
The association of bilateral scaphoid and distal radius fractures is extremely rare, can be neglected, requires a precise diagnosis and appropriate therapeutic management.
Dr. Nadhir Meraghni, Department of Orthopaedic Surgery, Centre Hospitalier Universitaire Mustapha Bacha, Place du 1er Mai, 16000, Algiers - Algeria. E-mail: nadhir.meraghni@gmail.com
Abstract
Introduction: A combination of bilateral scaphoid and distal radius fractures is extremely rare. It may occur as a result of high-energy trauma and can be neglected. The current paper described a case study of this rarely combined fracture.
Case Report: A 22-year-old female was admitted to the emergency department following a fall while exercising which resulted in severe pain in both wrists without any neurovascular deficit. X-ray imaging showed bilateral combined fractures of the scaphoid and distal radius. To fix the fractures, the patient underwent closed reduction and internal fixation with Kirschner wires along with immobilization for 3 months. The radius and scaphoid fractures were united within approximately 6 and 10 weeks, respectively.
Conclusion: Combined bilateral scaphoid and distal radius fractures are extremely rare resulting from high-energy trauma. The associated fractures require a precise diagnosis and appropriate therapeutic management.
Keywords: distal radius, scaphoid, fracture, bilateral, reduction
Bilateral combined fractures of the scaphoid and distal radius are an extremely rare association in trauma injuries and probably result from a high-energy trauma [1]. In fact, there are only two cases reported in the literature thus far [1]. In the current paper, the authors described an extremely rare entity of fracture association in a 22-year-old female who was victim of physical exercise accident.
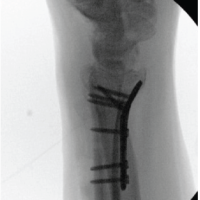
A 22-year-old female was admitted to the emergency department after a sport-related fall causing severe pain in both wrists, without skin or neurovascular damage. The radiographs showed combined bilateral fractures of the scaphoid and distal radius. Both distal radial fractures and scaphoid fractures were Type A according to the AO classification and the Herbert classification respectively (Fig.1A, 1B).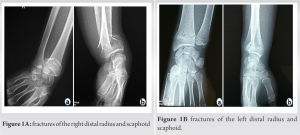 The patient was operated on under general anesthesia. Starting with the left wrist, first, we proceeded to a closed reduction and fixation of the distal radius fractures with Kirschner wires under fluoroscopic control. Then, the scaphoid fracture was stabilized with percutaneous Kirschner wires from distal to proximal. The same procedures were performed on the right limb (Fig. 2a, 2b).
The patient was operated on under general anesthesia. Starting with the left wrist, first, we proceeded to a closed reduction and fixation of the distal radius fractures with Kirschner wires under fluoroscopic control. Then, the scaphoid fracture was stabilized with percutaneous Kirschner wires from distal to proximal. The same procedures were performed on the right limb (Fig. 2a, 2b). This was followed by immobilization using cast. Three month post-surgery, the cast was removed and wrist range-of-motion exercises were started. The radius fractures and the scaphoid fractures were united within 6 weeks and 10 weeks, respectively. The wrist range of motion was measured using a goniometer. On the right side, he mean range of motion at 12 months follow-up was of 110 degrees for combined extension and flexion, 30 degrees for combined arc of radial and ulnar deviation, and 135 degrees for the combined pronation and supination. For the left side, it was of 105 degrees for extension and flexion, 28 degrees for radial and ulnar deviation, and 140 degrees for pronation and supination. (Fig. 3A, 3B, 3C, 3D). The Visual Analogic Scale (VAS) was of 1 on the right wrist and of 2 on the left side. The Quick Dash score was of 4.5 for both sides on the last follow-up.
This was followed by immobilization using cast. Three month post-surgery, the cast was removed and wrist range-of-motion exercises were started. The radius fractures and the scaphoid fractures were united within 6 weeks and 10 weeks, respectively. The wrist range of motion was measured using a goniometer. On the right side, he mean range of motion at 12 months follow-up was of 110 degrees for combined extension and flexion, 30 degrees for combined arc of radial and ulnar deviation, and 135 degrees for the combined pronation and supination. For the left side, it was of 105 degrees for extension and flexion, 28 degrees for radial and ulnar deviation, and 140 degrees for pronation and supination. (Fig. 3A, 3B, 3C, 3D). The Visual Analogic Scale (VAS) was of 1 on the right wrist and of 2 on the left side. The Quick Dash score was of 4.5 for both sides on the last follow-up.
Simultaneous fractures of the distal radius and scaphoid are uncommon [2,3,4,5]. Bilateral combined association of these fractures is extremely rare and results due to high-energy trauma [1, 6 ]. There is no consensus regarding the me chanism of injury [7]. Because fractures of the scaphoid involve extension and ulnar deviation of the wrist to place the scaphoid in a vertical and vulnerable position with three-point bending stresses applied, it seems likely that the scaphoid fracture occurs first and then continued axial loading and extension of the wrist results in the fractures of the radius [8,9]. Frykman noted that for this combined injury to occur, the required loads must be in a radial direction and higher than the ones required for the radius to fracture alone. In his experiment, the distal radial fracture occurred first, followed by the scaphoid fracture. Stother proposed that fractures of the scaphoid and the distal radius can occur only if the radius is relatively strong so that hyperextension at the wrist and fracture of the scaphoid occurs before the distal radial fracture [2]. Operative treatment is recommended even if fractures are not displaced [1]. In addition, to stabilizing the lesions, it reduces the risk of secondary displacement and allows early rehabilitation. Different methods are used to treat distal radial fractures including percutaneous pinning using Kirschner wires, plates, and external fixation. For the case described in this paper, we opted for the first method as the fractures were not complex. With the regards to the scaphoid fractures, we can use fixation with Herbert screws
or Kirschner wires and we chose fixation with Kirschner wires. The advantages of wires are reduction of the risk of infection and facilitation of functional recovery. The inconveniences are the difficulty to obtain anatomical reduction and the increased risks of complications: including secondary displacement, migration of wires and damage to tendons. A precise diagnosis and appropriate therapeutic management are required for this rare association of fractures. This case highlights the importance of careful examination for concomitant injuries following upper extremity fractures. Scaphoid fractures can easily be neglected as they are not readily visualized on initial plain radiographs. Scaphoid nonunion and carpal instability are the major complications of scaphoid fractures. Early diagnosis and treatment are crucial to such complications [10].
A combination of bilateral scaphoid and distal radius fractures is very rare resulting from high-energy traumas. This association requires a precise diagnosis and appropriate therapeutic management.
The association of bilateral scaphoid and distal radius fractures is extremely rare in trauma and it is highly likely a result of a high-energy trauma. Although this extremely rare entity of injury association would rest in serious complications if left untreated, commonly it is neglected due to missed diagnosis on plain radiographs. Radiography diagnostic assessment accuracy followed by appropriate surgical therapy and postoperative management are pivotal for the treatment of simultaneous bilateral scaphoid and distal radius fractures.
References
- 1.Ozkan K, Ugutmen E, Unay K et al. Fractures of the bilateral distal radius and scaphoid: a case report. J Med Case Reports 2008,2:93. https://doi.org/10.1186/1752-1947-2-93. [Google Scholar | PubMed | CrossRef]
- 2.Hove M. Simultaneous scaphoid and distal radial fractures. Journal of Hand Surgery (British and European Volume, 1994;19B:384-388. [Google Scholar | PubMed]
- 3.Hamdi MF. Scaphoid fracture associated with distal radius fracture in children: a case report. Chinese Journal of Traumatology 2009;12(3):187-188. [Google Scholar | PubMed]
- 4.Zrig M and al. Combined fracture of the distal radius and scaphoid in children. Report of two cases. Chirurgie de la main 2009;28:42-45. [Google Scholar | PubMed]
- 5.Joseph F and al. Combined Fractures of the Scaphoid and Distal Radius: A Revised Treatment Rationale Using Percutaneous and Arthroscopic Techniques. Hand Clinics 21 2005:427-441. [Google Scholar | PubMed]
- 6.Dumontier C and al. Combined scaphoid and distal radius fractures in adults. Hand Surgery and Rehabilitation 2016;35S:55-59. [Google Scholar | PubMed]
- 7.Yusuf Gürbüz, Tahir Sadık Sügün, Murat Kayalar. Combined Fractures of the Scaphoid and Distal Radius: Evaluation of Early Surgical Fixation (21 Patients with 22 Wrists). J Wrist Surg 2018;07(01):11-17. [Google Scholar | PubMed]
- 8.Thomas E. Trumble, Stephen K. Benirschke, Nicholas B. Vedder. Ipsilateral fractures of the scaphoid and radius. HAND SURG 1993;18A:8-14. [Google Scholar | PubMed]
- 9.Mayfield JK. Mechanism of carpal injuries. Clin Orthop 1980;149:45-54. [Google Scholar | PubMed]
- 10.Kay RM, Kuschner SH. Bilateral proximal radial and scaphoid fractures in a child. Journal of Hand Surgery (British and European Volume, 1999) 24B;2:255–257. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2024 Fixation of 3-Part Intra Articular Distal Radius Fracture with Combined Volar Plate and Dorsal Spanning Plate: A Case Report
November 1, 2024 Fixation of 3-Part Intra Articular Distal Radius Fracture with Combined Volar Plate and Dorsal Spanning Plate: A Case Report August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report
August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report
August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report August 1, 2026 Open Reduction and Internal Fixation of Gartland Type III Supracondylar Humerus Fractures Using the Posterior Paratricipital Approach: A Case Series
August 1, 2026 Open Reduction and Internal Fixation of Gartland Type III Supracondylar Humerus Fractures Using the Posterior Paratricipital Approach: A Case Series