
Clenched fist injury not always means a boxer fracture. This kind of rare fracture is also a possibility.
Dr. Sivabalaganesh Amirthalingam, Department of Orthopaedics, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: sivabalaganeshamirthalingam@gmail.com
Abstract
Introduction: Isolated displaced fourth and fifth metacarpal base fracture without a carpometacarpal joint subluxation or carpal bone fracture by a punch injury is extremely rare. The site of the fracture in the metacarpal is determined by the type and direction of punch. These fractures usually occur as a result of misdirected blow or wrong punch on a hard surface with a clenched fist. To best of our knowledge, there are only few published case reports. The difficulties in management and biomechanics of such fractures with 10 months follow-up are discussed in this case report.
Case Report: A 37-year-old male right hand dominant person presented with pain and swelling of the right hand after punching a wall. The difficulties in reduction and fixation of such fracture, the functional and radiological outcome of minimally open Kirschner wires fixation of this type of fracture with 10-month follow-up and the fracture biomechanics has been discussed in this case report.
Conclusion: Clenched fist injury not always means a boxer fracture. This kind of rare fracture is also a possibility and should kept as a differential diagnosis. These fractures are easily misinterpreted by a beginner. Meticulous reduction techniques and fixation will yield better results.
Keywords: Base of fourth and fifth metacarpal fracture, biomechanics of fist injury, fist injury, metacarpal base fractures, boxer’s fracture
Metacarpal fractures account for 40% of all upper extremity fractures [1]. Metacarpal fractures are particularly common in the young adult population who is most likely to sustain athletic or vehicular trauma [2]. Isolated fourth and fifth metacarpal base fractures are relatively rare. These fractures usually occur as a result of misdirected blow or wrong punch on a hard surface with a clenched fist. To best of our knowledge, there are only few published case reports.
A 37-year-old male right hand dominant person presented with pain, swelling, and difficulty in performing hand movements of the right hand after punching a wall. The patient presented to us immediately on the day of injury. There was a diffuse swelling and tenderness over the ulnar aspect of the right hand. Active movements of the ring and little fingers were restricted and associated with severe pain. Radiographs taken at the time of presentation showed a dorsally displaced partial articular fracture of the fourth and fifth metacarpal base shown in (Fig. 1).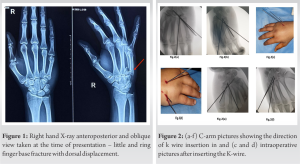 Computed tomography (CT) scan and lateral radiographs were not taken at the time of presentation. After obtaining informed consent, the patient was taken up for an emergency, closed reduction, and percutaneous Kirshner wire fixation. On a hand table under C-arm guidance, closed reduction of the fracture was attempted. As CT scans were not taken intraoperatively, the fracture was visualized under C-arm in multiple views to ensure, there was no dislocation of the Carpometacarpal (CMC) joints. The fracture was reduced by longitudinal traction of the ring and little finger and applying pressure over the metacarpal shaft followed by slightly extending the wrist and hyper pronating the forearm. There was difficulty in maintaining the reduction as the fracture displaced on releasing the axial traction. A total of three 1.5 mm Kirshner wires were used to stabilize the fractures. Initially, the fourth metacarpal was stabilized by passing a Kirschner wire directed from dorsomedial catching the proximal and distal fragments and the wire was anchored in the hamate with three cortical purchases (Fig. 2a). The fifth metacarpal reduction and stabilization was challenging as the reduction was not maintained in a single Kirschner wire and there was soft-tissue interposition making the reduction more difficult. This was an oblique type of fracture hence decided to do a divergent mono lateral Kirschner wire fixation (Fig. 2b). The entry point was chosen in such a way that they are far apart as possible where they cross the fracture line. A stab incision was made over the dorsoulnar aspect of the fifth metacarpal and an artery forceps was introduced to release the soft tissue then a Kirschner wire was entered as shown in the clinical picture (Fig. 2c and d) from the dorsoulnar aspect of the fifth metacarpal with the trajectory directed toward the capitate and bony resistance was felt throughout the K-wire insertion, ensuring the rotation of the little finger was maintained. The wire was inserted transfixing the shaft and base to the capitate and another Kirschner wire was passed from the dorsoulnar aspect slightly lateral to the first wire in the fifth metacarpal proximal and distal fragment transfixing the capitate shown in (Fig. 2e and 2f). The upper limb was put in a below elbow pop slab for 3 weeks. The Kirshner wires were removed at 3 weeks and the splint was maintained for a total of 4 weeks.
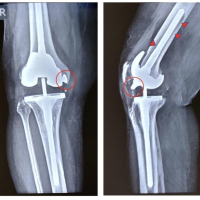
Computed tomography (CT) scan and lateral radiographs were not taken at the time of presentation. After obtaining informed consent, the patient was taken up for an emergency, closed reduction, and percutaneous Kirshner wire fixation. On a hand table under C-arm guidance, closed reduction of the fracture was attempted. As CT scans were not taken intraoperatively, the fracture was visualized under C-arm in multiple views to ensure, there was no dislocation of the Carpometacarpal (CMC) joints. The fracture was reduced by longitudinal traction of the ring and little finger and applying pressure over the metacarpal shaft followed by slightly extending the wrist and hyper pronating the forearm. There was difficulty in maintaining the reduction as the fracture displaced on releasing the axial traction. A total of three 1.5 mm Kirshner wires were used to stabilize the fractures. Initially, the fourth metacarpal was stabilized by passing a Kirschner wire directed from dorsomedial catching the proximal and distal fragments and the wire was anchored in the hamate with three cortical purchases (Fig. 2a). The fifth metacarpal reduction and stabilization was challenging as the reduction was not maintained in a single Kirschner wire and there was soft-tissue interposition making the reduction more difficult. This was an oblique type of fracture hence decided to do a divergent mono lateral Kirschner wire fixation (Fig. 2b). The entry point was chosen in such a way that they are far apart as possible where they cross the fracture line. A stab incision was made over the dorsoulnar aspect of the fifth metacarpal and an artery forceps was introduced to release the soft tissue then a Kirschner wire was entered as shown in the clinical picture (Fig. 2c and d) from the dorsoulnar aspect of the fifth metacarpal with the trajectory directed toward the capitate and bony resistance was felt throughout the K-wire insertion, ensuring the rotation of the little finger was maintained. The wire was inserted transfixing the shaft and base to the capitate and another Kirschner wire was passed from the dorsoulnar aspect slightly lateral to the first wire in the fifth metacarpal proximal and distal fragment transfixing the capitate shown in (Fig. 2e and 2f). The upper limb was put in a below elbow pop slab for 3 weeks. The Kirshner wires were removed at 3 weeks and the splint was maintained for a total of 4 weeks. 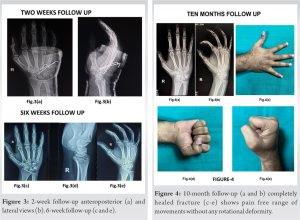 Following which the rehabilitation was started like active grip strengthening exercises (foam ball pinch, Towel squeeze exercise, finger lift, and stretch exercises) were commenced under supervision. Radiographs were taken at 2 weeks (Fig. 3a and 3b), 6 weeks (Fig. 3d-f), and 10th month (Fig. 4a and b) showed no loss of reduction and the fracture was completely healed without any rotational deformity (Fig. 4d) and he was able to perform pain free hand movements (Fig. 4c and 4e) and his grip strength was completely restored equal to the opposite hand measured by a Jamar dynamometer at 10-month follow-up.
Following which the rehabilitation was started like active grip strengthening exercises (foam ball pinch, Towel squeeze exercise, finger lift, and stretch exercises) were commenced under supervision. Radiographs were taken at 2 weeks (Fig. 3a and 3b), 6 weeks (Fig. 3d-f), and 10th month (Fig. 4a and b) showed no loss of reduction and the fracture was completely healed without any rotational deformity (Fig. 4d) and he was able to perform pain free hand movements (Fig. 4c and 4e) and his grip strength was completely restored equal to the opposite hand measured by a Jamar dynamometer at 10-month follow-up.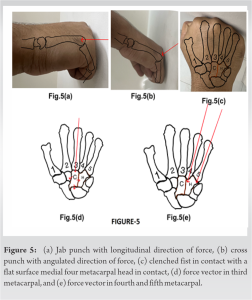
Isolated displaced fracture of the base of the fourth and fifth metacarpal is relatively rare [2]. The base of fourth and fifth metacarpal fractures has been well discussed and reported in literature but are almost always reported with CMC subluxation or hamate fractures and are easily missed [3,4]. However, the specialty about this case is the mechanism of the injury. Typically, the neck of the metacarpal is fractured when a longitudinal blunt force is applied. A very high force will cause CMC dislocation, hamate fracture, or an open fracture. A lateral view X-ray of the hand should be taken as these fracture dislocation can be missed [5]. The basic type of punches that are seen in boxing are Jab- a sudden punch, Cross – a straight punch, Hook – a short side power punch, upper cut – a short swinging upward power punch. In the literature, it has been described that fistfight is the common cause of fracture in the fifth metacarpal and the most common age group involved is young athletic individuals. The site and the pattern of fracture depend on the type of punch. In a jab type of punch, the resultant force will travel along the longitudinal axis of the metacarpal that will cause a compression and fracture in the base of metacarpal (Fig. 5a). In cross or hook punch, the resultant force will be angulated and cause fracture in the neck/sub capital region of the metacarpal (Fig. 5b). A clenched fist when contact with a flat surface all the medial four metacarpal head are in contact but the fracture is more common in the fifth metacarpal (Fig. 5c). Anatomically, the fourth and fifth metacarpal articulates with the hamate which forms a saddle type of synovial joint there by providing gliding, flexion and rotation movements in fourth and fifth CMC joint which increases the range of movement of hand [6]. The second and third CMC joint is plane synovial joint and its relatively rigid joint [6]. The second metacarpal articulates with the trapezium, trapezoid, capitate, and the third metacarpal making it the most stable CMC joint (Fig. 5c). The third metacarpal articulates with the capitate which is the largest carpal bone and it forms the keystone of the carpus. Theoretically when a high force is applied to static object, the object tends to break in the weakest point. When two objects are closely held together, the force will transmit to the other object and the force will be gradually reduced, once it reaches the terminal object and the structure would not break as the end force will not be strong enough to cause fracture. This principle can be applied to the fist injury for better understanding of the fracture. The second and third CMC joint is relatively rigid thus the total force applied will be transmitted to the capitate and the carpal bones and distributed so that the resultant force would not be strong enough to cause fracture (Fig. 5d). In our case, we hypothesize that the resultant vector force acting on the fourth and fifth metacarpal gets transferred to the CMC joint in this case the hamate (Fig. 5e). The fourth and the fifth CMC joint being relatively weak compared to the other two joints, there will be incomplete transmission of the applied force and if the remaining force is strong enough to produce a fracture. However, the irregularly shaped hamate bone provides attachment to numerous ligaments and muscles which redistributes the loading force to the surrounding structures. Hence, a very high force required for hamate fracture [7]. Surgical fixation these kind of fracture is debatable as fracture relatively similar to this type has been treated conservatively. Failure to achieve satisfactory reduction and stability can lead to decreased grip strength, non-union, and severe degenerative arthritis [8,9]. Alternate methods of fixation for similar fracture patterns done in the literature are by inserting the Kirschner wire from the fifth metacarpal shaft to the fourth metacarpal shaft for the base of the fifth [10,11]. Then obliquely oriented k-wire insertion to fix the fifth metacarpal base to the hamate [12]. In our case, the fourth metacarpal is also fractured so we decided to fix it with the hamate [13]. Intramedullary headless compression screws for midshaft and proximal third metacarpal fractures have been used successfully with a good radiological and functional outcome [14].
Clenched fist injury not always means a boxer fracture. This kind of rare fracture is also a possibility and should kept as a differential diagnosis. These fractures are easily misinterpreted by a beginner. Meticulous reduction techniques and fixation will yield better results.
Any case presenting with fist injury may not always be a boxer fracture, the fracture patterns vary with the direction of punch. A misdirected blow may cause this kind of rare fracture pattern. Surgeons should not hesitate in asking additional investigation in seeing such cases as these kind of fractures are easily misinterpreted by a beginner.
References
- 1.Downing ND, Davis TR. Hand Clin 2010;26:169-77. [Google Scholar | PubMed]
- 2.Moore A, Varacallo M. Metacarpal hand fracture. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. [Last accessed on 2022 Nov 26]. [Google Scholar | PubMed]
- 3.Gaheer RS, Ferdinand RD. Fracture dislocation of carpometacarpal joints: A missed injury. Orthopedics 2011;34:399. [Google Scholar | PubMed]
- 4.. Büren C, Gehrmann S, Kaufmann R, Windolf J, Lögters T. Management algorithm for index through small finger carpometacarpal fracture dislocations. Eur J Trauma Emerg Surg 2016;42:37-42. [Google Scholar | PubMed]
- 5.Braakman M. Are lateral X-rays useful in the treatment of fractures of the fourth and fifth metacarpals? Injury 1998;29:1-3. [Google Scholar | PubMed]
- 6.Metikala S, Herickhoff P. Isolated dorsal dislocations of the fourth and fifth carpometacarpal joints: A case report and review of literature. Cureus 2020;12:e12310. [Google Scholar | PubMed]
- 7.Price MB, Vanorny D, Mitchell S, Wu C. Hamate body fractures: A comprehensive review of the literature. Curr Rev Musculoskelet Med 2021;14:475-84. [Google Scholar | PubMed]
- 8.Balaram AK, Bednar MS. Complications after the fractures of metacarpal and phalanges. Hand Clin 2010;26:169-77. [Google Scholar | PubMed]
- 9.Swanson AB. Fractures involving the digits of the hand. Orthop Clin North Am 1970;1:261-74. [Google Scholar | PubMed]
- 10.Dillon J, Street J, Mahalingham K. Divergent dislocation of the ring and little finger carpometacarpal joints--a rare injury pattern. Acta Orthop Belg 2005;71:353-6. [Google Scholar | PubMed]
- 11.Bushnell BD, Draeger RW, Crosby CG, Bynum DK. Management of intra-articular metacarpal base fractures of the second through fifth metacarpals. J Hand Surg Am 2008;33:573-83. [Google Scholar | PubMed]
- 12.Wong TC, Ip FK, Yeung SH. Comparison between percutaneous transverse fixation and intramedullary K-wires in treating closed fractures of the metacarpal neck of the little finger. J Hand Surg Br 2006;31:61-5. [Google Scholar | PubMed]
- 13.Kelsch G, Ulrich C. Intramedullary K-wire fixation of metacarpal fractures. Arch Orthop Trauma Surg 2004;124:523-6. [Google Scholar | PubMed]
- 14.Hoang D, Huang J. Antegrade intramedullary screw fixation: A novel approach to metacarpal fractures. J Hand Surg Glob Online 2019;1:229-35. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 December 10, 2022 Unusual Failure of Modular TKA Prosthesis and Screw Migration following Revision Total Knee Arthroplasty
December 10, 2022 Unusual Failure of Modular TKA Prosthesis and Screw Migration following Revision Total Knee Arthroplasty June 10, 2023 ACL Reconstruction in a Poliotic Limb with Peroneus Longus Graft
June 10, 2023 ACL Reconstruction in a Poliotic Limb with Peroneus Longus Graft September 24, 2017 Head-on Allograft Transplantation: A Unique Case Report Where a Large Piece of Femoral Bone was Extruded from One Patient’s Body and Impaled Another Patient’s Tibia
September 24, 2017 Head-on Allograft Transplantation: A Unique Case Report Where a Large Piece of Femoral Bone was Extruded from One Patient’s Body and Impaled Another Patient’s Tibia September 10, 2022 Trans-Scaphoid Perilunate Fracture Dislocation Managed With Open Reduction: A Case Report
September 10, 2022 Trans-Scaphoid Perilunate Fracture Dislocation Managed With Open Reduction: A Case Report