
Swelling in or around the ankle pediatric age group, the differential diagnosis should include synovial chondromatosis.
Dr. Sandeep K Yadav, Department of Orthopedics, AIIMS, Jodhpur, Rajasthan, India. E-mail: sandy22987@gmail.com
Introduction: Synovial chondromatosis is not a common condition and involvement of the ankle joint is quite rare. We found only one case of synovial chondromatosis of the ankle joint among the pediatric population. We present a case of a 9-year-old boy with synovial chondromatosis of the left ankle.
Case Report: A 9-year-old boy had synovial osteochondromatosis in the left ankle joint, which caused pain, swelling, and restriction of movement of the left ankle. Radiological examinations showed variable size calcific foci adjacent to the medial malleolus and medial ankle joint space with mild soft-tissue swelling. The ankle mortise space was well-maintained. The magnetic resonance imaging of the ankle joint revealed a benign synovial neoplastic process and a few focal marrows containing loose bodies. The synovium was thick, and there was no articular erosion. The patient was planned and underwent an en bloc resection. A lobulated pearly white mass arising from the ankle joint was observed intraoperatively. Histological examination also showed attenuated synovium with osteocartilaginous nodule with binucleated and multinucleated forms of chondrocyte typical of osteochondroma were appreciated. Endochondral ossification, mature bony trabeculae with intervening fibro adipose tissue, was noted. The patient had remarkable relief of clinical complaints and was almost asymptomatic at the time of the first follow-up.
Conclusion: Synovial chondromatosis may present with diverse clinical manifestations according to the different stages of the disease as described by Milgram; like joint pain, limitation of movements, swelling due to the close proximity of important structures including joints, tendons, and neurovascular bundles. A simple radiograph with a characteristic appearance is usually sufficient in confirming the diagnosis. In pediatric patients, overlooking these conditions may result in growth abnormality, skeletal deformities, and several mechanical problems. We suggest that when dealing with the case of swelling in or around the ankle, the differential diagnosis should include synovial chondromatosis.
Keywords: Synovial chondromatosis, osteocartilaginous nodule, case report, pediatric population, endochondral ossification, en bloc resection.
Synovial chondromatosis is a rare chronic synovial disease characterized by cartilaginous nodule and joint bodies caused by synovial hyperplasia. This is generally benign and more common in adult males aged 30–50 years, with an incidence of 1/100,000, a male-female ratio of approximately 1.8:1 and more recently 3: 1 [1, 2]. The most commonly affected joints are the knee joint (70%), hip joint (20%), and elbow joint (7.9%) [3]. Synovial chondromatosis rarely occurs in the ankle. As far as we know, only a single case of synovial chondromatosis of the ankle among the pediatric population has been described [4]. The rarity of ankle synovial chondromatosis among children in the literature leads us to report our case.
A 9-year-old boy presented to the outpatient department with a 1-year history of vague pain, swelling, and restriction of movement of the left ankle. The pain was not localized to a particular region, and swelling gradually increased over the medial aspect of the left ankle over the last 3–4 months. Physical examination revealed non-tender single spherical, lobulated swelling measuring 5×4×3 cm over the anterior aspect of the left medial malleolus (Fig. 1). The swelling was immobile, bony, hard in consistency, non-reducible, non-compressible, and not adhered to the skin. There were no secondary changes over the swelling. There was a restriction of dorsiflexion of the left ankle compared to the right side. The rest of the foot ankle examination was unremarkable. There was no other swelling elsewhere in the body, and the patient was otherwise healthy, with no significant history. Radiograph of the left ankle showed mild soft-tissue swelling with variable size calcific foci adjacent to the medial malleolus and medial tibiotalar joint space, but no significant bony erosion. The ankle mortise space was well maintained (Fig. 2). 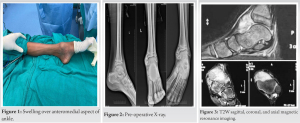 A magnetic resonance imaging of the left ankle was obtained, which suggested diffuse benign synovial neoplastic process of tibiotalar joint with 1–2 cm size few focal marrows containing loose bodies adjacent to the medial malleolus. The synovium of the ankle joint was thick, and there was no cortical erosion, and tibiotalar joint space was normal. These imaging findings favor primary synovial chondromatosis (Fig. 3). In light of these data, the patient was taken for an en bloc excisional biopsy. During the biopsy, a lobulated pearly white mass arising from the ankle joint was observed (Fig. 4). The lesion and synovium were excised and sent for a histopathology examination (Fig. 5). The diagnosis of synovial chondromatosis was confirmed by histologic examination.
A magnetic resonance imaging of the left ankle was obtained, which suggested diffuse benign synovial neoplastic process of tibiotalar joint with 1–2 cm size few focal marrows containing loose bodies adjacent to the medial malleolus. The synovium of the ankle joint was thick, and there was no cortical erosion, and tibiotalar joint space was normal. These imaging findings favor primary synovial chondromatosis (Fig. 3). In light of these data, the patient was taken for an en bloc excisional biopsy. During the biopsy, a lobulated pearly white mass arising from the ankle joint was observed (Fig. 4). The lesion and synovium were excised and sent for a histopathology examination (Fig. 5). The diagnosis of synovial chondromatosis was confirmed by histologic examination.
Histologic studies
On gross examination, it was a grey-white cartilaginous nodule. On microscopy, subepithelium showed attenuated synovium with osteocartilaginous nodule and moderate cellularity and variable atypia. Binucleated and multinucleated form of chondrocyte was appreciated. Enchondral ossification, mature bony trabeculae with intervening fibro adipose tissue, was noted. All these features are consistent with synovial chondromatosis. Following en bloc excision, the patient had symptomatic relief in the early post-operative and was utterly asymptomatic at the time of stitch removal. In addition, at annual follow-up patient has no sign of recurrence and pain free.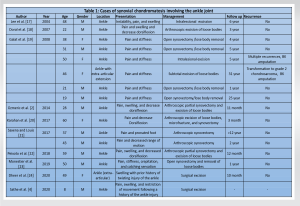
Ambroise paré first described synovial chondromatosis in 1558 [5]. In 1813, leannac claimed that the pathological changes were due to synovial-derived intra-articular bodies [6, 7]. There are two types of synovial chondromatosis described: Primary and Secondary. Primary synovial chondromatosis occurs in an otherwise normal joint and is characterized by undifferentiated stem cell proliferation in the synovial [8, 9]. It is more common in young and middle-aged adults and rare in children [4, 10, 11]. The pathological process is considered to be synovial cell cartilaginous metaplasia, and trauma is generally considered a trigger stimulus, but no statistical relevance has been described in the literature. Immunostaining revealed that primary synovial chondromatosis is a metaplastic condition [12]. Individual nodules can separate from the synovium and form a loose body in the joints, and these loose bodies continue to grow and are nourished by synovial fluid. These nodules can be further calcified and are known as osteochondromatosis, but only two-thirds of patients have been reported to have calcification. It is generally believed that primary synovial chondromatosis is progressive, likely to recur, and lead to severe osteoarthritis [13, 14]. Secondary synovial chondromatosis is caused by irritation of the synovium of the affected joint [8, 15]. It occurs when cartilage debris detaches from the articular surface and is embedded in the synovial [15]. It is associated with a pre-existing condition of joints such as degenerative joint disease, trauma, inflammatory and non-inflammatory arthropathy, avascular necrosis, and osteochondritis dissecans [15]. This form is unlikely to recur after surgical resection [13]. In 1977, milgram categorized the disease process into three different stages [16]. In Phase I, there is metaplasia of the synovial intima. There is active synovitis and nodular formation but no calcification. In Phase II, nodular synovitis and a loose body are present in the joints, and the loose body is cartilaginous mainly. In Phase III, synovitis subsides, but the loose body remains, which tend to adhere and calcify [16]. Diagnosis can be more difficult in the third stage, because there is no evidence of histological metaplasia. A summary of previously documented synovial chondromatosis of the ankle joint is presented in Table 1. Since the incidence of synovial chondromatosis in the ankle joint is very low and even rare in children, this report was presented as a case study. The condition was detected by clinical examination, diagnosed by radiographic imaging, and confirmed by histopathological examination. Standard radiograph of the left ankle showed several foci of calcifications of varying sizes adjacent to the medial malleolus and no significant adjacent cortical bone erosion (excluding malignancy), osteophytic proliferation, cyst formation, or the presence of degenerative changes in the affected joint. Therefore, a simple X-ray image with a characteristic appearance helped in clinching the diagnosis. There was no significant history of previous trauma or systemic inflammatory response. Thus, based on clinical and radiological findings, our case was evaluated as primary synovial chondromatosis of the ankle in Phase III since there was no pre-existing condition of the ankle, and loose bodies adhered to each other and calcified. Treatment decisions primarily are based on the patient’s age, symptoms, and stage, but surgery is often the treatment of choice. However, the surgical approach may vary depending on the stage. Stage: 1 synovectomy and stage 2: synovectomy and loose body removal, and removal of loose bodies for stage 3 [16, 25]. Other authors report that removing the loose body alone yields similar results to synovectomy and removal [26]. The natural history of this condition is not well known. Milgram has described cases where some nodules have been resorbed spontaneously and not extruded into the joint [16]. However, if extra-capsular chondromatous lesions are present, the lesions seem to behave more like a neoplasm than a reactive process, and surgical intervention is recommended. Malignant transformation of synovial chondromatosis into synovial chondrosarcoma is rare, but Davis et al. documented risk of malignant conversion of 5% (3/53) [3, 27, 28]. Other malignant transformation cases mainly occur in large joints [3, 27, 29, 30, 31, 32]. Therefore, we recommend that patients be counseled in this regard and offered periodic follow-ups to detect recurrence.
We described an unusual case of synovial chondromatosis of the ankle joint in a child. We evaluated this case with the other patients described in the literature. The patient responded well to the en bloc excision with significant symptomatic relief by the time of stitch removal, that is, 2 weeks, and was utterly pain-free at follow-up. The involvement of the ankle joint and the presentation in a 9-year boy makes this case unique, with no matched reference on literature search. When swelling develops in or around the ankle, the differential diagnosis should include synovial chondromatosis.
Appropriate early intervention as discussed above can prevent deformity and joint functionality. Synovial chondromatosis should be considered as a differential in swelling around joint in children if X-rays are suggestive of calcific foci.
References
- 1.Jiménez-Martín A, Zurera-Carmona M, Santos-Yubero FJ, Pérez-Hidalgo S. Arthroscopic treatment of synovial chondromatosis, an unusual cause of shoulder pain. Reumatol Clin 2014;10:416-7. [Google Scholar]
- 2.Ozmeric A, Aydogan NH, Kocadal O, Kara T, Pepe M, Gozel S. Arthroscopic treatment of synovial chondromatosis in the ankle joint. Int J Surg Case Rep 2014;5:1010-3. [Google Scholar]
- 3.Davis RI, Hamilton A, Biggart JD. Primary synovial chondromatosis: A clinicopathologic review and assessment of malignant potential. Hum Pathol 1998;29:683-8. [Google Scholar]
- 4.Sathe P, Agnihotri M, Vinchu C. Synovial chondromatosis of the ankle in a child: A rare presentation. J Postgrad Med 2020;66:112-3. [Google Scholar]
- 5.Barwell R. Clinical lectures on movable bodies in joints. Br Med J 1876;1:403-5. [Google Scholar]
- 6.Evans S, Boffano M, Chaudhry S, Jeys L, Grimer R. Synovial chondrosarcoma arising in synovial chondromatosis. Sarcoma 2014;2014:647939. [Google Scholar]
- 7.Halstead AE. IV. Floating bodies in joints. Ann Surg 1895;22:327-42. [Google Scholar]
- 8.Yu GV, Zema RL, Johnson RW. Synovial osteochondromatosis. A case report and review of the literature. J Am Podiatr Med Assoc 2002;92:247-54. [Google Scholar]
- 9.Leu JZ, Matsubara T, Hirohata K. Ultrastructural morphology of early cellular changes in the synovium of primary synovial chondromatosis. Clin Orthop Relat Res 1992;276:299-306. [Google Scholar]
- 10.Kumar A, Thomas AP. Recurrent synovial chondromatosis of the index finger case report and literature review. Hand Surg 2000;5:181-3. [Google Scholar]
- 11.Nashi M, Manjunath B, Banerjee B, Muddu BN. Synovial chondromatosis in a child: An unusual cause of shoulder pain case report. J Shoulder Elbow Surg 1998;7:642-3. [Google Scholar]
- 12.Davis RI, Foster H, Biggart DJ. C-erb B-2 staining in primary synovial chondromatosis: A comparison with other cartilaginous tumours. J Pathol 1996;179:392-5. [Google Scholar]
- 13.Valmassy R, Ferguson H. Synovial osteochondromatosis. A brief review. J Am Podiatr Med Assoc 1992;82:427-31. [Google Scholar]
- 14.Walling AK, Gasser SI. Soft-tissue and bone tumors about the foot and ankle. Clin Sports Med 1994;13:909-38. [Google Scholar]
- 15.Peh WC, Shek TW, Davies AM, Wong JW, Chien EP. Osteochondroma and secondary synovial osteochondromatosis. Skeletal Radiol 1999;28:169-74. [Google Scholar]
- 16.Milgram JW. Synovial osteochondromatosis: A histopathological study of thirty cases. J Bone Joint Surg Am 1977;59:792-801. [Google Scholar]
- 17.Young-In Lee F, Hornicek FJ, Dick HM, Mankin HJ. Synovial chondromatosis of the foot. Clin Orthop Relat Res 2004;423:186-90. [Google Scholar]
- 18.Doral MN, Uzumcugil A, Bozkurt M, Atay OA, Cil A, Leblebicioglu G, et al. Arthroscopic treatment of synovial chondromatosis of the ankle. J Foot Ankle Surg 2007;46:192-5. [Google Scholar]
- 19.Galat DD, Ackerman DB, Spoon D, Turner NS, Shives TC. Synovial chondromatosis of the foot and ankle. Foot Ankle Int 2008;29:312-7. [Google Scholar]
- 20.Karahan HG, Cetin O, Kurtulmuş A, Kayali C. Arthroscopic management and treatment of synovial chondromatosis and talus osteochondral defect in the ankle joint. A case study. Ortop Traumatol Rehabil 2017;19:293-6. [Google Scholar]
- 21.Saxena A, St Louis M. Synovial chondromatosis of the ankle: Report of two cases with 23 and 126 loose bodies. J Foot Ankle Surg 2017;56:182-6. [Google Scholar]
- 22.Peixoto D, Gomes M, Torres A, Miranda A. Arthroscopic treatment of synovial chondromatosis of the ankle. Rev Brasil Ortop (Engl Ed) 2018;53:622-5. [Google Scholar]
- 23.Monestier L, Riva G, Stissi P, Latiff M, Surace MF. Synovial chondromatosis of the foot: Two case reports and literature review. World J Orthop 2019;10:404-15. [Google Scholar]
- 24.Dheer S, Sullivan PE, Schick F, Karanjia H, Taweel N, Abraham J, et al. Extra-articular synovial chondromatosis of the ankle: Unusual case with radiologic-pathologic correlation. Radiol Case Rep 2020;15:445-9. [Google Scholar]
- 25.Fujita I, Matsumoto K, Maeda M, Kizaki T, Okada Y, Yamamoto T. Synovial osteochondromatosis of the Lisfranc joint: A case report. J Foot Ankle Surg 2006;45:47-51. [Google Scholar]
- 26.Shpitzer T, Ganel A, Engelberg S. Surgery for synovial chondromatosis: 26 cases followed up for 6 years. Acta Orthop Scand 1990;61:567-9. [Google Scholar]
- 27.Maurice H, Crone M, Watt I. Synovial chondromatosis. J Bone Joint Surg Br 1988;70:807-11. [Google Scholar]
- 28.Murphy FP, Dahlin DC, Sullivan CR. Articular synovial chondromatosis. J Bone Joint Surg 1962;44:77-86. [Google Scholar]
- 29.Hamilton A, Davis RI, Nixon JR. Synovial chondrosarcoma complicating synovial chondromatosis. Report of a case and review of the literature. J Bone Joint Surg 1987;69:1084-8. [Google Scholar]
- 30.Mullins F, Berard CW, Eisenberg SH. Chondrosarcoma following synovial chondromatosis. A case study. Cancer 1965;18:1180-8. [Google Scholar]
- 31.Perry BE, McQueen DA, Lin JJ. Synovial chondromatosis with malignant degeneration to chondrosarcoma. Report of a case. J Bone Joint Surg 1988;70:1259-61. [Google Scholar]
- 32.Taconis WK, Van der Heul RO, Taminiau AM. Synovial chondrosarcoma: Report of a case and review of the literature. Skeletal Radiol 1997;26:682-5. [Google Scholar]








