
Rare case with possible mechanisms of injury and treatment options with clinical outcome.
Dr. Vishnu Senthil, Department of Orthopeadics, Government Royapettah Hospital, Chennai, Tamil Nadu, India. E-mail: vishnake@gmail.com
Introduction: Hoffa’s fracture is rare high velocity injuries. Bicondylar Hoffa is a rare fracture entity with only few reported cases.
Case Report: We report a case of open Type 3b non-conjoint bicondylar Hoffa fracture accompanied with ipsilateral anterior tibial spine avulsion and disruption of the patellar tendon. Staged procedure was done, first procedure included wound debridement with external fixator. Second procedure involved definitive fixation of Hoffa fracture, anterior tibial spine, and patellar tendon avulsion. In our case, we have discussed the possible mechanism of injury, operative approaches, and early functional outcome.
Conclusion: We report such a case with its possible etiological causation, surgical management, clinical outcome, and prognostic outcome.
Keywords: Hoffa fracture, bi-condylar, tibial spine avulsion, patellar tendon disruption, open injury.
Hoffa fracture due to distal femur coronal shear force was first described by Fredrich Busch in 1869 and the present name was coined after Albert Hoffa in 1904 [1]. Hoffa fractures remain an enigma because of its difficulty to be appreciated in plain X-rays and need further investigation to delineate the fracture pattern and manage them accordingly. Hoffa fractures commonly result from high velocity injuries involving a coronal shear of the posterior condyle of femur during knee flexion. We report of a case non-conjoint bi-condylar Hoffa fracture with anterior tibial spine avulsion and patellar tendon rupture from the tibial tuberosity. Such a combination of Injury has rarely been reported in English literature. We report such a case with its possible etiological causation, surgical management, clinical outcome, and prognostic outcome [2, 3, 4, 5].
A 20-year-old young male presented to the emergency department following road traffic accident and on probing the patient, he had fallen with a flexed knee leading to axial impaction of tibial condyle over the posterior femoral condyle. Patient had an open lacerated transverse wound about 7 cm over the anterior aspect of the knee. The distal end of femur was protruding out along the avulsion of patellar tendon from the insertion site. Clinical examination was not possible because of open wound and intense pain. There was no distal neurovascular deficit and patient was hemodynamically stable. Radiological examination of the involved knee included the anterior-posterior and oblique views (Fig. 1) showing patella alta, suggesting the patellar tendon avulsion with fracture of anterior tibial spine and lateral-oblique view showing non-conjoint bicondylar Hoffa fracture.  Initially, wound was debrided and an external fixator applied. The second procedure was taken after 2 days and both femoral condyles approached through the same open wound. The bicondylar Hoffa fracture was fixed with two 6.5 mm partially threaded cannulated cancellous screw. Screws were inserted from the non-articular portion of the femoral condyle on knee flexion. The anterior tibial spine fragment was fixed with 4.0 mm partially threaded cannulated cancellous screw and the patellar tendon avulsion was fixed to the tibia with ethibond trans-osseous suturing (Fig. 2). The wound was primarily closed without the need of additional soft-tissue procedures. The patient was kept in external fixator for 6 weeks in view of healing of the patellar tendon and soft tissue.
Initially, wound was debrided and an external fixator applied. The second procedure was taken after 2 days and both femoral condyles approached through the same open wound. The bicondylar Hoffa fracture was fixed with two 6.5 mm partially threaded cannulated cancellous screw. Screws were inserted from the non-articular portion of the femoral condyle on knee flexion. The anterior tibial spine fragment was fixed with 4.0 mm partially threaded cannulated cancellous screw and the patellar tendon avulsion was fixed to the tibia with ethibond trans-osseous suturing (Fig. 2). The wound was primarily closed without the need of additional soft-tissue procedures. The patient was kept in external fixator for 6 weeks in view of healing of the patellar tendon and soft tissue. After 6 weeks, the external fixator was removed and patient was started on partial weight bearing and guarded knee flexion was started in fear of patellar tendon re-rupture. At the end of 3 months, full weight bearing was started and knee Rom was from 5° to 40°. At the end of 6 months, knee flexion further improved to 35° (Fig. 3) with the healing of the fracture (Fig. 4).
After 6 weeks, the external fixator was removed and patient was started on partial weight bearing and guarded knee flexion was started in fear of patellar tendon re-rupture. At the end of 3 months, full weight bearing was started and knee Rom was from 5° to 40°. At the end of 6 months, knee flexion further improved to 35° (Fig. 3) with the healing of the fracture (Fig. 4).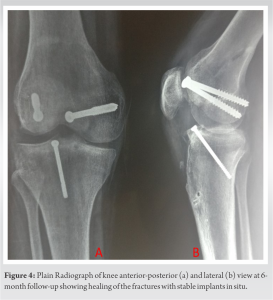
Hoffa fracture is partial articular distal femoral fractures involving a coronal split. Various case reports have described the probable mechanism of injury for this fracture and is commonly associated with high velocity trauma. Nork et al. [2] have reported that there is a 2.8 fold increase in Hoffa fracture following open injuries. This fracture occurs with a flexed knee, when the proximal tibia articular surface strikes the posterior condyle of femur accompanied twisting and shearing forces. During impact, the ground reaction force travels through the tibial plateau to the posterior femoral condyle with axial compression causing the fracture pattern. The lateral femoral condyle is more commonly involved because of the physiological valgus orientation leading to earlier tibiofemoral contact compared to the medial condyle. In bicondylar Hoffa fracture, force is directed in a posterior and upward direction without varus or valgus component. The fracture line and its obliquity is decided on the degree of flexion of knee while impact. Increasing knee flexion increases the distance between the fracture line and posterior condyle. The mechanism of injury in our case was identical with other case reports, resulting in a non-conjoint bicondylar fragment in a flexed knee as compared to Ul Haq et al. [6], where the mechanism of injury was due to semi-flexed knee impinging on the posterior femoral condyle leading to a bridge of bone between them. In our case, considering the magnitude of trauma and the probable explanation for the above injuries is that in initial degree of flexion patellar tendon could have ruptured/avulsed from the tibial tuberosity with continuing flexion of knee non-conjoint bicondylar Hoffa fracture, tibial spine avulsion, and open injury forcing the femoral condyles out of the knee wound could have occurred. The authors from various case reports have suggested that 40% of the fractures are overlooked in plain X-rays and most of them are missed in the anterior-posterior views because of the intact anterior part of the femoral condyle. In lateral view X-ray when fracture fragment is displaced, it is difficult appreciate the fracture line or involvement of the medial or lateral femoral condyle. Oblique X-rays have an important role in the pre-operative and intraoperative evaluation of reduction, screw length and identification of the involved condyle. CT with 3D reconstruction is the investigation of choice which is needed to outline the fracture in most of the cases since it involves the coronal portion of the posterior femoral condyle. Our case had an open fracture which needed debridement in emergency and fracture pattern was known intraoperatively; hence, routine X-rays were done. Surgical management is the mainstay of treatment because the fracture is intrinsically unstable due to articular surface involvement and continual of shear forces in both coronal and sagittal planes [7]. Non-operative treatment in the form of plaster cast or skeletal traction leads to loss of extension, non-union, instability, joint contracture, and early deformity. Hoffa’s fractures are commonly approached through midline, medial, or lateral approaches with or without ancillary procedures like Gerdy’s tubercle osteotomy [8] to enhance the exposure (Table 1). It shows the various approaches described in various case reports. Swashbuckler (modified anterior approach) advocated by Dua and Shamshery [9] allowed adequate exposure of both condyles and bicondylar Hoffa fracture could be managed anatomically with a single incision. The importance of a single incision in closed fractures is that it would result in lesser trauma to the quadriceps muscle, lesser fibrosis, and early return of function of quadriceps muscle. Hoffa’s fracture is commonly classified according to the AO classification Ul Haq et al. [6], classified B3.3 (Hoffa fracture) into two groups: B3.3a – conjoint bicondylar Hoffa fracture where the two condyles are joined by a bridge of intact bone which occurs due to a semi-flexed knee without any varus or valgus during impact. B3.3b – Non-conjoint bicondylar Hoffa fracture where the both condyles are separated from each other which occur due to increased knee flexion during impact. However, the above classification needs validation since only a few cases have been reported. Meyers and Mc Keevers have classified tibial spine fractures. Our patient had Type III Meyers and Mc Keevers for intercondylar tibial eminence fracture. Hoffa’s fracture need an accurate open reduction and internal fixation with <3 mm step or articular displacement. There is still not a consensus on the fixation methods, whether screws are to be directed anterior-posterior or posterior-anterior, number of screws, and surgical approach. Two or more screws are used to prevent rotational instability. In our case, we have used minimal screws in view of open injury to prevent infection. Jarit et al. suggested that posterior to anterior screw is more biomechanically stable than AP screw but PA screw insertion is more risky and difficult to perform. Partially threaded cannulated cancellous screws 6.5 mm or 4 mm are preferred to achieve compression and can be supplemented with anti-glide plates in osteoporotic bones. Mobilization is started early only when fracture fixation is stable. In our case, we decided to immobilize with external fixator in extension for 6 weeks till the soft tissues healed and also allowing time for patellar tendon and fracture healing. Immobilization in extension was preferred to allow healing of the repaired patellar tendon and allowing the posterior capsule to form a splint for the Hoffa fragment. We started knee mobilization and weight bearing gently to avoid the fixation becoming unstable (Table 1) describes the bicondylar femur fractures published by the previous authors.
We report of a case of non-conjoint bicondylar Hoffa fracture with associated tibial spine avulsion and patellar tendon avulsion. The possible mechanism of injury, fixation method, and the rehabilitation with early outcome has been described in our report. To our best of knowledge, such a case has been rarely reported in the literature.
- Knowledge of Fracture pattern and management.
- Adequate Surgical Planning and good articular reduction is needed to avoid Long term complications and Morbidity.
References
- 1.Hoffa A. Lehrbuch der Frakturen und Luxationen. Stuttgart: Verlag Von Ferdinand Enke; 1904. p. 451. [Google Scholar]
- 2.Nork SE, Segina DN, Aflatoon K, Barei DP, Henley MB, Holt S, et al. The association between supracondylar-intercondylar distal femoral fractures and coronal plane fractures. J Bone Joint Surg Am 2005;87:564-9. [Google Scholar]
- 3.Zeebregts CJ, Zimmerman KW, Duis HJ. Operative treatment of a unilateral bicondylar fracture of the femur. Acta Chir Belg 2000;100:104-6. [Google Scholar]
- 4.Papadopoulos AX, Panagopoulos A, Karageorgos A, Tyllianakis M. Operative treatment of bilateral bicondylar Hoffa fractures. J Orthop Trauma 2004;18:119-22. [Google Scholar]
- 5.Calmet J, Mellado JM, Forcada IL, Giné J. Open bicondylar Hoffa fracture associated with extensor mechanism injury. J Orthop Trauma 2004;18:323-5. [Google Scholar]
- 6.Ul Haq R, Modi P, Dhammi IK, Jain AK, Mishra P. Conjoint bicondylar Hoffa fracture in an adult. Indian J Orthop 2013;47:302-6. [Google Scholar]
- 7.Meyer C, Enns P, Alt V, Pavlidis T, Kilian O, Schnettler R. Difficulties involved in the Hoffa fractures. Unfallchirurg 2004;107:15-21. [Google Scholar]
- 8.Liebergall M, Wilber JH, Mosheiff R, Segal D. Gerdy’s tubercle osteotomy for the treatment of coronal fractures of the lateral femoral condyle. J Orthop Trauma 2000;14:214-5. [Google Scholar]
- 9.Dua A, Shamshery PK. Bicondylar Hoffa fracture: Open reduction internal fixation using the swashbuckler approach. J Knee Surg 2010;23:21-3. [Google Scholar]
- 10.Neogi DS, Singh S, Yadav CS, Khan SA. Bicondylar Hoffa fracture a rarely occurring, commonly missed injury. Injury Extra 2008;39:296-86. [Google Scholar]
- 11.Lal H, Bansal P, Khare R, Mittal D. Conjoint bicondylar Hoffa fracture in a child: A rare variant treated by minimally invasive approach. J Orthop Traumatol 2011;12:111-4. [Google Scholar]
- 12.Bali K, Mootha AK, Krishnan V, Kumar V, Rawall S, Goni V. A rare case of bicondylar Hoffa fracture associated with ipsilateral tibial spine avulsion and extensor mechanism disruption. Chin J Traumatol 2011; 14:253-6. [Google Scholar]
- 13.Kondareddi V, Yalamanchili KR, Kiran RK. Bicondylar Hoffa’s fracture with patellar dislocation-a rare case. J Orthop Trauma 2014;5:38-41. [Google Scholar]
- 14.Mounasamy V, Hickerson L, Fehring K, Desai P. Open bicondylar Hoffa fracture with patella fracture: A case report and literature review. Eur J Orthop Surg Traumatol 2013;23 Suppl 2:S261-5. [Google Scholar]
- 15.Kini SG, Sharma M, Raman R. A rare case of open bicondylar Hoffa fracture with extensor mechanism disruption. BMJ Case Rep 2013;2013:bcr2013009541. [Google Scholar]



