
Ceftazidime-avibactam/aztreonam combination has been shown to be useful in the management of carbapenem-resistant Klebsiella pneumoniae-induced bone and soft-tissue infections.
Dr. Akshat Gupta, Department of Orthopaedics, All India Institute of Medical Sciences, Rajkot, Gujarat, India. E-mail: drguptaakshat@gmail.com
Abstract
Introduction: Osteomyelitis secondary to multi-drug resistant (MDR) gram-negative bacteria (GNB), especially carbapenem-resistant Klebsiella pneumoniae (CRKP), is a rare occurrence. These are difficult-to-treat microorganisms, and their presence within the host bone tissue makes them inherently resistant to most standard antimicrobials. Although a number of drugs have been described in the literature, there are no standardised guidelines as to the ideal drug of choice effective against CRKP-induced bone and joint infections (BJIs). In this context, we have described our experience in treating three cases of CRKP osteomyelitis secondary to an open fracture, who presented to us following a road traffic accident (RTA).
Case Report: Three patients of polytrauma presented to the emergency room of a tertiary care institute following RTA. All of them were primarily resuscitated, following which fixation of the fractures was undertaken. In the post-operative period, surgical site infection was seen in all three at specific locations. These were thoroughly debrided, and intraoperative samples were sent for culture analyses. The latter revealed isolates of CRKP. Accordingly, a multidisciplinary approach was followed, combining inputs from the surgical team and clinical microbiologist, as well as an infectious disease specialist. Infected implants were removed, and a plastic surgery consult was sought for wound coverage. Ceftazidime-Avibactam (CAZ-AVI) in conjunction with Aztreonam (ATM) was started after synergy testing. This was continued for a duration of 4–6 weeks. In two patients, the fracture had successfully united, whereas in one, a definitive fixation is still pending. Soft-tissue envelope healing was achieved in all cases. No adverse effects were reported.
Conclusion: Cases of BJI secondary to CRKP necessitate a combined approach which includes prompt surgical debridement with/without implant removal and culture-specific antimicrobial therapy. Although experience is limited, the CAZ-AVI/ATM combination has shown promising results.
Keywords: Carbapenem-resistant Klebsiella pneumoniae, multidrug-resistant Gram-negative bacteria, osteomyelitis, ceftazidime-avibactam/aztreonam.
Bone and joint infections (BJIs) are one of the most challenging problems faced by orthopaedic surgeons. The key to successful management is a multidisciplinary approach with timely diagnosis, appropriate surgical treatment, and microbe-specific antibiotic therapy. While Staphylococcus aureus is the most commonly implicated micro-organism in osteomyelitis, the incidence of multidrug-resistant (MDR) Enterobacteriaceae, particularly carbapenem-resistant Klebsiella pneumoniae (CRKP), is on the rise [1,2]. Although rare, these represent a major public health problem and are associated with significant morbidity and mortality [3,4]. A number of antibiotic therapies have been described for the management of CRKP-induced BJIs [5,6,7]. Out of these, β-lactamase inhibitor combinations such as Ceftazidime-Avibactam (CAZ-AVI) or Aztreonam-Avibactam (ATM-AVI) constitute a newer class of antibiotics that have shown promising results in in-vitro models [6,8,9]. While individual reports/case series exist documenting the efficacy of CAZ-AVI alone or in combination with ATM in treating CRKP-induced osteomyelitis, there are no large-scale prospective studies for the same [10,11,12,13,14,15]. ATM-AVI, on the other hand, is yet to be approved by the United States Food and Drug Administration (U.S. FDA) for use in BJIs [5,13]. Due to a lack of standardised treatment guidelines, we have described our own experience in successfully managing three cases of BJI secondary to CRKP in a tertiary care centre of Western India.
Case 1:
A forty-seven-year-old male presented to the emergency room (ER) with an alleged history of a roadad traffic accident (RTA) 2 days back. The patient was diagnosed with an open grade IIIB fracture of the distal 1/3rd right femur with an associated fracture in the ipsilateral shaft of the tibia (Fig. 1a, b, c). There was accompanying internal degloving of the skin and subcutaneous tissue over the anteromedial aspect of the right thigh (Fig. 1d). The patient was taken up for emergency surgery and underwent debridement of the degloved area along with open reduction internal fixation (ORIF) (for femur) as well as closed reduction internal fixation (for tibia) (Fig. 1e, f, g). On the 4th post-operative day, purulent discharge was noted from the raw area over the thigh. This was accompanied by intermittent febrile episodes (temperature >101°F),evated total leucocyte counts (TLC = 16010/µL) and raised serum erythrocyte sedimentation rates (ESR = 105 mm/h) as well as highly sensitive C-reactive protein (hs-CRP = 202 mg/L). The patientient was taken up for re-debridement and freshening of the skin margins (Fig. 1h). However, in the immediate postoperativeperiod, his condition further deteriorated,, with TLC, ESR, and hs-CRP spiking to 21000/µL, 134 mm/h, and 287.7 mg/L. Ultrasonography (USG) showed a small echogenic collection in the right knee. As a result, the patient underwent surgical exploration and evacuation of the collection. Intra-operatively,, tissue samples were found to be positive for CRKP. Antibiotic sensitivity testing was done using the VITEK®2 automated analyser (BioMérieux, France) and revealed sensitivity only to colistin (intermediate sensitivity MIC <0.5 mcg/mL) and tigecycline (sensitive MIC <0.5 mcg/mL). Synergy testing showed affirmative results with the CAZ-AVI-AVI and ATM combination. The patient was started on intravenous antibiotics – CAZ-AVIVI and ATM – – at the dosage of 2.5 g q8h and 2 g q8hh for a total of 4 weeks. The raw raw area over the thigh was covered with a free anterolateral thigh flap. At 12 months follow-up, the patient has a healthy wound and can ambulate freely.
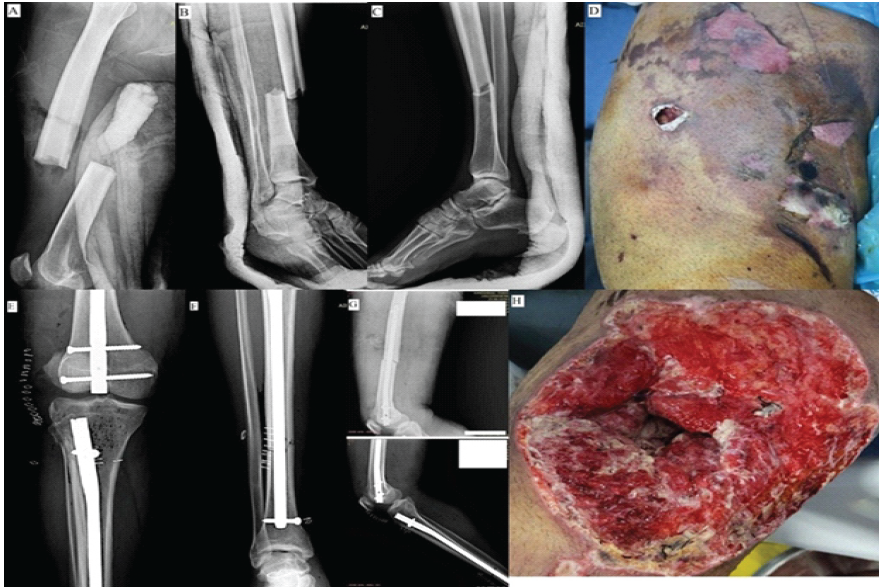
Figure 1: (a, b, c) Pre-operative X-rays; (d) Clinical representation of the injured thigh at the time of presentation; (e, f, g) Immediate post-operative X-rays; (h) Thigh wound following debridement (post-operative day 5).
Case 2:
A twenty-nine-year-old male patient suffered an RTARTA and was diagnosed with an open Grade IIIA fracture of the right mid-shaft femur, along with an open Grade IIIB fracture of the right proximal tibial shaft (segmental). He was initially operated on at the primary hospital of presentation and underwent ORIF using an interlocking nail for the femur and external fixation for the tibia (Fig. 2a, b, c). However, from post-operative day 2, an active wound discharge was noted over the anterior aspect of the leg. Lab parameters showed the following values: TLC – 18250/µL; ESR – 100 mm/h; and hs-CRP – 233.9 mg/L. The patient was subsequently referred to our institute, where he underwent debridement of the tibial wound as well as fixator re-application. An additional injury was detected over the right tibial plateau, which was fixed using two 6.0 mm cannulated cancellous screws (Fig. 2d and e).
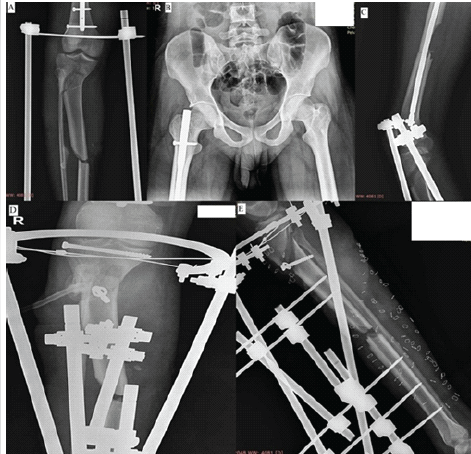
Figure 2: (a, b, c) X-rays of the patient at the time of hospital admission; (d and e) Immediate post-operative X-rays.
Intraoperative tissue samples were cultured and found to be positive for MDR K. pneumoniae. The latter showed sensitivity to only Tigecycline (MIC = 1 mcg/mL) and Colistin (MIC < 0.5 mcg/mL) (intermediate sensitivity), as well as the CAZ-AVI/ATM combination (positive synergy testing using the disc diffusion method). The case was discussed with an infectious disease specialist, and accordingly, the patient was started on intravenous CAZ-AVI 2.5g q8h + ATM 2g q8h for a total of 6 weeks. A plastic surgery review was done for the tibial wound defect (Fig. 3a, b, c, d, e, f, g). This involved coverage with a lateral gastrocnemius flap for the middle third and a medial gastrocnemius flap + split skin grafting for the upper third leg wound with implant (Fig. 3a, b, c, d, e, f, g). After 6 weeks, the patient underwent fixator removal, and antibiotics were stopped. At the 12-month follow-up, the patient is afebrile, has a completely healed soft-tissue coverage, and is planned for a definite tibial fixation.

Figure 3: (a, b, c, d) Intraoperative images of the tibial defect showing exposed bone and the (e, f, g) final wound status at 9 months follow-up.
Case 3:
A thirty-five-year-old victim of polytrauma presented to the ER following RTA. He was diagnosed with several bony injuries to the upper and lower limbs (Fig. 4a, b, c, d, e, f, g, h).

Figure 4: (a, b, c, d, e) Pre-operative radiographs showing fractures of the distal femur, elbow, ankle, and the foot; (f) Thigh wound at presentation; (g and h) Lacerations and degloving injuries of the foot area.
After initial resuscitation, all open fractures were copiously irrigated and splinted. Broad-spectrum antibiotics and tetanus prophylaxis were given. After stabilisation in the ER, the patient underwent staged fixation of the bony injuries. This involved the application of a knee-spanning external fixator frame to support the distal femur. The latter was switched to a locking plate after 3 weeks (Fig. 5a, b, c, d, e, f, g, h). On postoperative day 2 following ORIF, the patient developed fever spikes (temperature >100°F) with TLC, ESR, and hs-CRP documented at 13,800/µL, 105 mm/h, and 294 mg/L, respectively. USG revealed an echogenic collection at the operative site. As a result, debridement and lavage of the surgical site were carried out, followed by plate removal and fixator re-application (Fig. 5i). Samples sent intra-operatively for microbiological analyses revealed growth of MDR K. pneumoniae by the VITEK®2 automated analyser (BioMérieux, France). Intermediate and complete sensitivity was noted to colistin (MIC <0.5 mcg/mL) and tigecycline (MIC <0.5 mcg/mL), while CAZ-AVI and ATM showed positive synergy. After discussion with an infectious disease specialist, the patient was started on a 4-week course of IV CAZ-AVI (2.5 g q8h) + ATM (2 g q8h). Raw areas over the foot and thigh were treated with regular dressings as per the plastic surgeon’s advice. After 1 month, the patient’s infection had settled, and the raw areas healed (Fig. 5j, k, l). TLC had returned to normal limits (6000/µL) and inflammatory markers to their baseline values (ESR – 34 mm/h and hs-CRP – 14 mg/L). The patient was planned for definite distal femur fixation. However, he refused to undergo an additional surgical procedure, and hence, the injury was managed conservatively with a thigh splint. At 12 months follow-up, all fractures had united, and the patient is able to ambulate without support.
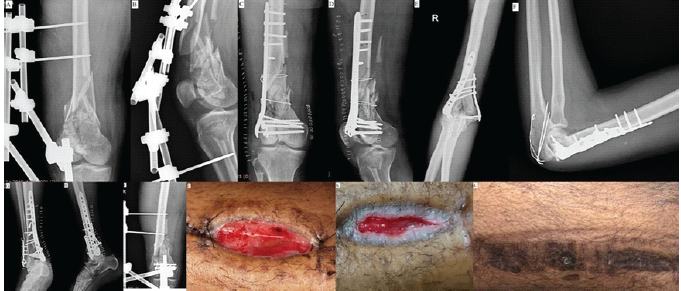
Figure 5: (a, b, c, d, e, f, g, h, i) Radiographs showing sequence of fixation of all bony injuries; (j, i, k, l) clinical images showing progressive healing of the infected thigh wound.
The frequency of Gram-negative bacteria (GNB)-induced osteomyelitis and prosthetic joint infections (PJIs) is approximately 10% [9,16]. Out of these, the most commonly implicated microorganisms are Acinetobacter baumannii, Klebsiella spp., Pseudomonas aeruginosa, Enterococcus faecium, Enterobacter spp., etc. Antimicrobial resistance in these microbes is broadly categorised into three types: (i) multidrug resistant if not susceptible to at least one agent in >3 antimicrobial classes; (ii) extensively drug resistant if non-susceptible to at least one agent in all but <2 antimicrobial categories; and (iii) pan-drug resistant if not susceptible to any antimicrobial agent across all categories [17]. Although carbapenems constitute high-end antibiotics, their resistance in intensive care units in the Indian subcontinent has reached an alarming 12–83% [5]. These β-lactamases include the Ambler class A (KPC enzymes), class B (metallo-carbapenemase enzymes/MBLs such as NDM, IMP), and class C (AmpC β-lactamases), as well as class D (oxacillinase enzymes like OXA-48) enzymes [5,6,9]. Mortality in CRKP-induced infections can range from 22 to 70%, with higher rates reported in patients with associated comorbidities [6,18]. Timely detection of these agents, hence, is crucial to initiating microbe-specific antibiotic therapy and ensuring clinical cure. BJIs are notorious for their complexity and pose significant treatment challenges. The main reasons for the same are (i) biofilm formation and (ii) poor rates of antibiotic diffusion into host tissue [6,9]. In vitro models suggest that the low concentration of oxygen and nutrients in the biofilm environment is probably responsible for the phenotypic changes within the bacteria, leading to antibacterial tolerance [19]. Different categories of antibiotics are, therefore, recommended to be used in combination for combating CRE infections. These mainly include carbapenems, meropenem-vaborbactam (MER-VAB), imipenem-cilastatin-relebactam (IMI-REL), ceftolozane-tazobactam, CAZ-AVI, cefiderocol, fosfomycin, tigecycline, and colistin [6,20,21]. Carbapenems have the broadest spectrum of antimicrobial activity and possess a favourable pharmacokinetic profile vis-à-vis bone infections. However, they are ineffective against carbapenemase-producing K. pneumoniae, even when combined with colistin [6]. MER-VAB and IMI-REL are newly introduced carbapenem-β-lactamase inhibitor combination drugs, which have been found to be effective against CRKPs (IMI-REL shows good response against P. aeruginosa also). However, they fail to combat MBLs as well as the OXA-48 category of enzymes. They are also ineffective against A. baumannii strains primarily resistant to MER and IMI [22]. Ceftolozane-Tazobactam is a fifth-generation cephalosporin combination with a β-lactamase inhibitor, which has shown promising results against extended-spectrum β-lactamase enzymes and some MDR strains of P. aeruginosa. Combined with colistin, the drug has demonstrated good anti-biofilm activity in in vitro models and can be used in meropenem-resistant cases [22]. CAZ-AVI was introduced in 2015 and is FDA approved for intra-abdominal infections, urinary tract infections, hospital-acquired pneumoniae, as well as BJIs. It is currently the only β-lactamase inhibitor combination having good activity against the OXA-48 category of enzymes [5,9,10,11,12,13,14,15,18,23]. The chief drawback is the limited effectiveness against MBLs such as NDM, which are quite prevalent in our part of the world. To offset this, ATM is usually added to CAZ-AVI, as the former has good activity against both OXA-48 as well as NDMs. A new combination – ATM-AVI – is currently under clinical trials [24,25]. Cefiderocol is a siderophore cephalosporin approved in 2019, which has shown broad coverage against most GNB, such as A. baumannii, Klebsiella spp., and P. aeruginosa, including activity against all four Ambler class β-lactamases. It has been cleared for use under limited treatment options [26]. There are no clear-cut guidelines on the choice, combination, or duration of antibiotic therapy for CRKP-induced BJIs. This is due to a lack of comparative randomised trials or large-scale cohort studies. However, the newer β-lactam/β-lactamase inhibitor class of drugs has shown promising results both in patients as well as in vitro models [5,6,9,10,24]. In our series, all patients first underwent a radical debridement of the infected tissues, with/without implant removal, following which broad-spectrum antibiotics were initiated. Once the culture report was affirmative for CRKP, the case was discussed in the infectious disease conference of the institute, and patients started on combination therapy. In all cases, the infection was successfully treated, and patients made a full recovery. We believe CAZ-AVI with ATM constitutes a reliable choice of antimicrobial when confronted with MDR GNB such as K. pneumoniae. Future trends call for blinded trials on the same to give more robust evidence. A summary of CRKPs reported thus far and how they compare with our study is given in Table 1.
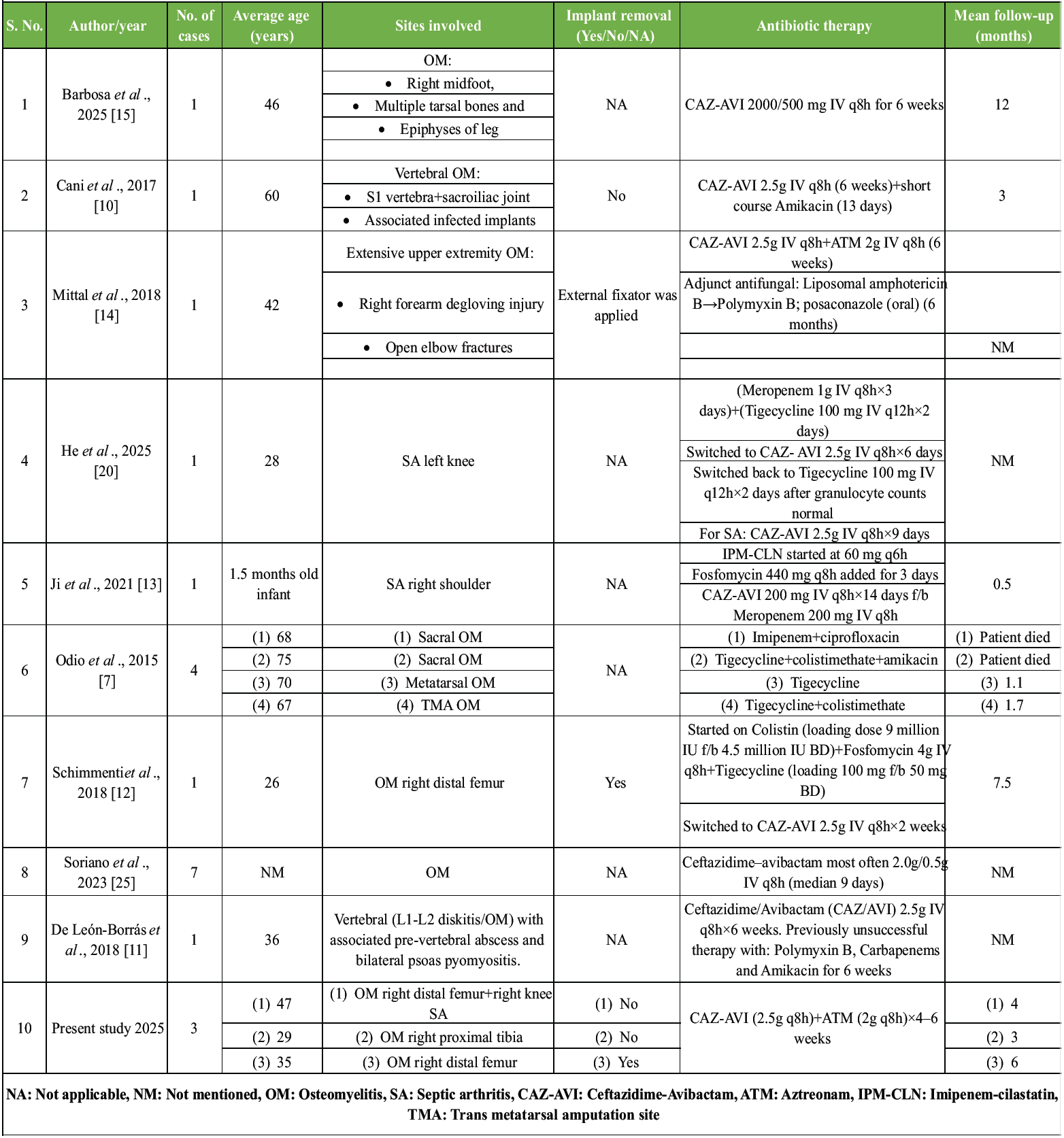
Table 1: A summary of all cases of Carbapenem-resistant Klebsiella pneumoniae-induced bone/joint infections and their management strategies
CRKPs represent a rare subset of MDR GNB, which are increasingly being implicated in BJIs. These require prompt surgical intervention, along with combination antimicrobial therapy. Although results may vary from case to case and the literature is still sparse, CAZ-AVI/ATM for a duration of 4–6 weeks has shown promising results.
A multidisciplinary approach is warranted in all cases of MDR pyogenic osteomyelitis. Thorough surgical debridement, judicious fracture stabilization, and combination culture-sensitive antibiotic therapy are the mainstays to ensure optimal response. For cases afflicted with CRKPs, CAZ-AVI/ATM combination has been shown to be reliable.
References
- 1. McNeil JC. Acute hematogenous osteomyelitis in children: Clinical presentation and management. Infect Drug Resist 2020;13:4459-73. [Google Scholar] [PubMed]
- 2. Yan J, Pu S, Jia X, Xu X, Yang S, Shi J, et al. Multidrug resistance mechanisms of carbapenem resistant Klebsiella pneumoniae strains isolated in chongqing, China. Ann Lab Med 2017;37:398-407. [Google Scholar] [PubMed]
- 3. Akova M, Daikos GL, Tzouvelekis L, Carmeli Y. Interventional strategies and current clinical experience with carbapenemase-producing gram-negative bacteria. Clin Microbiol Infect 2012;18:439-48. [Google Scholar] [PubMed]
- 4. Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 2013. Atlanta: CDC, 2013. Available from: https://www.cdc.gov/drugresistance/threat-report-2013/pdf/arthreats-2013-508.pdf [Last accessed on 15 Jan 2026]. [Google Scholar] [PubMed]
- 5. Nagvekar V, Shah A, Unadkat VP, Chavan A, Kohli R, Hodgar S, et al. Clinical outcome of patients on ceftazidime-avibactam and combination therapy in carbapenem-resistant enterobacteriaceae. Indian J Crit Care Med 2021;25:780-4. [Google Scholar] [PubMed]
- 6. Tsilika M, Ntziora F, Giannitsioti E. Antimicrobial treatment options for multidrug resistant gram-negative pathogens in bone and joint infections. Pathogens 2025;14:130. [Google Scholar] [PubMed]
- 7. Odio CD, Van Duin D, Cober E, Teixeira-Johnson L, Schmitt S, De Sanctis J. Carbapenem-resistant Klebsiella pneumoniae osteomyelitis and soft tissue infections: A descriptive case series. J Infect Dis Ther 2015;3:1. [Google Scholar] [PubMed]
- 8. Wei J, Zou C, Wang D, Huang A, Niu S. Genetic diversity and in vitro activity of ceftazidime/avibactam and aztreonam/avibactam against imipenem-resistant enterobacteriaceae isolates in Southwest China: A single-centre study. J Glob Antimicrob Resist 2020;22:448-51. [Google Scholar] [PubMed]
- 9. Davido B, Crémieux AC, Vaugier I, Gatin L, Noussair L, Massias L, et al. Efficacy of ceftazidime-avibactam in various combinations for the treatment of experimental osteomyelitis due to Klebsiella pneumoniae carbapenemase (KPC)-producing Klebsiella pneumoniae. Int J Antimicrob Agents 2023;61:106702. [Google Scholar] [PubMed]
- 10. Cani E, Moussavi F, Ocheretyaner E, Sharma R, Brown C, Eilertson B. Carbapenem-resistant Klebsiella pneumoniae vertebral osteomyelitis in a renal transplant recipient treated with ceftazidime-avibactam. Transpl Infect Dis 2018;20:e12837. [Google Scholar] [PubMed]
- 11. De León-Borrás R, Álvarez-Cardona J, Vidal JA, Guiot HM. Ceftazidime/avibactam for refractory bacteremia, vertebral diskitis/osteomyelitis with pre-vertebral abscess and bilateral psoas pyomyositis secondary to Klebsiella Pneumoniae carbapenemase-producing bacteria (KPC). P R Health Sci J 2018;37:128-31. [Google Scholar] [PubMed]
- 12. Schimmenti A, Brunetti E, Seminari E, Mariani B, Cambieri P, Orsolini P. Prosthetic Joint Infection from carbapenemase-resistant Klebsiella pneumoniae successfully treated with ceftazidime-avibactam. Case Rep Infect Dis 2018;2018:1854805. [Google Scholar] [PubMed]
- 13. Ji Z, Sun K, Li Z, Cheng W, Yang J. Carbapenem-Resistant Klebsiella pneumoniae osteomyelitis treated with ceftazidime-avibactam in an infant: A case report. Infect Drug Resist 2021;14:3109-13. [Google Scholar] [PubMed]
- 14. Mittal J, Szymczak WA, Guo Y, Levi MH, Chen L, Kreiswirth BN, et al. Two for the price of one: Emerging carbapenemases in a returning traveller to New York City. Case Rep 2018;2018:bcr2018225440. [Google Scholar] [PubMed]
- 15. Barbosa R, Garrido S, Costa L, Carvalho R. Medical treatment of osteomyelitis due to carbapenemase-producing Klebsiella pneumoniae in diabetes-related foot disease. Acta Med Port 2025;38:55-6. [Google Scholar] [PubMed]
- 16. Titécat M, Senneville E, Wallet F, Dezèque H, Migaud H, Courcol RJ, et al. Bacterial epidemiology of osteoarticular infections in a referent center: 10-Year study. Orthop Traumatol Surg Res 2013;99:653-8. [Google Scholar] [PubMed]
- 17. Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012;18:268-81. [Google Scholar] [PubMed]
- 18. He M, Jiang Y, Wu H, Xu X, Jiang H. Disseminated organ and tissue infection secondary to carbapenem-resistant Klebsiella pneumoniae bloodstream infection for acute lymphoblastic leukemia treated with ceftazidime-avibactam: Two case reports. Medicine (Baltimore) 2025;104:e41195. [Google Scholar] [PubMed]
- 19. Lora-Tamayo J, Murillo O, Ariza J. Clinical use of colistin in biofilm-associated infections. Adv Exp Med Biol 2019;1145:181-95. [Google Scholar] [PubMed]
- 20. Petrosillo N, Taglietti F, Granata G. Treatment options for colistin resistant Klebsiella pneumoniae: Present and future. J Clin Med 2019;8:934. [Google Scholar] [PubMed]
- 21. Leanza C, Mascellino MT, Volpicelli L, Covino S, Falletta A, Cancelli F, et al. Real-world use of imipenem/cilastatin/relebactam for the treatment of KPC-producing Klebsiella pneumoniae complex and difficult-to-treat resistance (DTR) Pseudomonas aeruginosa infections: A single-center preliminary experience. Front Microbiol 2024;15:1432296. [Google Scholar] [PubMed]
- 22. Matlock A, Garcia JA, Moussavi K, Long B, Liang SY. Advances in novel antibiotics to treat multidrug-resistant gram-negative bacterial infections. Intern Emerg Med 2021;16:2231-41. [Google Scholar] [PubMed]
- 23. Soriano A, Montravers P, Bassetti M, Klyasova G, Daikos G, Irani P, et al. The use and effectiveness of ceftazidime-avibactam in real-world clinical practice: EZTEAM study. Infect Dis Ther 2023;12:891-917. [Google Scholar] [PubMed]
- 24. Taha R, Kader O, Shawky S, Rezk S. Ceftazidime-avibactam plus aztreonam synergistic combination tested against carbapenem-resistant enterobacterales characterized phenotypically and genotypically: A glimmer of hope. Ann Clin Microbiol Antimicrob 2023;22:21. [Google Scholar] [PubMed]
- 25. Karaiskos I, Galani I, Souli M, Giamarellou H. Novel β-lactam-β-lactamase inhibitor combinations: Expectations for the treatment of carbapenem-resistant Gram-negative pathogens. Expert Opin Drug Metab Toxicol 2019;15:133-49. [Google Scholar] [PubMed]
- 26. Zhanel GG, Golden AR, Zelenitsky S, Wiebe K, Lawrence CK, Adam HJ, et al. Cefiderocol: A siderophore cephalosporin with activity against carbapenem-resistant and multidrug-resistant gram-negative Bacilli. Drugs 2019;79:271-89. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series
August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report
July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series
July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series- May 1, 2026 Tibial Osteomyelitis due to Burkholderia pseudomallei in a Non-diabetic Patient: A Case Report