
Chondromyxoid Fibroma are rare benign tumors that infrequently affect flat bones such as ribs. Histopathological examination is important to differentiate from other benign lesions. In ribs enblock resection is the mainstay of treatment.
Dr. Mantu Jain, Department of Orthopedics, AIIMS, Bhubaneswar, Odisha, India. E-mail: montu_jn@yahoo.com
Abstract
Introduction: Chondromyxoid fibroma (CMF) is an uncommon bone tumor, accounting for <1% of all bone tumors. It generally affects the metaphysis of the long bone of the lower limb and seldom involves the small bones, but the involvement of the flat bones, like ribs, is infrequent.
Case Report: A teenage girl complained of pain on the right side of the chest for the past 6 months, dull aching, and persistent without any diurnal variation. The chest X-ray examination showed a nodular, hyperdense lesion on the lateral chest wall near the 5–7th rib on the right side. A computed tomography scan confirmed the lesion from the sixth rib with ground-glass matrix and cortical thinning with a smooth margin, without any soft-tissue involvement. An enblock excision of the lesion was done. Histopathological studies showed a well-circumscribed tumor with reactive bone formation at the periphery with lobules of chondromyxoid tissue separated by spindle cells and stellate-shaped cells suggestive of CMF. At 1-year follow-up, she is asymptomatic without any recurrence.
Conclusion: CMFs are rare benign tumors that require histopathological study to differentiate from other benign lesions of the bone. In flat tubular bones like the ribs, enblock resection is the mainstay of treatment.
Keywords: Chondromyxoid fibroma, rib, excision.
Chondromyxoid fibroma (CMF) is a very uncommon bone tumor of cartilaginous origin accounting for <1% of all bone tumors [1]. The males are affected slightly more commonly than females, usually in affect the second and third decade of life [2]. It generally affects the metaphysis of long bones of a lower limb and seldom involves the small bones. However, the involvement of the flat bones like ribs is infrequent [2,3,4].
A teenage female patient presented to our outpatient department with complaints of pain on the right side of the chest for 6 months. The pain was a dull aching, mild in intensity without any diurnal variation. She had no visible swelling in the chest and elsewhere in the body. Physical examination revealed mild tenderness on the lateral aspect of the sixth rib. Her blood investigation, including the inflammatory markers, was within the standard limit. The chest X-ray examination showed a nodular, hyperdense lesion on the lateral chest wall near the 5–7th rib on the right side (Fig. 1a). The lesion was confirmed to be 4.4 × 3.9 × 2.7 cm, arising from the sixth rib with ground-glass matrix and cortical thinning with smooth margin, without any soft-tissue involvement on the computed tomography scan (Fig. 1b).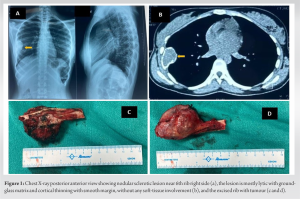 Fine-needle aspiration and cytology were done, which displayed mostly benign spindle cells. After taking informed consent, enblock excision of the lesion was done (Fig. 1c and d), and excised part was sent for histopathological examination. The histopathological study showed a well-circumscribed tumor with reactive bone formation at the periphery (Fig. 2a) with lobules of chondromyxoid tissue separated by spindle cells (Fig. 2b) and stellate-shaped cells (Fig. 2c). The intervening spindle cell showed monomorphic oval to spindle nuclei without any atypia, mitosis, or necrosis (Fig. 2d). The post-operative period was uneventful, and she was discharged on the 7th day. She was doing fine at her last follow-up at 1 year.
Fine-needle aspiration and cytology were done, which displayed mostly benign spindle cells. After taking informed consent, enblock excision of the lesion was done (Fig. 1c and d), and excised part was sent for histopathological examination. The histopathological study showed a well-circumscribed tumor with reactive bone formation at the periphery (Fig. 2a) with lobules of chondromyxoid tissue separated by spindle cells (Fig. 2b) and stellate-shaped cells (Fig. 2c). The intervening spindle cell showed monomorphic oval to spindle nuclei without any atypia, mitosis, or necrosis (Fig. 2d). The post-operative period was uneventful, and she was discharged on the 7th day. She was doing fine at her last follow-up at 1 year.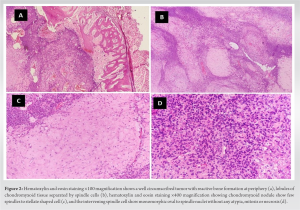
Clinically, CMF is symptomatic and diagnosed incidentally radiographically [5]. Sometimes the presentation can be associated with variables such as pain, swelling, restriction of movement, or pathological fracture. Pain is usually mild, intermittent, and dull aching type. The typical radiographic appearance of the tumor is a lytic, oval, and eccentric metaphyseal lesion with a long axis parallel to the bone having a sclerotic rim without calcification [6]. The form in the flat bones is atypical as the lesion extends throughout the entire diameter of the affected bone, expanding both surfaces and often making diagnosis difficult [7]. Magnetic resonance imaging can help delineate the extent of the disease [8]. A tissue biopsy will confirm the diagnosis [9]. Typical features of CMF will show lobules of spindle-shaped or stellate cells spread among myxoid and chondroid matrix separated by zones of fibrous tissue without calcification [10]. Differential diagnosis includes chondroblastoma, enchondroma, low-grade chondrosarcoma, and aneurysmal bone cyst, which can be ruled out with the classical histopathological picture of CMF [2,5,11]. CMFs of the small bones are managed with simple curettage. Recurrence can be minimized with phenol application and sometimes enblock resection along with bone graft or PMMA (polymethylmethacrylate) application [12]. Armah et al. have excised the sole CMF in ribs in their 15 cases series [10]. Similarly, Long et al. reported a case where they did a surgical excision of the second rib [13]. Yamamoto et al. reported a case of exophytic soft-tissue attached to a CMF of a rib [14]. The authors did an intraoperative frozen mass biopsy and curettage and cauterization of the bone. A frozen biopsy is vital when eccentric CMF is associated with a soft-tissue component, as in their case. Radiotherapy is sometimes considered in case of unresectable tumors; however, it predisposes to the risk of post-radiation sarcoma [12]. Malignant transformation of CMFs is unusual and reported to be 1–2% [15].
CMFs are rare benign tumors that may be clinically and radiologically indistinct from other lesions. Therefore, a histopathological study is critical for the accurate diagnosis of CMF. In flat tubular bones like the ribs, enblock resection is the mainstay of treatment.
CMF is a rare benign tumorous lesion that affects mostly elderly males. Ribs are infrequent location of presentation. A thorough workup is necessary in such a situation to rule out other severe conditions which can mimic CMF.
References
- 1.Rahimi A, Beabout JW, Ivins JC, Dahlin DC. Chondromyxoid fibroma: A clinicopathologic study of 76 cases. Cancer 1972;30:726-36. [Google Scholar | PubMed]
- 2.Zillmer DA, Dorfman HD. Chondromyxoid fibroma of bone: Thirty-six cases with clinicopathologic correlation. Hum Pathol 1989;20:952-64. [Google Scholar | PubMed]
- 3.Giudici MA, Moser RP Jr., Kransdorf MJ. Cartilaginous bone tumors. Radiol Clin North Am 1993;31:237-59. [Google Scholar | PubMed]
- 4.Robbin MR, Murphey MD. Benign chondroid neoplasms of bone. Semin Musculoskelet Radiol 2000;4:45-58. [Google Scholar | PubMed]
- 5.Schajowicz F, Gallardo H. Chondromyxoid fibroma (fibromyxoid chondroma) of bone. A clinico-pathological study of thirty-two cases. J Bone Joint Surg Br 1971;53:198-216. [Google Scholar | PubMed]
- 6.Wilson AJ, Kyriakos M, Ackerman LV. Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-8. [Google Scholar | PubMed]
- 7.Feldman F, Hecht HL, Johnston AD. Chondromyxoid fibroma of bone. Radiology 1970;94:249-60. [Google Scholar | PubMed]
- 8.Scaglietti O, Stringa G. Myxoma of bone in childhood. J Bone Joint Surg Am 1961;43:67-80. [Google Scholar | PubMed]
- 9.Dey B, Deshpande AH, Brar RK, Ray A. Chondromyxoid fibroma of the metatarsal bone: A diagnosis using fine needle aspiration biopsy. J Cytol 2018;35:67-8. [Google Scholar | PubMed]
- 10.Armah HB, McGough RL, Goodman MA, Gollin SM, Surti U, Parwani AV, et al. Chondromyxoid fibroma of rib with a novel chromosomal translocation: A report of four additional cases at unusual sites. Diagn Pathol 2007;4:44. [Google Scholar | PubMed]
- 11.Gherlinzoni F, Rock M, Picci P. Chondromyxoid fibroma. The experience at the Istituto Ortopedico Rizzoli. J Bone Joint Surg Am 1983;65:198-204. [Google Scholar | PubMed]
- 12.Dürr HR, Lienemann A, Nerlich A, Stumpenhausen B, Refior HJ. Chondromyxoid fibroma of bone. Arch Orthop Trauma Surg 2000;120:42-7. [Google Scholar | PubMed]
- 13.Long KL, Absher KJ, Draus JM Jr. Chondromyxoid fibroma of the second rib. J Pediatr Surg 2013;48:1442-4. [Google Scholar | PubMed]
- 14.Yamamoto A, Takada K, Motoi T, Imamura T, Furui S. Chondromyxoid fibroma of the rib with prominent exophytic configuration. Jpn J Radiol 2012;30:81-5. [Google Scholar | PubMed]
- 15.Beggs IG, Stoker DJ. Chondromyxoid fibroma of bone. Clin Radiol 1982;33:671-9. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Chondromyxoid Fibroma of the Right Thumb: Successful Management with Wide Local Excision, Iliac Crest Bone Grafting and K-Wiring – A Rare Case Report
April 1, 2026 Chondromyxoid Fibroma of the Right Thumb: Successful Management with Wide Local Excision, Iliac Crest Bone Grafting and K-Wiring – A Rare Case Report August 1, 2025 A Case Report of a Rare Entity – Lateral End of Clavicle Chondromyxoid Fibroma which was Mistaken as Giant Cell Tumor and Aneurysmal Cyst
August 1, 2025 A Case Report of a Rare Entity – Lateral End of Clavicle Chondromyxoid Fibroma which was Mistaken as Giant Cell Tumor and Aneurysmal Cyst January 10, 2023 Late Presentation of Giant Osteochondroma of Talar Neck in Elderly: A Case Report and Review of Literature
January 10, 2023 Late Presentation of Giant Osteochondroma of Talar Neck in Elderly: A Case Report and Review of Literature January 10, 2023 Case Series – Osteochondromas at Rare Locations
January 10, 2023 Case Series – Osteochondromas at Rare Locations