
Limb lengthening, distraction or traction on a limb in a child can cause an increase in blood pressure leading to hypertension for a variable period. Hence, children’s blood pressure should be monitored perioperatively.
Dr. Nareshkumar Satyanarayan Dhaniwala, Department of Orthopedics, Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical sciences (Deemed to be University), Sawangi, Wardha, India. E-mail: nsdhaniwala@gmail.com
Introduction: Congenital pseudarthrosis of tibia is an uncommon condition leading to gradually progressive deformity, shortening of the limb and disability. The condition is notorious for failure of treatment and need of multiple operations. A combination of open reduction, thorough excision of abnormal tissue at the pseudarthrosis site, intramedullary nailing, ring fixator application, and distraction to achieve bone equalization has proved successful.
Case Report: A case of congenital pseudarthrosis of the left tibia and fibula associated with neurofibromatosis treated by open reduction, intramedullary nailing, ring fixator application, and distraction at corticotomy to cause compression at the pseudarthrosis site and limb length equalization is being reported due to uncommon occurrence of transient hypertension in the child as a complication of ring fixator.
Conclusion: Transient hypertension is a rare complication seen in children after application of ring fixator. Its diagnosis and control require proper perioperative assessment of child regarding blood pressure (BP), monitoring of BP during distraction period and period of application of ring fixator, and its treatment under care of pediatrician.
Keywords: Congenital, pseudarthrosis, tibia, ring fixator, corticotomy, distraction, transient hypertension.
In pediatric orthopedic surgery, congenital pseudoarthrosis of tibia (CPT) continues to be one of the arduous issues of management [1]. Pseudo means false, and arthrosis is the formation of a joint. CPT is an uncommon congenital anomaly. Pseudarthrosis is reported in clavicle, fibula, femur and tibia, the most common being in tibia and fibula. In tibia, it occurs 1 in every 190,000 live births [2]. It is distinguished by de-ossification, bending as well as pathological fracture, which is followed by an inability to form a normal callus at the fracture site [3]. Pseudoarthrosis in general is assoc iated with neurofibromatosis-1 (NF-1) in 55% of cases. Pseudoarthrosis of tibia is reported in 6% of NF-1 patients [1]. Prophylactic intramedullary nailing before the fracture in the lesion, on-lay and in-lay bone grafting with fixation, vascularized fibular bone graft and the ilizarov external ring fixation with distraction osteogenesis across corticotomy are a few surgical options of treatment. In all these procedures, the excision of the abnormal hamartomatous tissue at the pseudarthrosis site is the primary and essential step in the treatment. Success of surgical treatment is uncertain in this entity and repeated surgeries in the form of revised fixation and bone grafting from autologous and synthetic sources are commonly needed. Some orthopedic procedures in children such as limb lengthening operation, too rapid bone lengthening particularly in tibia and femur have been reported to cause hypertension [4]. Children normally do not suffer from primary or secondary hypertension but hypertension has been reported following few orthopedic surgeries in children. There are reports of children developing transient hypertension following application of ring external fixator also. Herein a case of congenital pseudarthrosis of tibia and fibula in an 18 months old child is reported who had developed hypertension during the treatment with ring fixator.
The parents of an 18-month-old boy presented to the orthopedic outpatient department with complaints of substantial left leg shortening in the child for 8 months, deformity and inability to walk normally. The baby was delivered by caesarean section at full term due to breech presentation. His milestones of development were appropriate for the age. The child did not have anyother complaints. The patient’s mother had multiple nodular lesions of neurofibromatosis since her childhood over her face and hand. The father and uncle of the child’s mother also had similar lesions on their arms. The parents noticed a bending deformity in the left leg a few months after birth. This deformity allegedly increased after the fall from cot 8 months back. The patient was treated by repeated plaster cast for 4 months without any improvement in his condition. This delayed his standing and walking and led to progressive shorting in the left lower limb. On general examination, the child was healthy looking, afebrile, with a pulse of 96 beats per minute and blood pressure (BP) of 90/60 mmHg, with no pallor, no icterus, or clubbing. There were multiple café au lait spots on the front and back of trunk (Fig. 1). The left leg had bony deformity in the lower third with anterior convexity, with typical features of pseudarthrosis tibia and fibula along with gross abnormal mobility and 1.5 cm shortening. The right leg was normal. An X-ray of the left leg revealed bony discontinuity in both the tibia and fibula at lower thirds shaft with narrowing and sclerosis of bone ends at the pseudarthrosis site. Pseudarthrosis in fibula was at a lower level then pseudarthrosis in tibia. There is no evidence of any new bone formation at both the non-union sites (Fig. 2). The treatment included open excision of abnormal fibrous tissue from the pseudarthrosis site of tibia and freshening of bone ends to achieve bleeding bone ends with good contact. Intra medullary splintage of the tibia was done using a titanium elastic nail (TENS) passed from proximal end of the tibia to the lower metaphysis across the pseudarthrosis site and placement of synthetic bone graft granules at the pseudarthrosis site. Immobilization of the leg was done using ring fixator. Corticotomy was done carefully between the proximally placed first and second ring. Third and fourth rings stabilized the lower tibial segment. Three rings were stabilized with two illizarov wires and third ring from top remained without any wire. The assembly had four connecting rods and each ring was made up of two half rings. No intervention was done for fibula (Fig. 3). Distraction was started at the rate of 0.5 mm per 12 hourly 8 days after surgery.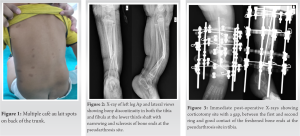 It was continued for fifteen days, and then compression was done for 5 days. Distraction was further continued till the limb length got equalized and there was good contact of the freshened bone ends at the pseudarthrosis site. This took around 6 weeks of continuous distraction. The ring fixators were kept for further 1 month during which there was reasonable consolidation of regenerate at the distracted corticotomy site (Fig. 4). The fixator had to be removed earlier because the gap between posterior part of ring and calf had decreased due to persistent edema and swelling in the leg. The limb was immobilized in above knee cast and child continuous to remain under follow-up. Preoperatively complete blood count (Hb 11.7 gm / dl , WBC 11,500/ml, and platelet count 3.27 lacs) and KFT (urea 7 mg/dl, creatinine 0.2 mg/dl, sodium 135 mmol/l, and potassium 4.5 mmol/l) were within normal limits. During surgery the anesthetist noted abnormal rise in BP of the child. Injectable labetalol was used to control it. Postoperatively the child was shifted to pediatric intensive care unit where he was treated and investigated regarding the cause of hypertension. Postoperatively his Hb decreased to 7.8 gm/dl, WBC 11,200/ml and platelet count were 2.91 lacs. KFT values were normal limits. Ultrasound scan of abdomen and pelvis ruled out any kidney or supra renal mass. Doppler study to detect renal artery stenosis did not show any abnormality.
It was continued for fifteen days, and then compression was done for 5 days. Distraction was further continued till the limb length got equalized and there was good contact of the freshened bone ends at the pseudarthrosis site. This took around 6 weeks of continuous distraction. The ring fixators were kept for further 1 month during which there was reasonable consolidation of regenerate at the distracted corticotomy site (Fig. 4). The fixator had to be removed earlier because the gap between posterior part of ring and calf had decreased due to persistent edema and swelling in the leg. The limb was immobilized in above knee cast and child continuous to remain under follow-up. Preoperatively complete blood count (Hb 11.7 gm / dl , WBC 11,500/ml, and platelet count 3.27 lacs) and KFT (urea 7 mg/dl, creatinine 0.2 mg/dl, sodium 135 mmol/l, and potassium 4.5 mmol/l) were within normal limits. During surgery the anesthetist noted abnormal rise in BP of the child. Injectable labetalol was used to control it. Postoperatively the child was shifted to pediatric intensive care unit where he was treated and investigated regarding the cause of hypertension. Postoperatively his Hb decreased to 7.8 gm/dl, WBC 11,200/ml and platelet count were 2.91 lacs. KFT values were normal limits. Ultrasound scan of abdomen and pelvis ruled out any kidney or supra renal mass. Doppler study to detect renal artery stenosis did not show any abnormality. Echocardiography ruled out any coarctation of aorta as well as left ventricular hypertrophy. The absence of any eye abnormalities including retinal changes excluded long standing hypertension. A 24-h urinary vanillylmandelicacid (VMA) was also normal, there by excluding neuroblastoma. Postoperatively, the child was put on tab Labetalol 1mg/kg/day after 1 day of BP observation. BP was 122/90 mm Hg. After 24 h BP was noted to be 118/98 mmHg and tab Amlodipine 0.1 mg/kg/day was added. BP did not settle with these doses so; tab Labetalol dose was increased from 1 mg/kg/day to 2 mg/kg/day after 2 days. 24 h later BP was 116/60 and tab Envas (Enalapril) 0.1 mg/kg/day was added as the third drug. Tab clonidine was added further in the dose of 5 ug/kg/day after next 24 h observation. After 2 weeks at the time of discharge, the child was taking four drugs and the dose of clonidine was increased from 5 to 6 ug/kg/day. Regular follow-up was done further and anti-hypertension drugs were reduced from four to two drugs after a month. The drugs were stopped totally after further 1 month. This period roughly coincided the period of distraction at the corticotomy site. Stoppage of distraction resulted in normalization of BP.
Echocardiography ruled out any coarctation of aorta as well as left ventricular hypertrophy. The absence of any eye abnormalities including retinal changes excluded long standing hypertension. A 24-h urinary vanillylmandelicacid (VMA) was also normal, there by excluding neuroblastoma. Postoperatively, the child was put on tab Labetalol 1mg/kg/day after 1 day of BP observation. BP was 122/90 mm Hg. After 24 h BP was noted to be 118/98 mmHg and tab Amlodipine 0.1 mg/kg/day was added. BP did not settle with these doses so; tab Labetalol dose was increased from 1 mg/kg/day to 2 mg/kg/day after 2 days. 24 h later BP was 116/60 and tab Envas (Enalapril) 0.1 mg/kg/day was added as the third drug. Tab clonidine was added further in the dose of 5 ug/kg/day after next 24 h observation. After 2 weeks at the time of discharge, the child was taking four drugs and the dose of clonidine was increased from 5 to 6 ug/kg/day. Regular follow-up was done further and anti-hypertension drugs were reduced from four to two drugs after a month. The drugs were stopped totally after further 1 month. This period roughly coincided the period of distraction at the corticotomy site. Stoppage of distraction resulted in normalization of BP.
For the treatment of CPT, vascularized fibular grafting, intramedullary stabilization, and external fixation are now being employed with varying degrees of effectiveness [5]. It is challenging to evaluate the results of treatment in various types of pseudoarthrosis, the effects of prior treatment, the requirement for follow-up till skeletal maturity, the timing of the surgery, and the definition of what is a successful result. The ilizarov circular external fixator has been used to treat CPT by a number of authors [6]. It concurrently addresses a number of features of the problem, including as pseudarthrosis resection, deformity repair, shortening correction, infection control, articular function, weight bearing, and valgus ankle correction. The duration of treatment, pin tract infections, ankle valgus, and refracture are the drawbacks of this procedure. The first western surgeons to report successful circular external fixation for CPT were Paley et al. [5]. With one treatment, their series of 16 patients had a union rate of 94% and with two treatments, a union rate of 100%. In newborn and young children, hypertension is often a secondary phenomenon, with a renal etiology accounting for 75–80% of occurrences. The prevalence of acute and temporary hypertension in children who are in traction or cast has been noted by Loggie et al. [7]. Following a variety of orthopedic surgeries, particularly those that involve extending or lengthening the limbs, stretching the contracted tissues over a long period, hypertension in children has been described. The first to describe its incidence following femoral lengthening were Wilk and Badgley, who also advised adding hypertension to the already extensive list of problems associated with limb lengthening [8]. It is rarely documented in the past that external fixators and limb lengthening procedures might cause hypertension. It has been proposed that hypertension develops as a result of the sciatic nerve being stretched during limb-lengthening procedures, which may result in reflex vasoconstriction. With regard to circular external fixators, hypertension might result from nerve irritation caused on by a change in the limb’s microenvironment, which would then cause reflex vasoconstriction and hypertension [9]. Yosipovitch and Palh, and subsequently Whitehill and Hakala, theorized that the rise in BP after stretching was caused by a reflex reaction to tension that built up in the sciatic nerve in the upper thigh, which led to a vasoconstrictor response [10, 11]. In a study conducted to assess the relationship between hypertension and external fixators, 12.2% (5/41) of cases had stage 2 hypertension while using an external fixator [12]. Akbarnia et al. found that children between the ages of 2 and 3 experienced a 5% overall incidence of severe hypertension complicating posteromedial release and casting for club foot surgery [13]. The reported case did not have hypertension before surgery and was given fitness by pediatrician. During surgery the anesthetist noted the high BP and took the suitable measure to control it. The patient continued to have raised BP even after reversal from anesthesia and was treated by pediatrician and strict record of BP was maintained. Finding the blood pressure continuously high, he was investigated to find out its cause. Investigations such as 24-h urinary VMA, Doppler study, echocardiography, ultrasound scan of abdomen, and pelvis were found within normal limits. Distraction at the corticotomy site was started 8 days after surgery and continued for about 1.5 months. The patient was kept indoor till control of blood pressure which in this case required four drugs. The patient was under regular follow-up of pediatrician and drugs were gradually reduced in number every fortnight and stopped about 2 weeks after stoppage of distraction. The fixator was planned to be continued till regenerate consolidation but was removed earlier as there was hardly any space remaining between the calf and proximal two rings. There was sufficient density of regenerate and the limb length had become equalized with good contact at the freshened pseudarthrosis site. The limb was immobilized in above knee cast and the child continues to be under follow-up. The intramedullary TENS is retained to keep the tibia aligned and guide the growth of the bone. The blood pressure was found normal at the time of admission for ring removal. It was again noted to be raised during surgery and the child was put on tab amlodipine 2.5 mg per day. The detection of hypertension on operation table and its continuance till distraction at the corticotomy site in tibia in absence of any primary hypertension or any known cause of secondary hypertension in the child indicates that the child had transient hypertension related to the surgery and distraction done in tibia. The child suffered transient hypertension as a complication of ring fixator application and corticotomy. Similar cases have been reported by many authors [9, 12, 14]. In the case described by Manamperi et al., the blood pressure normalized 4 weeks after the surgery. Changulai et al. have described hypertension as a complication of Taylor spatial frame in a child where fixator removal normalized the blood pressure. In our case, the hypertension required four drugs for proper control which were continued till distraction was done. Drugs were reduced from four to two after a month and were discontinued after stoppage of distraction due to normal readings of blood pressure. The child had normal blood pressure on admission for fixator removal. But he had a few readings of high blood pressure after fixator removal also and has been a kept under observation regarding recurrence of hypertension. The events indicate a relation between ring fixator on the limb, corticotomy surgery and hypertension in the child. Corticotomy distraction also may be a factor in the rise of blood pressure. Thus, surgery of ring fixator application, corticotomy, and distraction at the corticotomy site seem to be contributing to the development of transient hypertension in the child. There is a need of further studies on similar cases to know its exact correlation.
The case report highlights the occurrence of transient hypertension as a complication of ring fixator application in a child of congenital pseudarthrosis of tibia and fibula.
Blood pressure assessment should be done as a perioperative measure in young children also, as many orthopedic procedures may precipitate secondary or transient hypertension in children.
References
- 1.Vander Have KL, Hensinger RN, Caird M, Johnston C, Farley FA. Congenital pseudarthrosis of the tibia. J Am Acad Orthop Surg 2008;16:228-36. [Google Scholar]
- 2.Pannier S. Congenital pseudarthrosis of the tibia. Orthop Traumatol Surg Res 2011;97:750-61. [Google Scholar]
- 3.Wellwood JM, Bulmer JH, Graff DJ. Congenital defects of the tibia in siblings with neurofibromatosis. J Bone Joint Surg Br 1971;53:314-9. [Google Scholar]
- 4.Linshaw MA, Stapleton FB, Gruskin AB, Baluarte HJ, Harbin GL. Traction-related hypertension in children. J Pediatr 1979;95:994-6. [Google Scholar]
- 5.Paley D, Catagni M, Argnani F, Prevot J, Bell D, Armstrong P. Treatment of congenital pseudoarthrosis of the tibia using the Ilizarov technique. Clin Orthop Relat Res 1992;280:81-93. [Google Scholar]
- 6.Grill F. Treatment of congenital pseudarthrosis of tibia with the circular frame technique. J Pediatr Orthop B 1996;5:6-16. [Google Scholar]
- 7.Loggie JM, New MI, Robson AM. Hypertension in the pediatric patient: A reappraisal. J Pediatr 1979;94:685-99. [Google Scholar]
- 8.Wilk LH, Badgley CE. Hy pertension, another complication of the leg-lengthening procedure. Report of a case. J Bone Joint Surg Am 1963;45:1263-8. [Google Scholar]
- 9.Changulani M, Bradbury M, Zenios M. Hypertension as a complication of Taylor spatial frame. J Pediatr Orthop B 2009;18:392-3. [Google Scholar]
- 10.Yosipovitch ZH, Palti Y. Alterations in blood pressure during leg-lengthening. A clinical and experimental investigation. J Bone Joint Surg Am 1967;49:1352-8. [Google Scholar]
- 11.Whitehill R, Hakala MW. The hypertension of femoral lengthening: A canine experimental model. Surg Forum 1976;27:525-6. [Google Scholar]
- 12.Oroko MD, Wadia FD, Farrell R, Bradbury M, Zenios M. Hypertension as a complication of circular external fixator. J Pediatr Orthop B 2013;22:270-4. [Google Scholar]
- 13.Akbarnia BA, Shapiro J, Ziaee M, Akbarnia NO. Hypertension after operative correction of club-foot deformity. J Bone Joint Surg Am l990;72:1330-3. [Google Scholar]
- 14.Manamperi MM, Tennakoon D, Sooriyapperuma T, Somaratne T, Abeysinghe C. Transient hypertension as a complication of circular external fixator-ilizarov frame. Sri Lanka J Child Health 2020;49:295-6. [Google Scholar]








