
Access of tumour and placing intact nail plate after excision reduces the incidence of post-operative nail deformity.
Dr. Dipen Ariwala, 86, Sardar Nagar Society, Sumul Dairy Road, Surat - 395 008, India. E-mail: dipenaariwala@yahoo.com
Abstract
Introduction: Glomus tumor is a rare hamartoma, common in young female which is excruciatingly painful and affects daily activities. It is usually present in distal phalanx (subungual) but may occur in different locations. A clinician needs high-level suspicion to diagnose this condition.
Case Report: We hereby reviewed five cases (four females and one male) of this rare entity selected from patients attending our outpatient department since 2016 and were operated on. Out of these five cases, four were primary cases and one reoccurrence. Each of these was managed with en bloc excision of tumor and confirming it with biopsy after diagnosing it clinically and radiologically.
Conclusion: Glomus tumors are rare, benign, and slow-growing tumors that arise from neuromuscular-arterial structures called glomus bodies. Radiologically, magnetic resonance imaging classically shows T1 weight isointense and T2 mild hyperintense. Approaching a subungual glomus tumor through transungual approach with complete excision of the nail plate has reduced the risk of reoccurrence due to complete view/access of the tumor and placing intact the nail plate after excision reduces the incidence of post-operative nail deformity.
Keywords: Glomus tumor, finger, reoccurrence, love sign, cold sensitivity.
A glomus body is a specialized receptor that aids in the regulation of pain and temperature. Hyperplasia of one of the components such as afferent arteriole, anastomotic canal, afferent venule, actin-containing glomus cell, retinaculum, and capsule results in glomus tumor formation. A major unresolved problem in the treatment of glomus tumors is the long average time from symptom onset to diagnosis, approximately 7 years [1,2]. Tomak et al. show how all 14 patients were misdiagnosed and prescribed NSAIDs over the years [1]. This temporal discrepancy before diagnosis may be the result of wide-ranging differences, including neuroma, hemangioma, neuropathic pain, arthritis, and gout inflammation [3,4]. Patients with glomus tumors experience severe pain and sensitivity to cold due to the presence of type C nerve fibers. Light pressure on a hard object, such as the head of a pin, causes extreme pain (Love test). About 50% of glomus tumors arise in the subungual region. On physical examination, patients with glomus tumors seek a doctor early, but the mass is often too small to be identified [5]. They are usually <1 cm in diameter and can be seen through overlying tissue as a deep red or purple discoloration. Radiographs are usually unremarkable, but bone erosion may be seen in long-standing lesions.
Case 1
A 30-year-old lady presented to us with pain (VAS score was 9) and increased sensitivity over the tip of the right index finger which worsens at night for 2 years. Her pain persisted despite multiple analgesics and frequent visits to the hospital. Her pain was so much that she had to continuously rub her hand against the surface. On physical examination, there was immense tenderness over the radial aspect of the tip of the index finger with bluish discoloration of the radial portion of the nail (Fig. 1). The hematological profile was within the normal limit. The radiograph of the right index finger was unremarkable. Magnetic resonance imaging (MRI) shows a 2 × 4 × 5 mm (APXTRXCC) sized well-circumscribed T2 hyperintense/T1 hypointense lesion in the subungual region of the radial aspect of the right index finger with mild scalloping of the underlying distal phalanx (Fig. 3, 4, 5).
The hematological profile was within the normal limit. The radiograph of the right index finger was unremarkable. Magnetic resonance imaging (MRI) shows a 2 × 4 × 5 mm (APXTRXCC) sized well-circumscribed T2 hyperintense/T1 hypointense lesion in the subungual region of the radial aspect of the right index finger with mild scalloping of the underlying distal phalanx (Fig. 3, 4, 5).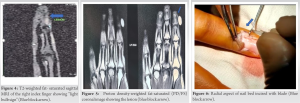 A dorsal approach to the index finger was performed under an operating microscope after complete excision with the removal of the overlying nail plate (Fig. 6, 7, 8).
A dorsal approach to the index finger was performed under an operating microscope after complete excision with the removal of the overlying nail plate (Fig. 6, 7, 8). A bluish mass of 2 × 3 × 4 mm (APXTRXCC) was identified and the sample was sent for histopathological evaluation. Closure of the wound done with Prolene 6–0 after placement of removed nail plate. Immediate post-operative pain was reduced to a VAS score of 2. The histopathological report was suggestive of glomus cells with bland round nuclei with pale eosinophilic cytoplasm, which confirmed the diagnosis of glomus tumor (Fig. 9).
A bluish mass of 2 × 3 × 4 mm (APXTRXCC) was identified and the sample was sent for histopathological evaluation. Closure of the wound done with Prolene 6–0 after placement of removed nail plate. Immediate post-operative pain was reduced to a VAS score of 2. The histopathological report was suggestive of glomus cells with bland round nuclei with pale eosinophilic cytoplasm, which confirmed the diagnosis of glomus tumor (Fig. 9).
Follow-up
Six months post-excision, the patient had complete relief of her symptoms (VAS score=0).
Case 2
A 35-year-old lady came to outpatient department (OPD) with the complaint of subungual pain in the left ring finger for 6 months. The pain was severe (VAS score was 8) and increased while washing utensils and during bathing. On clinical examination, love sign was positive with slight swelling over the radial aspect of the nail of the left ring finger. Ultrasonography of the local part showed a hypoechoic nodule with marked vascularity in the distal phalanx. She was advised dedicated MRI of her left ring finger which showed a 5 × 4 × 3 mm (APXTRXCC) sized well-defined oval lesion along the radial aspect of the nail bed of the left ring finger which was T1 weight isointense and T2 mild hyperintense (Fig. 10). Surgical excision using the dorsal approach to the nail bed, 1.5 cm incision taken bilaterally over the dorsal aspect of nail fold (V-shaped incision) (Fig. 11, 12). Removal of tumor (Fig. 13) followed by closure with 4–0 Prolene was done. Immediate post-operative her VAS score was 1. The excised tumor was sent for histopathology. Follow-up: Six months and 1-year postoperatively, she has no pain (VAS score: 0).
Surgical excision using the dorsal approach to the nail bed, 1.5 cm incision taken bilaterally over the dorsal aspect of nail fold (V-shaped incision) (Fig. 11, 12). Removal of tumor (Fig. 13) followed by closure with 4–0 Prolene was done. Immediate post-operative her VAS score was 1. The excised tumor was sent for histopathology. Follow-up: Six months and 1-year postoperatively, she has no pain (VAS score: 0).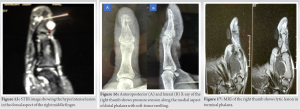
Case 3
A 45-year-old lady came to OPD with a chief complaint of severe pain (VAS score: 9) over the nail bed’s right middle finger which worsened during the night and had increased sensitivity to the cold. She was operated for the same 3 months back, but the pain persisted and increased gradually over the period of 3 months. The operative surgical specimen was sent for histopathology which confirmed it to be glomus tumor. On clinical examination, she has 1 cm × 1 cm bluish-colored well-defined, soft, and cystic swelling present over the deformed nail bed which was tender on palpation (Love test positive) (Fig. 14). MRI of the right ring finger was done (Fig. 15).
Case 4
A 42-year-old lady with a similar complaint of severe pain (VAS score: 9) over the distal nail bed of the right thumb which worsened at night and increased cold sensitivity. On examination also, finding were similar to the previous patient. X-ray was done (Fig. 16). MRI of the right thumb was suggestive of the small lytic lesion in the terminal phalanx of mid shaft of thumb with draining posterior granulation tissue extending into the nail bed. A noteworthy point is X-ray and MRI which are inconclusive of glomus tumor (Fig. 17). She was operated in a similar way and the specimen was sent for histopathology which showed a tumor composed of multiple thin-walled slit-like vessels surrounding which is tumor cells, which are round with punched out nucleus, a moderate amount of eosinophilic cytoplasm in the myxoid and hyalinized stroma. Immediate postoperatively her VAS score was 1. Three weeks post-procedure, patient’s VAS score was 0.
Case 5
A 44-year-old male has a painful nail bed (VAS score: 8) of the little finger with physical examination suggestive of glomus tumor (Fig. 18). MRI of the left little finger which showed a 1 × 2 × 2.5 mm (APXTRXCC) sized well-defined oval lesion T1 hypointense and T2 hyperintense lesion in the subungual region of little finger (Fig. 19). He was also operated in a similar manner with a histopathology report confirming the diagnosis of glomus tumor. Postoperatively 3 weeks and 6 weeks later, her VAS score was 0.
Glomus tumor is a benign tumor which requires a thorough history, clinical examination, and MRI for correct diagnosis. Etiology is unknown but a hereditary link is found. Early diagnosis of glomus tumors is critical to avoid treatment delays, chronic pain, and psychiatric misdiagnosis. Glomus tumors appear as painful, purplish-red, pale papules, or nodules <2 cm in the deep dermis or subcutaneous fat, most commonly on the fingers, toes, or under the nail plate. The Hildreth sign is a reduction in pain and tenderness with the love test when using a tourniquet to induce transient ischemia. Most of the times X-ray finger is unremarkable, although lytic lesion may be present as seen in our case. Color Doppler is a good tool for the diagnosis of glomus tumors, but it is operator dependent [6].
Glomus tumors are neuromuscular arterial entities, usually dark on T1-weighted images and bright on T2-weighted images. Therefore, MRI is the test of choice. Most glomus tumors are benign. However, rare malignancies have also been reported [7]. The treatment of solitary glomus tumor is surgical [8]. Reoperation rates have been reported to be 12–24%, but careful and complete excision of well-encapsulated lesions is usually curative [9]. Literature has reported two approaches for excision that is transungual (through complete or partial removal of nails) and periungual [10].
The approach that we used in the above cases was transungual approach with complete removal of the nail which has noted the advantage of a complete view of the tumor and hence reduced risk of reoccurrence. Transungual with partial removal has been associated with nail deformity as seen in one of our case. Most of these tumors are benign; however, metastatic rates are more than 25% if the size of the lesion is more than 2 cm and histopathology is suggestive of malignancy. Inadequate excision is suggested if symptoms reoccur after day to week of excision and when a symptom appears after 2–3 years of surgery, it may imply that there are multiple tumors. The possibility of post-operative neuroma, which causes pain, cannot be overlooked [10]. For multiple tumors, argon, carbon dioxide, or Nd:YAG laser therapy, or sclerotherapy with hypertonic saline or sodium tetradecyl sulfate are preferred options. Our experience says that approaching a subungual glomus tumor through transungual approach with complete excision of nail plate has reduced the risk of reoccurrence due to complete view/access of the tumor and placing intact the nail plate after excision reduces the incidence post-operative nail deformity
References
- 1.Tomak Y, Akcay I, Dabak N, Eroglu L. Subungual glomus tumours of the hand: Diagnosis and treatment of 14 cases. Scand J Plast Reconstr Surg Hand Surg 2003;37:121-4. [Google Scholar | PubMed]
- 2.Rohrich RJ, Hochstein LM, Millwee RH. Subungual glomus tumors: An algorithmic approach. Ann Plast Surg 1994;33:300-4. [Google Scholar | PubMed]
- 3.Samaniego E, Crespo A, Sanz A. Key diagnostic features and treatment of subungual glomus tumor. Actas Dermosifiliogr 2009;100:875-82. [Google Scholar | PubMed]
- 4.Garg B, Machhindra MV, Tiwari V, Shankar V, Kotwal P. Nail-preserving modified lateral subperiosteal approach for subungual glomus tumour: A novel surgical approach. Musculoskelet Surg 2016;100:43-8. [Google Scholar | PubMed]
- 5.Mohler DG, Lim CK, Martin B. Glomus tumor of the plantar arch: A case report with magnetic resonance imaging findings. Foot Ankle Int 1997;18:672-4. [Google Scholar | PubMed]
- 6.Fornage BD. Glomus tumors in the fingers: Diagnosis with US. Radiology 1988;167:183-5. [Google Scholar | PubMed]
- 7.Vasisht B, Watson HK, Joseph E, Lionelli GT. Digital glomus tumors: A 29-year experience with a lateral subperiosteal approach. Plast Reconstr Surg 2004;114:1486-9. [Google Scholar | PubMed]
- 8.Samaniego E, Crespo A, Sanz A. Key diagnostic features and treatment of subungual glomus tumor. Actas Dermosifiliogr 2009;100:875-82. [Google Scholar | PubMed]
- 9.Garg B, Machhindra MV, Tiwari V, Shankar V, Kotwal P. Nail-preserving modified lateral subperiosteal approach for subungual glomus tumour: A novel surgical approach. Musculoskelet Surg 2016;100:43-8. [Google Scholar | PubMed]
- 10.Mohler DG, Lim CK, Martin B. Glomus tumor of the plantar arch: A case report with magnetic resonance imaging findings. Foot Ankle Int 1997;18:672-4. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Intramuscular Glomus Tumor of Foot Presenting as Neuroma of Sural Nerve: A Case Report
August 1, 2026 Intramuscular Glomus Tumor of Foot Presenting as Neuroma of Sural Nerve: A Case Report July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report February 1, 2026 National Demographic and Treatment Patterns of Finger Cellulitis, Paronychias, and Felons
February 1, 2026 National Demographic and Treatment Patterns of Finger Cellulitis, Paronychias, and Felons January 1, 2026 Extradigital Glomus Tumor of the Forearm: Lessons from a Missed Diagnosis
January 1, 2026 Extradigital Glomus Tumor of the Forearm: Lessons from a Missed Diagnosis