
Needle External fixator for phalanx fracture is a cheap and reasonably effective procedure.
Dr. Amrit Jha, Department of Orthopaedics, Fellowship in FIFA, Wrightington Hospital, Wigan, United Kingdom. E-mail: dramritjha@gmail.com
Introduction: Among all the phalanges, most fractured is the proximal phalanx. Frequently encountered complications are malunion, stiffness, and soft-tissue injury which invariably increase the disability. The aim of fracture reduction, therefore, comprises acceptable alignment and the gliding of the flexor and extensor tendons are maintained. Factors affecting management are fracture location, type of fracture, soft-tissue injury, and fracture stability.
Case Report: A 26-year-gentlemen, right hand dominant, a clerk by occupation, came to emergency with right-hand index finger pain, swelling, and unable to move the right index finger treated with debridement, wound wash, and external fixator frame made with K wire and needle cap. Fracture united in 6 weeks with good hand function and the full range of motion of the hand.
Conclusion: Mini fixator for phalanx fracture is a cheap and reasonably effective procedure. A needle cap fixator is a good alternative in difficult situations, it helps in correcting the deformity as well as keeps the joint surface distracted.
Keywords: Hand injury, open fracture, phalanx fracture
Metacarpals and phalanges are the most common hand fracture about 10%. The proximal phalanx of the fingers is most common fracture phalanx [1]. The deformity and displacement are typical when the proximal phalanx fracture involves the outer rays. Proximal phalanx fracture are usually stable and can be treated nonoperatively. The indication of surgery is angulation more than 20 in coronal view and >15° in sagittal view, <50% bone contact, rotational deformity, and collapse [2]. Proximal fragment is flexed due to interosseous muscle and lead to apex volar deformity [3]. Longitudinal compression force is given by flexor and extensor tendon that shortens the phalanx and distal fragment is extended. Close non-displaced and minimal displaced proximal phalanx fractures is managed nonoperatively. The goal of surgical treatment is to create a stable construct capable of withstanding gentle forces that are associated with an early range of motion. They include K wire, K wire and fixator, screw fixation, and anatomical plates.
26-year-old gentlemen, right-hand dominant, a clerk by occupation, came to emergency with right-hand index finger pain, swelling, and unable to move the right index finger. On examination, there was swelling, tenderness, and an ope wound over the dorsal aspect of the right hand’s second proximal phalanx. The extensor indices tendon was intact on clinical examination. All other systemic examination was normal. Plain radiograph right hand anteroposterior and oblique show a displaced extra-articular second proximal phalanx fracture (Fig. 1). 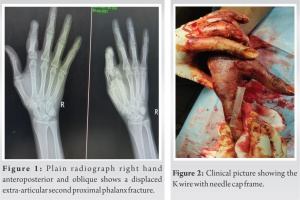 We discussed with the patient regarding surgery and rehabilitation. Written informed consent was taken for surgery. The patient was planned for a universal min external fixator. The patient was operated on under a local ring block with 2% of lignocaine without adrenaline. Unfortunately, due to miscommunication between operation theater staff, implant (fixator) was not available for surgery and the team was not aware of this. In this difficult situation, we thought of only debridement for now and postpone the fixation for the next theater list. We proceed with the debridement, extensor indices tendon was intact after the debridement fracture was unstable in length so at that moment, we thought of fixation. 1.2 mm diameter K wire one was passed parallel to the joint proximal to fracture and the second K wire was distal to fracture. The acceptable reduction was achieved in all planes and a sterile needle cap was pierced through one edge only, to avoid injury from exposed ends of K wires (Fig. 2) which act as mini fixator. A wound wash was given and the open wound was closed with ethilon 3–0 suture. The finger was immobilized for 2 weeks because we are concerned with the stability of fixation. The patient returned to work the very next day after surgery but advise to avoid heavy work. The patient was reviewed on 14 days for suture removal and finger motion was started to prevent stiffness with a needle cap fixator in situ. On 4-week follow-up, K wire is removed, and a plain radiograph was done. The patient was advised of active finger movement and further follow-up. Plain radiograph at six showing complete fracture union (Fig. 3).
We discussed with the patient regarding surgery and rehabilitation. Written informed consent was taken for surgery. The patient was planned for a universal min external fixator. The patient was operated on under a local ring block with 2% of lignocaine without adrenaline. Unfortunately, due to miscommunication between operation theater staff, implant (fixator) was not available for surgery and the team was not aware of this. In this difficult situation, we thought of only debridement for now and postpone the fixation for the next theater list. We proceed with the debridement, extensor indices tendon was intact after the debridement fracture was unstable in length so at that moment, we thought of fixation. 1.2 mm diameter K wire one was passed parallel to the joint proximal to fracture and the second K wire was distal to fracture. The acceptable reduction was achieved in all planes and a sterile needle cap was pierced through one edge only, to avoid injury from exposed ends of K wires (Fig. 2) which act as mini fixator. A wound wash was given and the open wound was closed with ethilon 3–0 suture. The finger was immobilized for 2 weeks because we are concerned with the stability of fixation. The patient returned to work the very next day after surgery but advise to avoid heavy work. The patient was reviewed on 14 days for suture removal and finger motion was started to prevent stiffness with a needle cap fixator in situ. On 4-week follow-up, K wire is removed, and a plain radiograph was done. The patient was advised of active finger movement and further follow-up. Plain radiograph at six showing complete fracture union (Fig. 3). We measure grip strength and pinch with a dynamometer which is 90 of normal strength to the opposite limb. The patient has a PIP range of flexion of around 85°.
We measure grip strength and pinch with a dynamometer which is 90 of normal strength to the opposite limb. The patient has a PIP range of flexion of around 85°.
Proximal phalanx extra-articular fractures are common and are associated with significant soft-tissue injury. For stable fracture, conservative treatment is the main treatment. The main objective of treatment is union and preserve the gliding mechanism of tendon with normal motion. In lateral view, fracture has palmar apical configuration with distal fragment that is extended due to the short excursion of the extensor tendon hood and lateral bands and proximal fracture is flexed because the intrinsic muscles flex the MCP joint. The treatment options include conservative open reduction internal fixation (ORIF), and external fixators. ORIF can cause impairment of the gliding layers due to soft-tissue damage. Hence, external fixator proves to be a better alternative. It not only reduces further soft-tissue damage but allows mobilization of joints that helps to reduce chances of joint stiffness [4]. Suzuki et al. in 1994 described a frame made up of K wire and rubber band for managing intra-articular fracture in hand with good results known widely as the Suzuki frame [5]. Badia et al. described an external fixator frame without a rubber band made up of two K wires through the proximal phalanx and head of the middle phalanx for proximal phalanx fracture-dislocation. They achieved good results except in one case where residual pain with flexion [6]. Finsen V modified Suzuki frame rubber with vessel loop for fracture of base of middle phalanx and found stiffness in some cases. The reason for stiffness is the thickness of vessel loop and prolonged frame time [7]. Inanami et al. used three K wire-made dynamic external fixators for four acute and three malunited fracture dislocation of the proximal phalanx with an average range of 88° [8]. Kapur et al. used K wire and jurgan pin balls to construct a frame and treated intra-articular fracture of the middle and proximal phalanx with good results [9]. Sastravaha et al. described a Sriracha external fixator frame made by cutting a plastic syringe and passing K wire through the bone and syringe-like quadruple cortical purchase for the treatment of proximal phalanx fracture-dislocation. They found good results equal to other fixator in their study. The advantage of this fixator is the low cost and simplicity of the application [10].
Min external fixator for phalanx fracture is a cheap and reasonably effective procedure. A needle cap fixator is a good alternative in difficult situations, it helps in correcting the deformity as well as keeps the joint surface distracted.
A needle cap fixator is a good alternative in a difficult situation, it helps in correcting the deformity as well as keeps the joint surface distracted.
References
- 1.Barton N. Internal fixation of hand fractures. J Hand Surg Br 1989;14:139-42. [Google Scholar | PubMed]
- 2.Singh J, Jain K, Mruthyunjaya, Ravishankar R. Outcome of closed proximal phalangeal fractures of the hand. Indian J Orthop 2011;45:432-8. [Google Scholar | PubMed]
- 3.Kurzen P, Fusetti C, Bonaccio M, Nagy L. Complications after plate fixation of phalangeal fractures. J Trauma 2006;60:841-3. [Google Scholar | PubMed]
- 4.Pennig D, Gausepohl T, Mader K, Wulke A. The use of minimally invasive fixation in fractures of the hand--the minifixator concept. Injury 2000;31 Suppl 1:102-12. [Google Scholar | PubMed]
- 5.Suzuki Y, Matsunaga T, Sato S, Yokoi T. The pins and rubbers traction system for treatment of comminuted intraarticular fractures and fracture-dislocations in the hand. J Hand Surg Br 1994;19:98-107., Erratum in: J Hand Surg [Br] 1994;19:408. [Google Scholar | PubMed]
- 6.Badia A, Riano F, Ravikoff J, Khouri R, Gonzalez-Hernandez E, Orbay JL. Dynamic interdigital external fixation for proximal interphalangeal joint fracture dislocations. J Hand Surg Am 2005;30:154-60. [Google Scholar | PubMed]
- 7.Finsen V. Suzuki’s pins and rubber traction for fractures of the base of the middle phalanx. J Plast Surg Hand Surg 2010;44:209-13. [Google Scholar | PubMed]
- 8.Inanami H, Ninomiya S, Okutsu I, Tarui T. Dynamic external finger fixator for fracture dislocation of the proximal interphalangeal joint. J Hand Surg Am 1993;18:160-4. [Google Scholar | PubMed]
- 9.Kapur B, Paniker J, Casaletto J. An alternative technique for external fixation of traumatic intra-articular fractures of proximal and middle phalanx. Tech Hand Up Extrem Surg 2015;19:163-7. [Google Scholar | PubMed]
- 10.Sastravaha N, Limudomporn K, Taweewuthisub W. A novel technique for dynamic external fixation of proximal interphalangeal joint fracture-dislocations. J Hand Surg Asian Pac Vol 2020;25:427-33. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Bridge Plating of Second and Third Carpometacarpal Fracture Dislocations: A Case Report of Rare Injury
January 1, 2026 Bridge Plating of Second and Third Carpometacarpal Fracture Dislocations: A Case Report of Rare Injury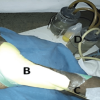 January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial
January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre
November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre October 1, 2025 Burden, Treatment Patterns, and Functional Recovery of Hand Injuries in a Tertiary Hospital of Eastern India
October 1, 2025 Burden, Treatment Patterns, and Functional Recovery of Hand Injuries in a Tertiary Hospital of Eastern India