
Bilateral head radius fracture – diagnosis and management.
Dr. Anuj Kumar, Department of Orthopedics, Dr. Rajendra Prasad Government Medical College, Kangra, Himachal Pradesh, India. E-mail: docvipinsharma@gmail.com
Abstract
Introduction: Bilateral radial head fractures are a unique and rare presentation. Few studies are available in the literature documenting these type of injuries. We present a rare case of bilateral radial head fractures (Mason type 1) and managed conservatively with full functional recovery.
Case Report: A 20-year-old male sustained bilateral radial head fractures (Mason type 1) following a roadside accident. The patient was managed conservatively with above elbow slab for 2 weeks followed by range of motion exercises. The patient had uneventful follow-up with full range of motion at elbow.
Conclusion: Bilateral radial head fractures in a patient are a discreet clinical entity. A high index of suspicion, meticulous history, clinical examination, and appropriate imaging is essential in patients with history of fall on outstretched hands to avoid missing diagnosis. Early diagnosis, proper management, and appropriate physical rehabilitation lead to complete functional recovery.
Keywords: Bilateral elbow joint, fracture dislocation, radial head fractures.
The elbow joint is a complex joint, in which superior radioulnar joint plays a key role in the pronation and supination of the forearm. The radial head may be fractured when it collides with the capitulum. This can occur with a pure axial load (e.g., Essex-Lopresti injury), a valgus load, posterolateral rotatory type of load, or as the radial head dislocates posteriorly as part of a posterior Monteggia fracture or posterior olecranon fracture-dislocation [1]. It accounts for about 2% of all fractures around the elbow, but bilateral radial head fractures are very rare. Few studies are available in literature documenting these type of injuries. Hence, we are reporting this unique and rare presentation of bilateral radial head fracture in a patient which was conservatively managed with full functional recovery.
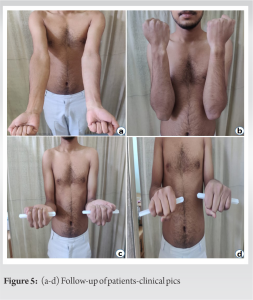
A 20-year-old male presented to the emergency department with complaints of pain and swelling in bilateral elbow joints following a roadside accident involving a bike skid. The patient had a fall backward with both arms in outstretched position. At the time of fall, there was extension at shoulder and elbow; supination at forearm; and dorsiflexion at wrist. On clinical examination, swelling 2 × 1 cm was noted on posterolateral aspect of elbow over radial head. Deep tenderness over radial head was present bilaterally. Pronosupination and flexion-extension movements at elbow were painful and restricted. No varus or valgus instability was noted in both elbows. On radiography, type I radial head fracture (Mason’s Classification) was noted bilaterally (Fig. 1 and 2). The patient was managed conservatively with above elbow slab ×2 weeks and NSAIDs. Following slab removal after 2 weeks, physiotherapy both elbows was initiated. The patient had pain free and full range of motion at 6 weeks follow-up (Fig. 3, 4, 5).
The patient was managed conservatively with above elbow slab ×2 weeks and NSAIDs. Following slab removal after 2 weeks, physiotherapy both elbows was initiated. The patient had pain free and full range of motion at 6 weeks follow-up (Fig. 3, 4, 5).
Mason classification is commonly used for classification of radial head fractures with Mason type 1: undisplaced marginal fractures; type 2: displaced marginal fractures; and type 3 as comminuted fractures [2]. Morrey has further refined this classification by adding variables of displacement, articular surface and fracture dislocation – (a) fractures of radial neck, (b) including a quantitative definition of displacement (a fragment involving 30% or more of articular surface that is displaced more than 2 mm), and (c) incorporated fracture-dislocations of the elbow [3]. Mason type 1 is the injuries frequently reported, while some studies have reported, Mason type 2 and Mason type 3 injuries as a bilateral fracture head radius presentation [4,5,6,7,8] (Table 1). Radiography (AP and Lateral View) elbow is an important tool, being essential for diagnosis of radial head fractures. Inclusion of a joint above and below elbow is essential to avoid missing fracture combinations like Essex-Lopresti fractures [9]. Some additional views, for example, Green Span view may be required for better visualization of radial head fracture. MRI is helpful in 76–90% of patients with radial head fractures for detection of soft tissue and cartilaginous injuries [10]. Clinically, relevant associated injuries, for example, coronoid fractures and elbow dislocations were found in 39% of patients with radial head fractures in some studies with likelihood of associated injury strongly correlated to the severity of the radial head fracture [11]. Treatment of radial head fractures ranges from conservative management in Mason type 1 fractures, for example, immobilization to operative modalities such as ORIF with Herbert Screws/1.5–2 mm cancellous screws, arthroscopic excision, and radial head arthroplasty in Mason type 2 and 3 fractures [1]. Conservative treatment, for example, above elbow slab/pressure bandage or cuff and collar sling for support followed by active mobilization as early as possible is the method of choice for Mason type I fractures [8]. The shortest the period of immobilization, the best are patient-reported outcome measure scores (PROMs) at follow-up [12]. These fracture types are prone to overtreatment in the form of radiographic follow-up without modifying treatment, leading to unnecessary patient visits, radiation exposure, and increased costs [13]. Introduction of new techniques and implants for the fixation of small articular fracture fragments in type 2 fractures has improved their surgical outcome [14]. In some studies with comparative evaluation of surgical and conservative modalities of treatment in Mason type 2 fractures, no clear cut advantage of one technique over the other has been reported [10]. Isolated comminuted radial head fractures, without associated instability of the elbow, are managed by resection of the radial head with satisfactory outcome [15]. Replacement of comminuted radial head by silicone implants restores elbow stability, but several implant-related problems and complications have been reported [16]. On the other hand, ORIF is another option for Mason type III fractures, but ORIF in more than 3 fracture fragments has resulted in unsatisfactory outcome due to difficult reduction, hardware failure, and non-union [17]. Only one randomized study comparing ORIF versus radial head arthroplasty for comminuted unstable radial head fractures has reported significantly better PROMs in arthroplasty group [18]. However, it is currently unknown whether one fixation technique has superior outcomes over the others. The present patient was having bilateral radial head fractures (Mason Type 1) and, hence, was managed by bilateral above elbow immobilization for 10 days followed by active elbow exercises, following which he had full range of motion.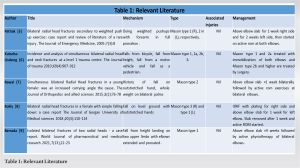
Bilateral radial head fractures in a patient are a discreet clinical entity. A high index of suspicion, meticulous history, clinical examination, and appropriate imaging is essential in patients with history of falls on outstretched hands to avoid missing diagnosis. Early diagnosis, proper management, and appropriate physical rehabilitation lead to complete functional recovery.
Bilateral radial head fractures are an injury pattern, both rare and unique. Meticulous history, clinical examination, and radiography help identifying fracture geometry and providing appropriate treatment to the patient, leading thereby to improved functional outcome.
References
- 1.David R. Elbow fracture and dislocation. In: Robert WB, Charles MC, James DH, Margaret M, editors. Rockwood and Green’s Fractures in Adults. 7th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2010. p. 911-2. [Google Scholar | PubMed]
- 2.Mason ML. Some observations on fractures of the head of the radius with a review of one hundred cases. Br J Surg 1954;42:123-32. [Google Scholar | PubMed]
- 3.Morrey BF, editors. Radial head fractures. In: The Elbow and its Disorders. Philadelphia, PA: WB Saunders; 1985. p. 355. [Google Scholar | PubMed]
- 4.Pathak SK. Bilateral radial head fracture secondary to weighted push-up exercise: Case report and review of literature of a rare injury. J Emerg Med 2005;7:8. [Google Scholar | PubMed]
- 5.Kutscha-Lissberg F, Platzer P, Thalhammer G, Krumböck A, Vécsei V, Braunsteiner T. Incidence and analysis of simultaneous bilateral radial head and neck fractures at a level I trauma center. J Trauma 2010;69:907-12. [Google Scholar | PubMed]
- 6.Rawal PR, Fhoghlu CN, Mahapatra AN. Simultaneous bilateral Mason Type IIb radial head fractures in a young female: Was an increased carrying angle the cause? J Orthop Allied Sci 2015;3:76-8. [Google Scholar | PubMed]
- 7.Kokly S, Sahebjamee A. Bilateral radial head fractures in a female with simple falling down: A case report. J Gorgan Univ Med Sci 2018;20:110-4. [Google Scholar | PubMed]
- 8.Berrada H. Isolated bilateral fractures of the two radial heads-a case report. World J Pharma Med Res 2021;7:22-3. [Google Scholar | PubMed]
- 9.Kaas L, Turkenburg JL, van Riet RP, Vroemen J, Eygendaal D. Magnetic resonance imaging findings in 46 elbows with a radial head fracture. Acta Orthop 2010;81:373-6. [Google Scholar | PubMed]
- 10.Kaas L, Van Riet RP, Turkenburg JL, Vroemen JP, van Dijk CN, Eygendaal D, et al. Magnetic resonance imaging in radial head fractures: Most associated injuries are not clinically relevant. J Shoulder Elbow Surg 2011;20:1282-8. [Google Scholar | PubMed]
- 11.Van Riet RP, Morrey BF, O’Driscoll SW, Van Glabbeek F. Associated injuries complicating radial head fractures: A demographic study. Clin Orhop Relat Res 2005;441:351-5. [Google Scholar | PubMed]
- 12.Smits AJ, Giannakopoulos GF, Zuidema WP. Long-term results and treatment modalities of conservatively treated Broberg-Morrey Type 1 radial head fractures. Injury 2014;45:1564-68. [Google Scholar | PubMed]
- 13.Shulman BS, Lee JH, Liporace FA, Egol KA. Minimally displaced radial head/neck fractures (Mason type-I, OTA types 21A2.2 and 21B2.1): Are we “over treating” our patients? J Orthop Trauma 2015;29:31-5. [Google Scholar | PubMed]
- 14.Akesson T, Herbertsson P, Josefsson PO, Hasserius R, Besjakov J, Karlsson MK. Displaced fractures of the neck of the radius in adults. An excellent long-term outcome. J Bone J Surg Br 2006;88:642-4. [Google Scholar | PubMed]
- 15.Antuña SA, Sánchez-Márquez JM, Barco R. Long-term results of radial head resection following isolated radial head fractures in patients younger than forty years old. J Bone J Surg Am 2010;92:558-66. [Google Scholar | PubMed]
- 16.Vanderwilde RS, Morrey BF, Melberg MW, Vinh TN. Inflammatory arthritis after failure of silicone rubber replacement of the radial head. J Bone Joint Surg Br 1994;76:78-81. [Google Scholar | PubMed]
- 17.Ring D, Quintero J, Jupiter JB. Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-5. [Google Scholar | PubMed]
- 18.Chen X, Wang SC, Cao LH, Yang GQ, Li M, Su JC. Comparison between radial head replacement and open reduction and internal fixation in clinical treatment of unstable, multi-fragmented radial head fractures. Int Orthop 2011;35:1071-6. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 10, 2023 Transscaphoid Transcapitate Perilunate Fracture-dislocation with Inferior Arc Injury and Acute Ulnar Nerve Compression: A Case Report
June 10, 2023 Transscaphoid Transcapitate Perilunate Fracture-dislocation with Inferior Arc Injury and Acute Ulnar Nerve Compression: A Case Report May 10, 2022 Coccidioidomycosis Osteomyelitis of Distal Tibia in a Preschool Girl: A Case Report
May 10, 2022 Coccidioidomycosis Osteomyelitis of Distal Tibia in a Preschool Girl: A Case Report July 11, 2014 Rupture of Extensively Porous Coated Stems. – A Case Series of 2 Patients
July 11, 2014 Rupture of Extensively Porous Coated Stems. – A Case Series of 2 Patients- July 10, 2016 A Technical Note for Extracting an Incarcerated Femoral Kuntscher Nail