
Melorheostosis, apart from the affected bone, can also rarely present extra-osseously in the surrounding soft tissues and sometimes affect the functionality of the nearby joint. Early diagnosis and complete excision can result in the regaining of full function of the affected joint.
Dr. Ashok Gachhayat, Department of Orthopaedics, KIMS, Bhubaneswar, Odisha, India. E-mail: drashokscb84@gmail.com
Introduction: Melorheostosis was initially identified in 1922 by Leri and Joanny. It is often referred to as candle bone disease, melting wax syndrome, or Leri disease. This mesenchymal condition is uncommon, benign, and non-heritable. There is still a lack of clarity regarding the underlying cause of the condition. The estimated incidence is 0.9% per million. No inherited traits have been identified, and both sexes are equally affected. Pain or swelling is the most typical symptoms, and the onset is insidious. People often call this condition “candle disease of the bone” because the radiological signs of it look like dripping candle wax.
Case Report: A 56-year-old female presented with an 8-year history of the left knee pain, swelling, and movement restriction. On examination, a hard, bony lump measuring 12×5 cm was located on the outer aspect of the left knee. The skin over the lump’s surface was neither erythematous nor warm. Plain radiographs revealed a wide, dense, undulating, or irregular cortical hyperostosis, resembling candle wax, spreading along the length of the fibula bone as well as an extra-osseous calcification mass across the lateral aspect of the left knee. The patient underwent excision with complete left knee motion.
Conclusion: Melorheostosis’ actual etiology is yet unknown. There is no established treatment for this condition. Only symptomatic treatment helps patients feel better; in some circumstances, the excision of a bone mass yields more beneficial results.
Keywords: Melorheostosis, rare, benign, candle wax, extra-osseous, Myositis ossificans.
Melorheostosis was initially identified in 1922 by Leri and Joanny [1]. It is often referred to as candle bone disease, melting wax syndrome, or Leri disease. This mesenchymal condition is uncommon, benign, and non-heritable. There is still a lack of clarity regarding the underlying cause of the condition [1]. The estimated incidence is 0.9% per million [2]. The term “melorheostosis” comes from the Greek words “melos,” “rhein,” and “osteos” [3]. It typically starts in childhood and affects both sexes equally. Patients typically have an insidious onset of discomfort and edema [4]. Axial skeleton involvement is sporadic and typically only affects the diaphysis of the long bone of the lower limb. Cortical bone thickening causes uneven hyperostosis of bone, which seems to flow down the length of the bone [5]. Here, we discuss a rare case of extraosseous melorheostosis around the knee joint.
A 56-year-old woman presented with 10 years of dull aching pain, swelling, and limited movement in her left knee. 10 years prior, the pain began, and it was progressive in nature. There was no traumatizing past history. A swelling over the lateral aspect of the left knee joint that was gradually growing in size and connected to a gradual reduction in knee joint movement was noticed by the woman 2 years later. Activities involving knee flexion set off the pain. The patient has no past medical or family history that is clinically relevant. On examination, it was discovered that the left knee’s lateral aspect was swollen, but the area above it did not exhibit any localized redness or increase in temperature (Fig. 1). From the lateral aspect of the left distal femur down to the fibular head, the swelling was 15×5 cm, bony, hard, not connected to the underlying bone, and non-tender. The range of motion for the left knee joint was 0–40°, with further movement restricted (Fig. 2). There was no evidence of a distal neurovascular impairment. In any other region of the body, there were no lesions like this. Plain radiographs revealed an irregular extraosseous radiolucent mass extending to the fibular head across the lateral aspect of the left knee with no bony contact. Cortical hyperostosis that looked like candle wax covered the whole length of the fibula (Fig. 3). This cortical hyperostosis was large, thick, undulating, or irregular. The results of the tests were within normal ranges for the CBC, serum calcium, phosphate, alkaline phosphatase, erythrocyte sedimentation rate, C-reactive protein, beta-fetoprotein, and carcinoembryonic antigen. The lump, which measured 13 cm by 5 cm, was cut out entirely by making a longitudinal incision along the lateral portion of the left knee joint and doing soft tissue dissection (Fig. 4 and 5). A distinct 3 cm x 1.5 cm tiny lump was also removed (Fig. 5).
From the lateral aspect of the left distal femur down to the fibular head, the swelling was 15×5 cm, bony, hard, not connected to the underlying bone, and non-tender. The range of motion for the left knee joint was 0–40°, with further movement restricted (Fig. 2). There was no evidence of a distal neurovascular impairment. In any other region of the body, there were no lesions like this. Plain radiographs revealed an irregular extraosseous radiolucent mass extending to the fibular head across the lateral aspect of the left knee with no bony contact. Cortical hyperostosis that looked like candle wax covered the whole length of the fibula (Fig. 3). This cortical hyperostosis was large, thick, undulating, or irregular. The results of the tests were within normal ranges for the CBC, serum calcium, phosphate, alkaline phosphatase, erythrocyte sedimentation rate, C-reactive protein, beta-fetoprotein, and carcinoembryonic antigen. The lump, which measured 13 cm by 5 cm, was cut out entirely by making a longitudinal incision along the lateral portion of the left knee joint and doing soft tissue dissection (Fig. 4 and 5). A distinct 3 cm x 1.5 cm tiny lump was also removed (Fig. 5). 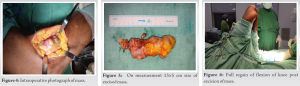 As the common peroneal traveled along it, the bulk around the fibular head was left behind. The tissue that was removed was sent for histological analysis. After the removal, the knee could move from 0 to 130° during the operation (Fig. 6 and 7). The results of the biopsy mentioned in this section show the lamellar bone with trabeculae that are getting bigger and the Haversian Canal (Fig. 8).
As the common peroneal traveled along it, the bulk around the fibular head was left behind. The tissue that was removed was sent for histological analysis. After the removal, the knee could move from 0 to 130° during the operation (Fig. 6 and 7). The results of the biopsy mentioned in this section show the lamellar bone with trabeculae that are getting bigger and the Haversian Canal (Fig. 8).
Leri and Joanny described melorheostosis for the 1st time in 1922 [6]. Hyperostotic linear bone densities with soft tissue contractures and ossification are characteristic of it [7]. Our patient’s age coincides with the typical presenting age range of 1–63 years [8]. Melarheostosis was observed in our patient’s left knee and left fibular bone. As has already been shown [8, 9], the lower limbs are more often affected than the upper limbs, ribs, and axial bones [1, 2]. The manifestations of melorheostosis might be monostotic, polyostotic, or monomelic. This rare condition usually looks like the monomelic form, which we also have. Although several explanations have been put forth, the precise pathophysiology of melorheostosis is still unknown. In 1979, Murray and McCredie [11] postulated that a spinal sensory nerve supplying a single sclerotome had an early developmental defect that led to bone overgrowth. In 1995, Fyns put forward the hypothesis that melorheostosis, which results in a postzygotic mutation of the mesenchyme and concurrent involvement of the bone, cutaneous, vascular, and soft tissues, was caused by mosaicism. In our case, this method simplifies the understanding of the soft-tissue involvement and bone fibula lesion [12]. According to several studies, melorheostosis results from a loss-of-function mutation in the LEMD3 gene (12q12–q14.3), which codes for an inner nuclear membrane protein that regulates bone formation and is implicated in the signaling of tumor growth factor and bone morphogenic protein. A proliferation of hyperostotic lesions may result from this gene’s mutations. The most frequent presenting complaint listed in the literature [8, 9] was knee discomfort, which is how our patient complained in this case. However, a lot of individuals have their diagnoses made by unintentional radiological findings [13]. Additional described signs and symptoms include soft-tissue contractures or masses [3, 10, 20], which were also present in our patient. They include stiffness and a restricted range of motion of the affected joint [11, 12, 19]. Melorheostosis is often diagnosed by radiological findings, such as those obtained from X-rays, computed tomography scans, magnetic resonance imaging, and bone scans; each modality has revealed distinctive characteristics [15]. Adults with melorheostosis have four radiological patterns on X-rays: the traditional falling wax type, an osteoma-like lesion, a myositis ossificans (MO)-like lesion, an osteopathia striata-like lesion, and a mixed type [3]. The radiological pattern in children typically differs from that in adults [8]. In our case, a typical lesion in the fibula bone coexists with a soft-tissue lesion that resembles MO on the lateral aspect of the knee joint. Melorheostosis lesions must be distinguished from MO and lesions that resemble MO. MO is typically preceded by a history of trauma, and radiologically, nodular calcification rather than the initial lamellar pattern is found in melorheostosis [3, 16]. In addition, a melorheostosis bone scan will exhibit a significantly higher tracer uptake than MO [17]. Since 1976 [18, 19], Tc-99m bone scintigraphy has been established as a technique to support the diagnosis of melorheostosis. Angiographical studies [16, 17] have demonstrated that melorheostosis increases tracer uptake, which bridges over the joints because of hypervascularity. Reduced tracer uptake in patients receiving bisphosphonate treatment lends support to the idea that increased osteoblastic activity and turnover are important aspects of melorheostosis [15]. Based on the clinical and radiological findings in our case, we think this is a classic case of melorheostosis in the fibula with a MO-like melorheostosis lesion on the side of the knee. Osteoma, parosteal osteosarcoma, localized scleroderma, synovial osteochondromatosis, and Cafey disease are among the conditions on the differential diagnostic list for melorheostosis. Diagnoses can be precisely differentiated by a comprehensive clinical examination and an extensive radiological workup [15]. Melorheostosis care approaches must be customized for each patient because there is currently no defined standard treatment [8]. The treatment aims to reduce pain and preserve function. In addition, there are a few papers that discuss the usage of bisphosphonates to effectively relieve pain. Patients who experience mechanical problems such as nerve compression, contractures, impingement, and deformity may choose surgical options [15]. Our patient has been followed up for more than 6 months, and radiological findings remain unchanged. Clinically, the pain has subsided with a complete knee range of motion.
Our patient’s melorheostosis presents in an unusual way, with a single extraosseous MO-like lesion and a characteristic candle-wax appearance along the length of the fibula on the X-ray image, combined with more mechanical symptoms of knee joint movement restriction. Our case adds to the body of knowledge about the numerous melorheostosis presentations and validates hypotheses that are currently held about the etiology of the condition. There is no conclusive treatment for this condition. The disease can only be cured by treating its symptoms. In our case, the extraosseous lump was surgically removed and the knee joint was given a full range of motion again.
A rare benign disease with a wide range of presentations is melorhoeostosis. It is distinguished by a distinct X-ray finding. So far, no conclusive treatment is available. Effective symptomatic therapy is administered with favorable outcomes.
References
- 1.Leri A, Joanny J. Une affection non décrite des os hyperostose “en coulée” sur toute la longeur d’un member ou “melorhéostose”. Bull Mem Soc Med Hosp Paris 1922;46:1141-5. [Google Scholar]
- 2.Wynne-Davies R, Gormley J. The prevalence of skeletal dysplasias. An estimate of their minimum frequency and the number of patients requiring orthopaedic care. J Bone Joint Surg Br 1985;67:133-7. [Google Scholar]
- 3.Freyschmidt J. Melorheostosis: A review of 23 cases. Eur Radiol 2001;11:474-9. [Google Scholar]
- 4.Biaou O, Avimadje M, Guira O, Adjagba A, Zannou M, Hauzeur JP. Melorheostosis with bilateral involvement in a black African patient. Joint Bone Spine 2004;71:70-2. [Google Scholar]
- 5.Rozencwaig R, Wilson MR, McFarland GB Jr. Melorheostosis. Am J Orthop (Belle Mead NJ) 1997;26:83-9. [Google Scholar]
- 6.Leri A, Joanny J. Une affection non décrite des os hyperostose “en coulée” sur toute la longeur d’un member ou “melorhéostose”. Bull Mem Soc Med Hosp Paris 1922;46:1141-5 [Google Scholar]
- 7.Jain K, Arya RK, Bharadwaj M, Kumar S. Melorheostosis: Clinicopathological features, diagnosis, and management. Orthopedics 2009;32:512-20. [Google Scholar]
- 8.Artner J, Cakir B, Wernerus D, Reichel H, Nelitz M. Melorheostosis: Current concepts in diagnosis and treatment-a review of literature (313 cases). J Musculoskelet Res 2012;15:1230002-18. [Google Scholar]
- 9.Zhang C, Dai W, Yang Y, Tang Q, Yao Z. Melorheostosis and a review of the literature in China. Intractable Rare Dis Res 2013;2:51-4. [Google Scholar]
- 10.Zeiller SC, Vaccaro AR, Wimberley DW, Albert TJ, Harrop JS, Hilibrand AS. Severe myelopathy resulting from melorheostosis of the cervicothoracic spine. A case report. J Bone Joint Surg Am 2005;87:2759-62. [Google Scholar]
- 11.Murray R, McCredie J. Melorheostosis and the sclerotomes: A radiological correlation. Skeletal Radiol 1979;4:57-71. [Google Scholar]
- 12.Fryns JP. Melorheostosis and somatic mosaicism. Am J Med Genet 1995;58:199. [Google Scholar]
- 13.Mumm S, Wenkert D, Zhang X, McAlister WH, Mier RJ, Whyte MP. Deactivating germline mutations in LEMD3 cause osteopoikilosis and Buschke-Ollendorff syndrome, but not sporadic melorheostosis. J Bone Miner Res 2007;22:243-50. [Google Scholar]
- 14.Hellemans J, Preobrazhenska O, Willaert A, Debeer P, Verdonk PC, Costa T, et al. Loss-of-function mutations in LEMD3 result in osteopoikilosis, Buschke-Ollendorff syndrome and melorheostosis. Nat Genet 2004;36:1213-8. [Google Scholar]
- 15.Elsheikh AA, Pinto RS, Mistry A, Frostick SP. A unique case of melorheostosis presenting with two radiologically distinct lesions in the shoulder. Case Rep Orthop 2017;2017:9307259. [Google Scholar]
- 16.Suresh T, Muthukumar T, Saifuddin A. Classical and unusual imaging appearances of melorheostosis. Clin Radiol 2010;65:593-600. [Google Scholar]
- 17.Davis DC, Syklawer R, Cole RL. Melorheostosis on three-phase bone scintigraphy. Case report. Clin Nucl Med 1992;17:561-4. [Google Scholar]
- 18.Bied JC, Malsh C, Meunier P. Melorheostosis in adults. Apropos of 2 cases, 1 of them treated with diphosphonate (EHDP). Rev Rhum Mal Osteoartic 1976;43:193-9. [Google Scholar]
- 19.Janousek J, Preston DF, Martin NL, Robinson RG. Bone scan in melorheostosis. J Nucl Med 1976;17:1106-8. [Google Scholar]








