
Avascular patella necrosis is rare and usually associated with steroid use. Still, it can occur in traumatic cases also and can be treated with conservative management due to the non-progressive nature of the condition.
Dr. Rajesh Rana, Department of Orthopaedics, SCB Medical College and Hospital, Cuttack, Odisha, India. E-mail: rajesh.rana66@gmail.com
Introduction: Avascular necrosis (AVN) of patella is a very rare condition and occurs in very few case. Although underlying etiology is still unknown, some expert suggest that its due to interruption of blood supply to patella which may be due to high velocity trauma or may be due to long term history of steroid intake. Here are the findings of our case AVN patella and reviews of earlier literature.
Case Report: We present a case of a AVN patella in a 31-year-old male. The patient presented with pain in knee with stiffness and tenderness at knee followed by decrease range of movement of knee. Magnetic resonance imaging showed irregular cortical outline of patella with degenerative osteophytes-suggestive of osteonecrosis of patella. It was treated conservatively with physiotherapy for range of movement of knee.
Conclusion: ORIF with extensive exploration and infection may compromise that the vascularity of patella may lead to AVN of patella. As the disease is non-progressive, it is better to manage such patients conservatively with range of movement brace so as to decrease the chance of complication associated with surgical intervention.
Keywords: Avascular necrosis, patella, range of movement, non-progressive, physiotherapy.
Avascular necrosis (AVN) of patella is a rare entity and has been reported in very few cases. Osteonecrosis of the patella has been described after trauma [1] as a complication of a total knee arthroplasty [2, 3] and as an idiopathic disease [2, 3]. Secondary osteonecrosis of the patella associated with corticosteroid use has been reported as an isolated disease in five patients in four case reports [5, 6, 7, 8]. Male is highly susceptible than females and its a non-progressive disease. The underlying etiology of development of the disease is still a debate, but some experts suspect that an interruption of blood supply to a section of bone either femur or tibia is disrupted. The purpose of this case report is to define the clinical and radiographic characteristics and functional outcome of this disease.
A 31-year-old male presented with chief complaints of pain, stiffness, and decreased range of movement of knee. He had a history of comminuted fracture of patella following a road traffic accident in the year 2017. He had been surgically treated with ORIF with encirclage. He had been advised to start knee range of movement exercise from 6 weeks postoperatively followed by regular physiotherapy (Range of movement 0–50°). After regular follow-up on 1 month, 3 month, 6 month, and 1 year, the patient complained of anterior knee pain which did not subside even after regular physiotherapy at the end of 1 year.
Clinically,
- Tenderness over anterior aspect of knee
- Restricted range of movement of knee (flexion restricted to 50°)
- Stiffness around knee.
He was again admitted and planned for quadriceps V-Y plasty in the year 2018. Even after surgery, there was no significant difference in functional outcome of the patient (Range of movement achieved up to 60°). Knee pain was increasing day by day while walking and was not subsiding even after analgesic medication. As pain did not subside and there is stiffness and restricted range of movement of knee (Fig. 1). The patient admitted for encirclage implant removal followed by physiotherapy for range of motion of knee.
Investigation
- Routine blood investigation, serology markers, and chest X-ray
- X-ray of knee (anteroposterior view and lateral view) was done immediate post-operative, 6 weeks, 3 months, 1 year, and 2 years
- Magnetic resonance imaging.

Findings
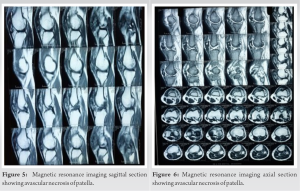
- Irregular cortical outline of patella with degenerative osteophytes-suggestive of osteonecrosis of patella (Fig. 2, 3, 4).
- Diffuse altered signal intensity in soft-tissue around patella involving subcutaneous plane with associated skin irregularity (post op change) (Fig. 5 and 6).
Steroid-induced osteonecrosis of the patella has been reported in the literature [8]. Often they are associated with other areas like hip osteonecrosis. Chronic use of steroids is reported for other systemic diseases. In our case, we had no steroid use, but there was traumatic history. Post-traumatic osteonecrosis of the patella is rare. Oishi et al. [7] also reported a similar case of osteonecrosis of the patella after chronic use of steroids. In their case, they had mild anterior knee pain for a long time, which on evaluation, they found osteonecrosis. He found degeneration of patellar cartilage with mild synovitis. The detached dead patellar fragments became loose bodies and started moving inside the knee joint. Removal of loose bodies leads to significant improvement of symptoms. Unlike their case, we had pain and movement restrictions due to stiffness. Post-traumatic osteonecrosis is often associated with stiffness due to previous trauma or surgeries. Physiotherapy improved stiffness. Elkayam et al. [5] also reported a similar case of AVN of the patella. The patient had ulcerative colitis and for which he was taking steroids chronically. Scapinelli [1] reported some cases of AVN of the patella following trauma. There were some improvements in their cases with time, unlike our case, with slow improvement. There was one case report AVN of patella following global dislocation of patella and it was treated with conservative treatment [9]. The patient regained vascularity of patella with over a period of time. In our case, also patient was managed conservatively with reasonable functional rehabilitation. AVN of patella is a noted complication following total knee replacement following patellar resurfacing [2, 10].
ORIF with extensive exploration and infection may compromise the vascularity of patella may lead to AVN of patella. Stiffness is maybe a associated complication of long-term immobilization and fibrosis around the knee and may not be isolated associated with AVN patella. There is no significant difference in functional outcome between surgically treated group and conservatively treated groups. Rather, there is more chance of complications such as infections, hemorrhage, and neurovascular damage in surgically treated group followed by long term hospital stay. Only there is decrease in anterior knee pain of the patient following encirclage wire removal. As the disease is non-progressive, it is better to manage such patients conservatively with range of movement brace so as to decrease the chance of complication associated with surgical intervention.
Avascular patella necrosis is rare and usually associated with steroid use. Still, it can occur in traumatic cases also and can be treated with conservative management due to the non-progressive nature of the condition.
References
- 1.Scapinelli R. Blood supply of the human patella. Its relation to ischemic necrosis after fracture. J Bone Joint Surg 1967;49B:563-70. [Google Scholar]
- 2.Cameron HU, Huffer B. Avascular necrosis of the patella following total knee replacement. Acta Orthop Belg 1985;51:805-10. [Google Scholar]
- 3.Mont MA, Tomek IM, Hungerford DS. Core decompression for steroid associated avascular necrosis of the distal femur. Clin Orthop 1997;334:124-30. [Google Scholar]
- 4.LaPrade RF, Noffsinger MA. Idiopathic osteonecrosis of the patella: An unusual cause of pain in the knee. J Bone Joint Surg 1990;72A:1414-8. [Google Scholar]
- 5.Elkayam O, Fishel B, Zhukovsky G, Yaron M. Steroid induced avascular necrosis of the patella in an ulcerative colitis patient. Clin Exp Rheumatol 1996;14:447-8. [Google Scholar]
- 6.Mizuta H, Kubota K, Shiraishi M, Kai K, Nakamura E, Takagi K. Steroidrelated bilateral osteonecrosis of the patella. Arthroscopy 1993;9:114-6. [Google Scholar]
- 7.Oishi Y, Yokota S, Nakagami W, Tsunoda K, Ueda H, Takahashi Y, et al. Steroid induced osteonecrosis of the patella: A case report. Acta Orthop Scand 1991;62:178-9. [Google Scholar]
- 8.Yamaguchi H, Masuda T, Sasaki T, Nojima T. Steroid-induced osteonecrosis of the patella. Clin Orthop 1988;229:201-4. [Google Scholar]
- 9.Brueckmann FR. Natural history of avascular necrosis of the patella due to closed global patellar dislocation. J South Orthop Assoc 1998;7:222-6. [Google Scholar]
- 10.Nakagawa Y, Matsusue Y, Akagi M, Nakamura T. Osteonecrosis of the resurfaced patella following bilateral total knee arthroplasty. A case report and review of the literature. Bull Hosp Jt Dis 1999;58:224-7. [Google Scholar]







