
Complex knee subluxations can be corrected with hexagonal fixators in a single sitting without changes in hardware.
Dr. Raj Milind Sawant, Department of Orthopaedic Surgery, Dr. D. Y. Patil Medical College and Hospital, Navi Mumbai - 400 706, Maharashtra, India. E-mail: rajsawant135@gmail.com
Introduction: The aim of the study was to study results of (made in India) hexapod external fixator (HEF) (deft fix)-assisted correction in a case of knee subluxation with malunited medial tibial condyle fracture.
Methodology: A subject with knee subluxation was selected for application of hexapod and Ilizarov ring fixator for staged correction of subluxation using deft fix-assisted correction.
Result: The study shows anatomical reduction of the subluxated knee using HEF with deft fix-assisted correction.
Conclusion: The HEF does not require frame transformation and is easier to use and is known to have the ability to correct complex multiplanar deformities better and much faster than the traditional Ilizarov ring fixator which requires multiple changes in hardware while correcting complex deformities. Software-assisted hexapod correction provides more faster and accurate correction with the ability to do fine adjustments at any stage of correction.
Keywords: Hexapod fixator, external fixator, knee subluxation, deftfix.
Hexapod external fixator (HEF) is a device that can correct deformities in six axes and Taylor Spatial Frame (TSF) is the most commonly used device [1]. Projective geometry is the mathematical basis of all hexapod system which describes the complex geometry of an object in space [1]. TSF was developed by Taylor brothers [1]. This system is now the most commonly used six axes deformity correction system [1]. Deformity analysis is an essential component for using TSF of a limb and the operating surgeon must be well versed in this [2, 3]. Six telescopic sturts which are attached at universal joints help in connecting two partial or full rings (Fig. 1). Calculation of deformity, mounting, and frame parameters is an essential component used in planning of TSF [2, 3]. The reference frame is usually the point of location of origin which can be either proximal or distal [2, 3]. The moving fragments usually carry the corresponding points [2, 3]. Pre-operative X-rays can be an excellent guide for deformity correction [2, 3]. Parameters which are most commonly used for deformity analysis include anteroposterior and lateral views of angulation and translation, axial view angulation and translation [2, 3]. Clinical examination can reveal rotational deformity [2, 3]. The relationship between the reference ring and the origin is reflected by mounting parameters [2, 3]. The diameter of the rings and the length of the sturts are defined by the information provided by frame parameters [1]. In case of open fractures, TSF can be used to stabilize fracture and can also be used in case of acute trauma to tibia [4, 5, 6, 7]. In primary management, reduction is held using sturts between two rings and the remaining malalignment is corrected later using the total residual program [1]. The added advantage of the TSF is its ability to offer multidirectional deformity correction without changing the main structure as there are various parameter which are needed to be measured by the surgeon and therefore high chances of subjective errors [8]. The HEF using computer-assisted 3Dsoftware helps in planning fracture reduction and deformity correction eliminating the need for calculating parameters using traditional methods [8].
We present a case of a 28-year-old male who presented to us with a chief complaint of pain and swelling over the left knee with a restricted range of motion for 8 months with foot drop. He had a history of road traffic accidents 8 months ago during which he suffered a slip and fall and developed pain and swelling with fracture of the medial condyle and subluxation of the knee joint. He was operated on at an outside hospital where open reduction internal fixation with plating for medial tibial condyle fracture was done. The patient had developed a left-sided food drop postoperatively. The patient’s range of motion was restricted post-operatively and presented to us after 8 months. Clinical pictures on admission show healed surgical scar along with swelling present diffusely over the left knee with a valgus deformity and knee subluxation (Fig. 2a-d). The patient was assessed clinically and the deformity in his left knee was assessed. His range of motion at the knee joint was found to be 15–90° with a fixed flexion deformity of 15° (Fig. 2e). Pre-operative X-rays films were taken which showed a malunited medial condyle fracture of the tibia with knee subluxation with the implant in situ (Fig. 3a-d). The patient was planned for surgery after routine blood investigations and taking fitness. The incision was taken over the proximal tibia previously healed surgical scar on the anterolateral side. Dissection was done and implant removal of the proximal tibial plate was done. 160 mm 2 rings and half ring construct was made over the distal femur and fixed with Ilizarov wires and the 160 mm 2 rings construct progressed over the proximal tibia and fixed with Ilizarov wires.
The patient was assessed clinically and the deformity in his left knee was assessed. His range of motion at the knee joint was found to be 15–90° with a fixed flexion deformity of 15° (Fig. 2e). Pre-operative X-rays films were taken which showed a malunited medial condyle fracture of the tibia with knee subluxation with the implant in situ (Fig. 3a-d). The patient was planned for surgery after routine blood investigations and taking fitness. The incision was taken over the proximal tibia previously healed surgical scar on the anterolateral side. Dissection was done and implant removal of the proximal tibial plate was done. 160 mm 2 rings and half ring construct was made over the distal femur and fixed with Ilizarov wires and the 160 mm 2 rings construct progressed over the proximal tibia and fixed with Ilizarov wires. Proximal construct’s proximal ring is fixed with 2 Schanz pins and the distal ring with 1 Schanz pin. Distal constructs proximal ring fixed with 2 Schanz pins and distal ring with 1 Schanz pin. Clinical picture post-operative shows Stage 1 Ilizarov ring fixator application (Fig. 4). Post-operative X-rays were taken after the application of the Ilizarov ring fixator (Fig. 5a and b). In Stage 2, hexapod sturts were applied and deformity correction was started in a staged manner (Fig. 6a-d).
Proximal construct’s proximal ring is fixed with 2 Schanz pins and the distal ring with 1 Schanz pin. Distal constructs proximal ring fixed with 2 Schanz pins and distal ring with 1 Schanz pin. Clinical picture post-operative shows Stage 1 Ilizarov ring fixator application (Fig. 4). Post-operative X-rays were taken after the application of the Ilizarov ring fixator (Fig. 5a and b). In Stage 2, hexapod sturts were applied and deformity correction was started in a staged manner (Fig. 6a-d). After attaching hexapod sturts X-rays of the left knee were taken in AP and lateral views which were uploaded in deft fix software and calculations were made of angle, and translation both in AP and lateral views (Fig. 7a-c).
After attaching hexapod sturts X-rays of the left knee were taken in AP and lateral views which were uploaded in deft fix software and calculations were made of angle, and translation both in AP and lateral views (Fig. 7a-c). 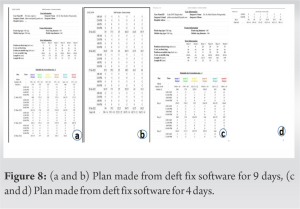 A staged correction was started using a plan made from deft fix software for 9 days (Fig. 8a and b). Subluxation was assessed clinically. X-rays of the left knee AP and lateral were assessed using a deft fix and the second plan of correction was made which was followed for 4 days (Fig. 8c and d). X-rays of knee AP and lateral views were taken on post-operative day 15 (Fig. 9a and b). Physiotherapy was started for the patient in the form of knee range of motion exercises, ankle pumps, active toe movements, and the patient was made to walk with a walker. X-rays were again repeated 1-month post-operative (Fig. 9c and d).
A staged correction was started using a plan made from deft fix software for 9 days (Fig. 8a and b). Subluxation was assessed clinically. X-rays of the left knee AP and lateral were assessed using a deft fix and the second plan of correction was made which was followed for 4 days (Fig. 8c and d). X-rays of knee AP and lateral views were taken on post-operative day 15 (Fig. 9a and b). Physiotherapy was started for the patient in the form of knee range of motion exercises, ankle pumps, active toe movements, and the patient was made to walk with a walker. X-rays were again repeated 1-month post-operative (Fig. 9c and d).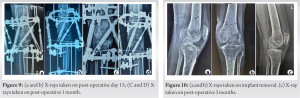 Implant removal was done on post-operative day 45 and X-rays were taken which showed a good reduction of knee joint both in AP and lateral views (Fig. 10a and b). The patient showed a good range of motion after the removal of the hexapod and was highly satisfied with the treatment. X-ray was repeated on a post-operative day 3 months which showed a good reduction of the knee joint (Fig. 10c).
Implant removal was done on post-operative day 45 and X-rays were taken which showed a good reduction of knee joint both in AP and lateral views (Fig. 10a and b). The patient showed a good range of motion after the removal of the hexapod and was highly satisfied with the treatment. X-ray was repeated on a post-operative day 3 months which showed a good reduction of the knee joint (Fig. 10c).
The concept of six axes correction-the hexapod fixator. Hexa-6: Pod-legs, these six sturts are arranged in v-fashion with software-assisted movements. Deformities exist in 3-dimensional space and what we see is two-dimensional representation (AP and lateral) views of three-dimensional deformities. The correction of these deformities occurs in three dimensions. Y-axis– AP view, X-axis – lateral view, Z-axis – axial view. Any object can be defined in three-dimensional space about its position relative to these three axes. Any deformity that we see in the AP and lateral view is a deformity which is in 3D space and can be defined by the X, Y, and Z axis. While correcting deformities two kinds of movements are there, three translation movements, axial (lengthening/shortening along the y-axis), transverse (sagittal along the X-axis), and transverse (frontal along the Z-axis). Three rotations, frontal plane (angulation around the Z-axis), sagittal plane (angulation around X-axis), and axial (torsional around Y-axis). With a conventional Ilizarov system, all three deformities can be corrected but multiple steps with the sequential change of hardware are required in the following order: (1) Lengthening, (2) AP correction, (3) lateral correction, and (4) torsional correction. All these steps can be done at the same time using a hexapod fixator with help of software, software accepts inputs of where is this frame in 3D space about deformity and creates a map by multiple measurements of lengths of these sturts, where these sturts are connected, size of rings, movement occurring at the fulcrum. Inputs can be given regarding movements around the fulcrum, and the various movements that you want to do. It can be angulation in a particular plane depending on the X-ray and the software tells you how much these sturts have to be adjusted and gives a plan of approximately 10 days of how each of these sturts has to be adjusted for scheduled correction.
The study shows anatomical reduction of the subluxated knee using a HEF.
HEF is a software-assisted modification of ilizarov external fixator which provides more precise reduction without the need for change of hardware in multiple stages .However, this is a technically demanding surgery as the surgeon must have in depth knowledge of the HEF application and the use of computer software for calibration.
References
- 1.Keshet D, Eidelman M. Clinical utility of the Taylor spatial frame for limb deformities. Orthop Res Rev 2017;9:51-61. [Google Scholar]
- 2.Paley D. History and science behind the six-axis correction external fixation devices in orthopaedic surgery. Oper Tech Orthop 2011;21:125-8. [Google Scholar]
- 3.Standard S, Herzenberg J, Conway J, Siddiqui N. The Art of Limb Alignment. 2nd ed. Baltimore, Maryland: Rubin Institute for Advanced Orthopaedics, Sinai Hospital of Baltimore; 2012. [Google Scholar]
- 4.Al-Sayaad MJ. Taylor spatial frame in the treatment of paediatric and adolescent tibial shaft fractures. J Pediatr Orthop 2006;26:164-70. [Google Scholar]
- 5.Zenios M. The use of the Taylor spatial frame for the treatment of unstable tibial fractures in children. J Orthop Trauma 2013;27:563-8. [Google Scholar]
- 6.Eidelman M, Katzman A. Treatment of complex tibial fractures in children with the Taylor spatial frame. Orthopaedics 2008;31:992-5. [Google Scholar]
- 7.Iobst SA. Hexapod external fixation for tibial fractures in children. J Pediatr Orthop 2016;36:S24-8. [Google Scholar]







