full weight-bearing after radiological evidence of union. Follow-up evaluations were performed at 15 days, 1 month, and 3 months. Radiographs demonstrated maintained reduction, satisfactory implant positioning, and progressive fracture healing. The blade, anti-rotation screw, and additional cannulated cancellous screws were appropriately positioned with adequate tip-apex distance, and the bicortical distal locking screw remained stable (Figs. 5 and 6).
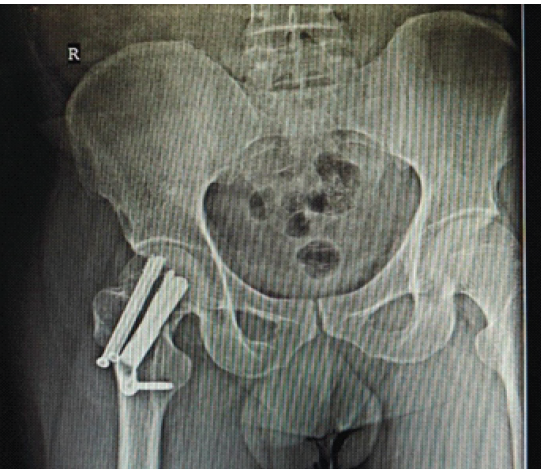
Figure 5: Post-operative pelvis with both hips anteroposterior radiograph showing satisfactory implant positioning and fracture reduction.
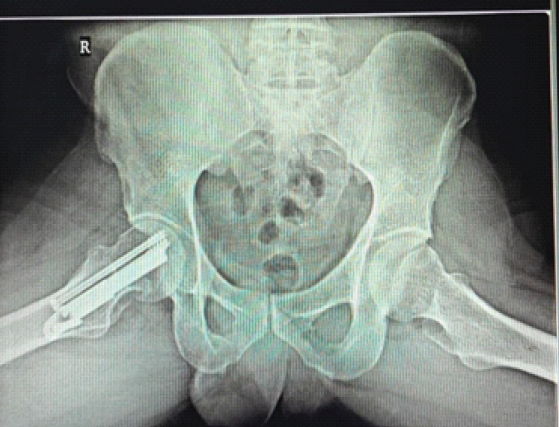
Figure 6: Post-operative pelvis with both hips, frog-leg lateral radiograph showing progressive fracture union and stability.
At the 3-month follow-up, radiographs demonstrated complete bony union. The patient regained a painless, full range of hip movements with excellent functional recovery (Fig. 7). The Harris Hip Score improved progressively from 65 at 15 days to 95 at 3 months, while the VAS score improved from 6 to 0 (Table 1) [11].

Figure 7: Clinical photographs showing full functional recovery at 3-month follow-up.
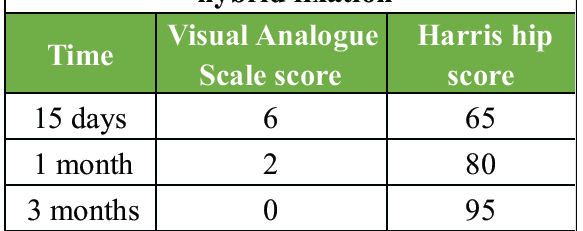
Table 1: Functional outcomes following hybrid fixation
The favourable outcome could be attributed to early surgical intervention, anatomical reduction, ideal implant positioning, and augmentation of the FNS with two additional cannulated cancellous screws despite the unstable fracture configuration.
Femoral neck fractures with vertical orientation are subjected to high shear forces, increasing the risk of displacement, fixation failure, and non-union [3,4]. Management of these fractures in young adults remains challenging because preservation of the femoral head is of paramount importance. Several studies have demonstrated that delay in surgery is associated with increased incidence of AVN due to prolonged compromise of femoral head vascularity [1,2]. Therefore, early surgical intervention combined with anatomical reduction remains the cornerstone of treatment. The quality of reduction has been consistently shown to influence both fracture union and long-term functional outcomes. Residual varus malalignment or rotational instability increases stress across the fracture site and predisposes to fixation failure. The FNS provides angular stability and controlled dynamic compression through a minimally invasive approach and has shown promising biomechanical and clinical outcomes compared with conventional cannulated cancellous screws [1,4,10]. However, in highly vertical Pauwels type III fractures, the standard FNS construct alone may not adequately neutralise rotational and shear forces. Biomechanical studies have suggested that augmentation with additional cannulated cancellous screws improves construct stiffness, enhances rotational control, and distributes load more effectively across the fracture site [6,8]. In addition, recent reports have highlighted potential limitations and complications associated with standalone FNS fixation in certain unstable fracture patterns, further supporting the rationale for augmentation in selected cases [12]. In the present case, the use of two additional 6.5 mm cannulated cancellous screws along with FNS provided enhanced stability without compromising the minimally invasive nature of the procedure. Early fixation within 15 h of injury, accurate anatomical reduction, and stable fixation contributed to successful fracture union and excellent functional recovery in our patient. This case highlights that augmentation of the FNS with additional cancellous screws may be a valuable option in managing unstable vertical femoral neck fractures in young adults.
Augmentation of the FNS with additional cannulated cancellous screws provides improved rotational and axial stability in unstable femoral neck fractures. This technique is simple, minimally invasive, and effective in achieving early union and excellent functional outcomes.
Augmenting the femoral neck system with additional cannulated cancellous screws improves rotational stability and is a reliable technique for managing unstable Pauwels type III femoral neck fractures in young adults.
References
- 1. Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury 2015;46:484-91. [Google Scholar] [PubMed]
- 2. Florschutz AV, Langford JR, Haidukewych GJ, Koval KJ. Femoral neck fractures: Current management. J Orthop Trauma 2015;29:121-9. [Google Scholar] [PubMed]
- 3. Panteli M, Rodham P, Giannoudis PV. Biomechanical rationale for fixation choices. Injury 2015;46:445-52. [Google Scholar] [PubMed]
- 4. Stoffel K, Zderic I, Gras F, Sommer C, Eberli U, Mueller D, et al. Biomechanical evaluation of the femoral neck system in unstable Pauwels III femoral neck fractures. J Orthop Trauma 2017;31:131-7. [Google Scholar] [PubMed]
- 5. Hu H, Cheng J, Feng M, Gao Z, Wu J, Lu S, et al. Clinical outcome of FNS vs cannulated screws. J Orthop Surg Res 2021;16:370. [Google Scholar] [PubMed]
- 6. Schopper C, Zderic I, Menze J, Müller D, Rocci M, Knobe M. Stability of FNS vs pins. J Orthop Transl 2020;24:88-95. [Google Scholar] [PubMed]
- 7. Lu Y, Huang Z, Xu Y, Huang Q, Ren C, Li M, et al. Femoral neck system versus cannulated screws for fixation of femoral neck fracture in young adults: A systematic review and meta-analysis. Am J Transl Res 2022;15:5480-90. [Google Scholar] [PubMed]
- 8. Tang Y, Zhang Z, Wang L, Xiong W, Fang Q, Wang G. FNS vs cannulated screws: a comparative study. J Orthop Surg Res 2021;16:504. [Google Scholar] [PubMed]
- 9. Zhou XQ, Li ZQ, Xu RJ, She YS, Zhang XX, Chen GX, et al. Early clinical results of FNS vs screws. Orthop Surg 2021;13:1802-9. [Google Scholar] [PubMed]
- 10. Vatkar AJ, Kale S, Kanade G, Godke A, Dey JK, Godke R, et al. FNS vs CCS in the Indian population. J Clin Orthop 2023;8:16-20. [Google Scholar] [PubMed]
- 11. Nilsdotter A, Bremander A. Measures of hip function and symptoms: Harris hip score (HHS), hip disability and osteoarthritis outcome score (HOOS), Oxford hip score (OHS), Lequesne index of severity for osteoarthritis of the hip (LISOH), and American Academy of Orthopaedic Surgeons (AAOS) hip and knee questionnaire. Arthritis Care Res (Hoboken) 2011;63:S200-7. [Google Scholar] [PubMed]
- 12. Kale S, Chalak A, Vatkar A, Dey JK, Mehta N, Das S. Limitations and complications in treating femoral neck fractures with the femoral neck system: A case report. J Orthop Case Rep 2024;14:78-82. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System
December 1, 2025 From Valgus-impacted to Displaced: Clinical and Technical Lessons in Femoral Neck Fracture Fixation with the Femoral Neck System September 1, 2025 Failure of the Femoral Neck System in a Young Patient: A Case Report
September 1, 2025 Failure of the Femoral Neck System in a Young Patient: A Case Report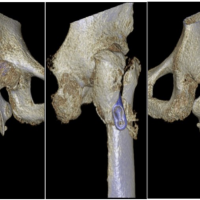 February 10, 2024 Peri-Implant Fracture Following Prior Fixation of Femoral Neck Fracture Using the Femoral Neck System: A Case Report
February 10, 2024 Peri-Implant Fracture Following Prior Fixation of Femoral Neck Fracture Using the Femoral Neck System: A Case Report August 10, 2022 Management of Femoral Neck Fracture in Above Knee Amputee with Femoral Neck System: A Case Report
August 10, 2022 Management of Femoral Neck Fracture in Above Knee Amputee with Femoral Neck System: A Case Report