
Corroboration of presenting history, clinical acumen, and intraoperative exploration along with histopathological diagnosis is the linchpin of evidence based medicine and in extrapolation, the surgical management of soft-tissue swellings of the hand.
Dr. Arjun Ganesh, Department of Orthopaedics, Sri Ramachandra Institute of Higher Education and Research, No:1 Ramachandra Nagar, Porur, Chennai, Tamil Nadu, India. E-mail: drarjunganesh@gmail.com
Abstract
Introduction: Giant cell tumors of tendon sheath (GCTTS) are benign soft-tissue lesions commonly affecting the digits, which occasionally cause pressure atrophy of an adjoining bone; but perforating the cortex to expand into the medullary canal is quite uncommon. We report such a case of suspected recurrent ganglion cyst with eventually manifested as a GCTTS with an intra-osseous involvement of the capitate and hamate bone.
Case Presentation: A 28-year-old lady had been diagnosed as a case of recurrent ganglion cyst of the dorsum of the left wrist – 6 years ago and 4 years ago – both of which were confirmed histopathologically and were surgically excised. The patient had now presented in July 2021 with similar complaints of pain and swelling over the same site, for 1 year. Our initial clinical diagnosis was a case of recurrent ganglion cyst. Patient also presented with occasional bouts of fever for the past 2 weeks, which made us suspect osteomyelitis as well. Routine blood parameters showed that an elevated ESR and CRP, blood, and urine cultures were negative and magnetic resonance imaging showed features suggestive of osteomyelitis-involvement of capitate and hamate bone. However, to our surprise, intraoperatively, there were no features suggestive of osteomyelitis and the lesion was excised in-toto and the gross specimen resembled a classic ganglion cyst, which was sent for histopathological examination. To our surprise yet again, it was reported as a case of Giant cell tumor of the tendon sheath, which in retrospect, clinically and radiologically correlated with an intra-osseous involvement of the capitate and hamate. The patient is on regular follow-up to pick up any further recurrences.
Conclusion: "Once a ganglion, always a ganglion” should not be taken as the Gospel truth. Histopathological diagnosis continues to remain as the gold standard, especially in cases of soft-tissue swellings of the hand. Correlation and integration of clinical features, Imaging modalities and histopathological diagnosis are the cornerstone in the management of GCTTS.
Keywords: Giant cell tumor of tendon sheath, ganglion, osteomyelitis
Ganglion cysts are considered the most common tumor of the wrist and hand. They are most common between the second and fourth decades of life. The most common anatomical location is the dorsal wrist [1] Giant cell tumors of the tendon sheath (GCTTS) is a benign lesion most commonly attached to the tendons and bones of the fingers, hands [2], but intraosseous extension into the carpal bones and medullary canal of the metacarpals is an extremely uncommon finding. It can mimic and make differential diagnoses with several hand tumors. Definitive diagnosis and the treatment of choice are reached with complete resection and histopathological examination. Most patients present with pain, swelling, joint effusion, and disability in the third and fourth decades of life [3]. We describe an eccentric case report which includes clinical, radiologic, histologic diagnostic, and surgical challenges in an unexpected lytic osseous lesion of the carpal bones.
A 28-year-old lady with no known comorbidities had presented to the outpatient department with chief complaints of pain and swelling over dorsum of the left hand for 1 year, which had aggravated over the past 6 months. Swelling was insidious in onset and gradually progressive, which has increased to the current size of 1.5 cm × 1.5 cm. Swelling is occasionally associated with pain, which was dull, diffuse, and non-radiating in nature. Patient had presented with similar complaints at the same region in the past – two episodes – 4 years and 6 years ago, respectively, which was clinically and radiologically diagnosed as a case of ganglion cyst, which was surgically excised and confirmed with the histopathological diagnosis. On local examination of the left hand, a 4 cm longitudinal scar over the dorsum, in line with the third web space was seen. A non-tender diffuse swelling of size 1.5 cm × 1.5 cm (Fig. 1) was palpable and radial to the scar at level of midcarpal joint.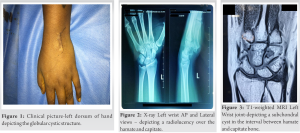 The swelling was firm in consistency, not mobile and appeared more prominent of palmar flexion of the wrist. Full range of motion of the wrist joint and active finger movements were present. Routine blood parameters revealed a WBC Total count of 10,000, ESR-20, and CRP-1.1.
The swelling was firm in consistency, not mobile and appeared more prominent of palmar flexion of the wrist. Full range of motion of the wrist joint and active finger movements were present. Routine blood parameters revealed a WBC Total count of 10,000, ESR-20, and CRP-1.1.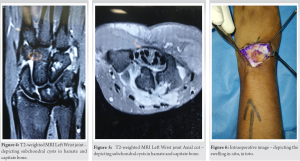 X-ray of the left hand (Fig. 2) revealed no obvious abnormality-apart from a slight radiolucency over the hamate and capitate. Magnetic resonance imaging (MRI) of the left hand revealed (Fig. 3-5)- (1) A focal small cyst beneath extensor digitorum tendon at the level of base of third metacarpal-suggestive occult ganglion cyst.
X-ray of the left hand (Fig. 2) revealed no obvious abnormality-apart from a slight radiolucency over the hamate and capitate. Magnetic resonance imaging (MRI) of the left hand revealed (Fig. 3-5)- (1) A focal small cyst beneath extensor digitorum tendon at the level of base of third metacarpal-suggestive occult ganglion cyst.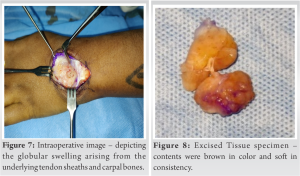 (2) Another similar cyst on the ventral aspect in the interval between capitate and hamate bone. (3) Subchondral cysts in hamate and capitate bone. With the clinical suspicion of a recurrent ganglion cyst with associated osteomyelitis, we had decided to excise the lesionin-toto. Intraoperatively (Fig. 6 and 7), there was a breach of the dorsal cortex of the hamate, with extension of the contents into the dorsal subcapsular and subcutaneous area. Contents were brown in color and soft in consistency.
(2) Another similar cyst on the ventral aspect in the interval between capitate and hamate bone. (3) Subchondral cysts in hamate and capitate bone. With the clinical suspicion of a recurrent ganglion cyst with associated osteomyelitis, we had decided to excise the lesionin-toto. Intraoperatively (Fig. 6 and 7), there was a breach of the dorsal cortex of the hamate, with extension of the contents into the dorsal subcapsular and subcutaneous area. Contents were brown in color and soft in consistency. The tissue specimen (Fig. 8) was sent for culture- sensitivity and histopathology. Fungal culture and KOH mount were negative. Bacterial culture was negative. Histopathology biopsy report revealed–tendinous tissue along with circumscribed neoplasm composed of sheets of mononuclear cells interspersed with osteoclastic giant cells, with no evidence of atypia or mitosis – concluding the diagnosis to be that of a Giant cell tumor. The patient has been on regular follow-up for the past 2 years and there have been no recurrences.
The tissue specimen (Fig. 8) was sent for culture- sensitivity and histopathology. Fungal culture and KOH mount were negative. Bacterial culture was negative. Histopathology biopsy report revealed–tendinous tissue along with circumscribed neoplasm composed of sheets of mononuclear cells interspersed with osteoclastic giant cells, with no evidence of atypia or mitosis – concluding the diagnosis to be that of a Giant cell tumor. The patient has been on regular follow-up for the past 2 years and there have been no recurrences.
Ganglions are the most common soft-tissue masses of the hand and wrist typically measuring 1–2 cm in size and either single or multiloculated. They may form suddenly or develop gradually. Ganglions are thought to arise when repetitive microtrauma to the capsular and ligamentous structures of the joint stimulate fibroblasts at the synovialecapsule interface to produce hyaluronic acid-forming a highly viscous fluid that pools in the ganglion [4]. GCT of bone is generally a benign tumor composed of mononuclear stromal cells and characteristic multinucleated giant cells that exhibit osteoclastic activity. Reactive or regenerative hyperplasia accompanied by an inflammatory process has been the most commonly accepted theory for GCTTS [1]. Diagnostic workup includes patient history and a detailed physical examination. Their variable clinical presentation is related to variations in site and progression [5]. Plain radiographs can be helpful since GCTTS may produce erosions in the cortical bone and may invade medullary space, which a rarity. The typical appearance is a lytic lesion with a well-defined but non-sclerotic margin that is eccentric in location, extends near the articular surface [6]. MRI is the most useful diagnostic tool and is also required for surgical planning [1]. GCTTS with bone invasion should be considered when MRI shows solid mass with characteristic low signal on T2-weighted images [7]. The current standard treatment of choice for GCTTS is simple excision. The main concern about the treatment is the high recurrence rates, ranging from 15 to 45% as reported by several studies. Incomplete excision is widely accepted as a definitive risk factor. Open surgical excision offers significantly lower chance of recurrence compared with aspiration in the treatment of wrist ganglions [4]. Cortical destruction, location at the interphalangeal joint of the thumb and distal interphalangeal joints, presence of degenerative joint disease, Type 2 tumors, tumors with increased mitotic activity, and neurovascular dissection during removal and incomplete excision constitute risk factors favoring recurrence [1]. He et al. had reported a similar case report of a giant cell tumor of the tendon sheath with the involvement of tarsal bones and intertarsal joint. Higher imaging in the form of CT and MRI was done to further diagnose and evaluate the quality and range of tumor. Patient was treated with surgical excision of the tumor and had returned to an asymptomatic walk in 3 months [2]. In our peculiar case, we had clinically and radiologically suspected it to be a case of a recurrent ganglion cyst with associated osteomyelitis. As per the standard guidelines of management of a ganglion cyst, we had decided to excise the lesion in-toto. Intraoperatively, there was an intraosseous extension of the lesion into the cortices of capitate and hamate – which is uncommon in a case of GCTTS or a ganglion cyst. The tissue diagnosis was in favor of a Giant cell tumor. The patient has been on regular follow-up for the past 2 years and no recurrences have been reported till date [Fig. 9-11].
“Once a ganglion, always a ganglion” should not be taken as the Gospel truth. Histopathological diagnosis continues to remain as the gold standard, especially in cases of soft-tissue swellings of the hand. Correlation and integration of clinical features, imaging modalities, and histopathological diagnosis are the cornerstone in the management of GCTTS.
Corroboration of presenting history, clinical acumen, and intraoperative exploration along with histopathological diagnosis are the linchpin of evidence based medicine and in extrapolation, the surgical management of soft-tissue swellings of the hand.
References
- 1.Ozben H, Coskun T. Giant cell tumor of tendon sheath in the hand: Analysis of risk factors for recurrence in 50 cases. BMC Musculoskelet Disord 2019;20:457. [Google Scholar | PubMed]
- 2.He QF, Bian ZY, Xiang JJ, Zhu LL. Giant cell tumor of tendon sheath with tarsal bones and intertarsal joint invasion: A case report. J Am Podiatr Med Assoc 2020;110:15. [Google Scholar | PubMed]
- 3.Raskin KA, Schwab JH, Mankin HJ, Springfield DS, Hornicek FJ. Giant cell tumor of bone. J Am Acad Orthop Surg 2013;21:118-26. [Google Scholar | PubMed]
- 4.Head L, Gencarelli JR, Allen M, Boyd KU. Wrist ganglion treatment: Systematic review and meta-analysis. J Hand Surg Am 2015;40:546-53.e8. [Google Scholar | PubMed]
- 5.Gouin F, Noailles T. Localized and diffuse forms of tenosynovial giant cell tumor (formerly giant cell tumor of the tendon sheath and pigmented villonodular synovitis). Orthop Traumatol Surg Res 2017;103:S91-7. [Google Scholar | PubMed]
- 6.Chakarun CJ, Forrester DM, Gottsegen CJ, Patel DB, White EA, Matcuk GR Jr. Giant cell tumor of bone: Review, mimics, and new developments in treatment. Radiographics 2013;33:197-211. [Google Scholar | PubMed]
- 7.Wang CS, Duan Q, Xue YJ, Huang XM, Wang LL, Chen ZY, et al. Giant cell tumour of tendon sheath with bone invasion in extremities: Analysis of clinical and imaging findings. Radiol Med 2015;120:745-52. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series
August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report
July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series
July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature
June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature