
Chondrosarcoma of the great toe is a rare condition and early diagnosis with adequate surgical resection is associated with a high cure rate to avert complications like mets.
Dr. Shivank Khurana, Department of Orthopaedic Surgery, J.N.M.C.H., Faculty of Medicine, Aligarh Muslim University, Aligarh, Uttar Pradesh- 202002, India. E-mail: sshivankhurana2@gmail.com
Abstract
Introduction: Chondrosarcoma (CHS) of the toes is very rare and the involvement of phalanges is extremely rare. The osteolytic destruction of this tumor severely affects limb function and carries the risk of distant metastasis. These tumors are removed surgically to minimize local recurrence and distant metastases, maximize limb function with better prognosis. The main objective of this report is to present the case of a CHS that invaded the phalanx of the left great toe and formed a large phalangeal mass with osteolytic destruction of the distal bone.
Case Report: This case report includes a 60-year-old man suffering from swelling of his left great toe for 2 years, with pain and swelling for 6 months. Serial hematological, radiological and tumor investigations were done. Magnetic resonance imaging revealed a well-defined peripherally enhancing multilobulated soft-tissue mass with central necrotic component involving the entire proximal phalanx of left great toe extending to distal phalanx and head of first metatarsal. The patient was planned for operative intervention due to the possibility of invasion into the adjacent bones. The tumor was excised and sent for histopathological examination, which was reported as Grade 2 CHS (PT, Nx, and Mx) and was S100 positive. The patient has been followed-up for 5 months.
Results: There were no signs of local recurrence or distant metastasis on radiological investigations or clinical assessment during follow-ups.
Conclusion: CHS occurring in toes is extremely rare. In this case, extensive surgical resection of the large low-grade CHS was safe and effective.
Keywords: Chondrosarcoma, phalanges, excision
Enchondroma is the most common benign cartilage bone tumor of the toes. In contrast, the foot is a rare region for chondrosarcoma (CHS), and the involvement of phalanges is extremely rare. Primary CHS is the third most common primary malignancy of bone after plasmacytoma and osteosarcoma [1]. The most common skeletal sites are pelvic bones, followed by the proximal humerus, distal femur, and ribs. The small bones of the hands and feet are rarely affected (<1% of all cases of CHS) [2]. Although a positive prognosis is expected, there is little information about the biological behavior of phalangeal CHS. Phalangeal CHS acts as a locally aggressive lesion and, unlike CHS elsewhere, metastasis is rare. CHSs are innate cartilaginous malignant tumors in which the tumor matrix formation is completely chondroid. CHSs are most common in men aged 30–60 years, with a slight female dominance for phalangeal CHSs. The risk factors for CHS include enchondromas, multiple exostoses, Ollier’s disease, and Maffucci’s syndrome [3,4]. The most common symptoms are mild pain and tenderness. Local swelling with soft-tissue masses and pathologic fractures are other physical findings. CHS remote metastasis passes through a hematogenous pathway and typically progresses straight to the lungs. The overall prognosis is related to lesion size, anatomical location, type, and histologic grade. The 5-year survival rate for patients with Grade 1 lesions is 90%; the rate decreases to 29% for those with Grade 3 tumors. Grade 1 lesions do not metastasize. The radiographic appearance of conventional CHSs reveals large radiolucent areas with thick walls. The most important radiographic findings that indicate whether a tumor is low grade or high grade are the pattern of calcification, the nature of the tumor margin, and the size of the soft-tissue mass. Magnetic resonance imaging (MRI) provides a complete view of intraosseous and soft-tissue sizes of CHSs. Cartilage regions of the tumor have moderate signal intensity on T1-weighted images relative to adjacent skeletal muscle and high signal intensity on T2-weighted images. Calcification appears as an area without signal [5,6,7,8]. Computed tomography and standard radiography are the best methods for imaging calcification. When strengthened with gadolinium, MRI can determine the location of the biopsy by identifying areas of necrosis within the lesion. These physical and radiographic findings distinguish malignant and non-malignant tumors of the foot. The differential diagnosis of a standing CHS in the foot includes benign lytic bone tumors such as enchondroma, malignant bone tumors metastasized from other regions or osteosarcoma, and infection [9].
A 60-year-old healthy Indian male with a 2-year history of progressive swelling of the left great toe and history of pain and swelling over left great toe for the past 6 months. Rapid increase in the size of swelling was observed over the past 6 months. No history of antecedent trauma elicited. His past history was not significant. Initial examination revealed swelling and tenderness of the left middle toe. Swollen mass measured around 7 * 5 cm over the left great toe (Fig. 1).  The mass was firm to touch, tender on palpation, and had indistinct borders. The movements of the interphalangeal joint and metatarsophalangeal joint were limited. There were no skin color changes. The routine blood tests and biochemical tests were normal. A plain radiograph (Fig. 2) demonstrated a sclerotic change accompanied by soft-tissue swelling and a relatively large well defined lytic, expansile multiloculated lesion with endosteal scalloping involving proximal phalanges of great toe with areas of focal thinning and focal breach with reduced metatarsophalangeal joint space. MRI left foot (Fig. 3) revealed a well-defined peripherally enhancing multilobulated soft-tissue mass with central necrotic component involving the entire proximal phalanx of left great toe extending to distal phalanx and head of first metatarsal also infiltrating into adjacent muscles and tendons attached to great toe and in subcutaneous tissue both in dorsal and plantar aspect. The lesion appears hypointense on T1, heterogeneously hyperintense on T2/PD with restriction on DWI, and no evidence of blooming on SWI. Size ~ 5.8*4.7*4.6 cm. A tru-cut biopsy and fine needle aspiration cytology revealed intermediate CHS. The pre-operative imaging findings were suggestive of malignant occupancy of the first phalanx of the left foot with the possible distal invasion of the adjacent metatarsals.
The mass was firm to touch, tender on palpation, and had indistinct borders. The movements of the interphalangeal joint and metatarsophalangeal joint were limited. There were no skin color changes. The routine blood tests and biochemical tests were normal. A plain radiograph (Fig. 2) demonstrated a sclerotic change accompanied by soft-tissue swelling and a relatively large well defined lytic, expansile multiloculated lesion with endosteal scalloping involving proximal phalanges of great toe with areas of focal thinning and focal breach with reduced metatarsophalangeal joint space. MRI left foot (Fig. 3) revealed a well-defined peripherally enhancing multilobulated soft-tissue mass with central necrotic component involving the entire proximal phalanx of left great toe extending to distal phalanx and head of first metatarsal also infiltrating into adjacent muscles and tendons attached to great toe and in subcutaneous tissue both in dorsal and plantar aspect. The lesion appears hypointense on T1, heterogeneously hyperintense on T2/PD with restriction on DWI, and no evidence of blooming on SWI. Size ~ 5.8*4.7*4.6 cm. A tru-cut biopsy and fine needle aspiration cytology revealed intermediate CHS. The pre-operative imaging findings were suggestive of malignant occupancy of the first phalanx of the left foot with the possible distal invasion of the adjacent metatarsals.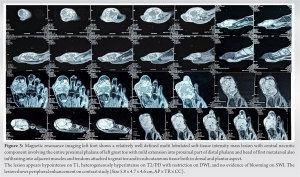 All routine blood tests, biochemical tests, and chest radiographs were within normal limits, and parallel CT examinations of the chest, abdomen, and pelvis revealed no metastatic lesions or other tumorigenic lesions. The patient and his family were informed of his condition based on the imaging findings and clinical symptoms. Due to the possibility of invasion of the adjacent distal metatarsal bone, the patient was advised to undergo extensive resection, and the patient and his family agreed. An orthopedic surgeon performed the surgical treatment. The surgeon performed an osteotomy of the first phalanx of the left foot and distal bone removal of the adjacent metatarsal (Fig. 4).
All routine blood tests, biochemical tests, and chest radiographs were within normal limits, and parallel CT examinations of the chest, abdomen, and pelvis revealed no metastatic lesions or other tumorigenic lesions. The patient and his family were informed of his condition based on the imaging findings and clinical symptoms. Due to the possibility of invasion of the adjacent distal metatarsal bone, the patient was advised to undergo extensive resection, and the patient and his family agreed. An orthopedic surgeon performed the surgical treatment. The surgeon performed an osteotomy of the first phalanx of the left foot and distal bone removal of the adjacent metatarsal (Fig. 4). 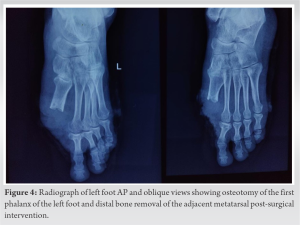 The tumor tissue was excised and sent for histopathological examination. Histological examination confirmed the previous histological diagnosis. Histology section (Fig. 5) shows lobules of chondrocytes having mild-to-moderate atypia along with mixed inflammation, necrosis, and hemorrhage. With a mitotic rate of: 0–1/10 HPF. Lymphovascular invasion was present, but no regional lymph node involvement was seen.
The tumor tissue was excised and sent for histopathological examination. Histological examination confirmed the previous histological diagnosis. Histology section (Fig. 5) shows lobules of chondrocytes having mild-to-moderate atypia along with mixed inflammation, necrosis, and hemorrhage. With a mitotic rate of: 0–1/10 HPF. Lymphovascular invasion was present, but no regional lymph node involvement was seen.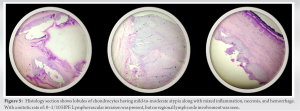 It suggested Grade 2 CHS (PT, Nx, Mx). S100 was done for confirmation which came out to be positive. The patient has been followed up for 5 months after surgery till date, and the patient is in good condition with no tumor recurrence or distant metastasis (Fig. 6).
It suggested Grade 2 CHS (PT, Nx, Mx). S100 was done for confirmation which came out to be positive. The patient has been followed up for 5 months after surgery till date, and the patient is in good condition with no tumor recurrence or distant metastasis (Fig. 6).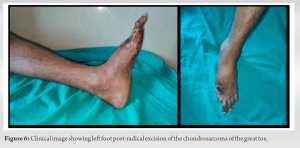
Cartilaginous tumors involving bones of the feet are usually benign tumors, such as enchondroma. CHS, the third most common type of primary malignant bone tumor, is very uncommon in the foot. In feet, the calcaneus, the talus, and the first metatarsal bone are the most frequent sites of involvement [3,4]. There is a slight female predominance for phalangeal CHS in comparison to other locations in the skeleton. Pain and swelling are the most frequent presentations. Phalangeal CHSs are locally aggressive tumors with minimal metastatic potential. CHS of the calcaneus and the talus are more likely to metastasize [4]. As a rule, CHSs are slow growing and tend to recur late. The metastatic potential and survival of CHS patients are correlated to the histologic grade. Prompt classification of the grade of CHS is important because the prognosis and treatment are different for different stages. Evans et al. [7] used their own grading system, as follows: Low-grade, low-level malignancy; intermediate-grade, moderately malignant; and high-grade, highly malignant. Reported 10-year survival rates were 83% for low-grade, 64% for intermediate-grade, and 29% for high-grade CHS. The incidence of metastatic disease is rare for low-grade, 10% for intermediate-grade, and 71% for high-grade CHS [6,7,8,9]. Bovée et al. [6] reported that phalangeal CHS recurs in 36% of cases but does not metastasize. Phalangeal CHS has a much better prognosis than CHS in other regions. Mohammadianpanah et al. [9] described a case of phalangeal CHS at the proximal phalanx of the third toe that proceeded to an amputation at the metacarpophalangeal joint. Histological differentiation between enchondroma and well-differentiated CHS may also be difficult. Hence, the correlation of the clinical, radiological, and histological findings is necessary to confirm the diagnosis. CHS in a small bone of the foot can be potentially fatal. The histological grade, location of the tumor, and adequacy of surgical excision are the major determinants of long-term survival [10]. Adequate surgical resection as simple or ray amputation is the treatment of choice and is associated with a high rate of cure. Since amputation can lead to a significant loss of foot function, curettage with an adequate follow-up may be considered as a preferable alternative treatment modality [3,4]. CHS is mostly resistant to chemotherapy and radiotherapy; thus, surgery is generally the preferred treatment [11]. In general, Grade 1 lesions should be discussed with intralesional curettage; high-speed motor mechanical cleaning; and adjuvant surgical methods such as cryosurgery, phenol, high temperature, and bone cement combined therapy [12,13].
CHS occurring in toes is extremely rare. In this case, extensive surgical resection of the large low-grade CHS was safe and effective. Clinical and radiologic follow-up is extremely important when malignancy is suspected. Finally, the patient should be informed about the clinical context. We offer limb salvage for CHS of the phalanx of the foot with wide resection in selected cases on the basis of clinical context.
Article summarizes an extremely rare presentation of an uncommon malignant bone tumor, its diagnosis and treatment. Such rare presentations should be managed appropriately to avoid complications and improve the quality of life of the patient. A before-hand knowledge, literature, and experience are crucial.
References
- 1.Unni KK. Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases. 5th ed. Philadelphia, PA: Lippincott-Raven; 1996. [Google Scholar | PubMed]
- 2.Bovee JV, Van Der Huel RO, Taminiau AH, Hogendoorn PC. Chondrosarcoma of the Phalanx: A locally aggressive lesion with minimal metastatic potential. A report of 35 cases and a review of the literature. Cancer 1999;86:1724-32. [Google Scholar | PubMed]
- 3.Unni KK. Cartilaginous lesions of bone. J Orthop Sci 2001;6:457-72. [Google Scholar | PubMed]
- 4.Ogose A, Unni KK, Swee RG, May GK, Rowland CM, Sim FH. Chondrosarcoma of small bones of the hands and feet. Cancer 1997;80:50-9. [Google Scholar | PubMed]
- 5.Harkless L. Soft-tissue and bone tumors. Clin Podiatr Med Surg 1993;10:587. [Google Scholar | PubMed]
- 6.Bovée JV, Cleton-Jansen AM, Taminiau AH, Hogendoorn PC. Emerging pathways in the development of Chondrosarcoma of bone and implications for targeted treatment. Lancet Oncol 2005;6:599-607. [Google Scholar | PubMed]
- 7.Evans Hl, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: A clinicopathologic analysis with emphasis on histological grading. Cancer 1977;40:818-31. [Google Scholar | PubMed]
- 8.Kinoshita GM, Matsumoto T, Maruoka M, Shiraki T, Tsunemi K, Futani H, et al. Bone and soft tissue tumors in the foot. J Bone Joint Surg Am 2002;84:216. [Google Scholar | PubMed]
- 9.Mohammadianpanah M, Torabinejad S, Bagheri MH, Omidvari S, Mosalaei A, Ahmadloo N. Primary chondrosarcoma of phalanx. Foot 2004;14:159-63. [Google Scholar | PubMed]
- 10.Wiss DA. Chondrosarcoma of the first metatarsal. J Surg Oncol 1983;23:110-2. [Google Scholar | PubMed]
- 11.Somers J, Faber LP. Chondroma and chondrosarcoma. Semin Thorac Cardiovasc Surg 1999;11:270-7. [Google Scholar | PubMed]
- 12.Hanna SA, Whittingham-Jones P, Sewell MD, Pollock RC, Skinner JA, Saifuddin A, et al. Outcome of intralesional curettage for low-grade chondrosarcoma of long bones. Eur J Surg Oncol 2009;35:1343-7. [Google Scholar | PubMed]
- 13.Mohler DG, Chiu R, McCall DA, Avedian RS. Curettage and cryosurgery for low-grade cartilage tumors is associated with low recurrence and high function. Clin Orthop Relat Res 2010;468:2765-73. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Intramuscular Glomus Tumor of Foot Presenting as Neuroma of Sural Nerve: A Case Report
August 1, 2026 Intramuscular Glomus Tumor of Foot Presenting as Neuroma of Sural Nerve: A Case Report June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study
June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report
February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report November 1, 2024 Double Trouble No More: A Case Report of En-bloc Resection and Total Hip Replacement for Secondary Hip Osteoarthritis Due to Femur Neck Osteochondroma
November 1, 2024 Double Trouble No More: A Case Report of En-bloc Resection and Total Hip Replacement for Secondary Hip Osteoarthritis Due to Femur Neck Osteochondroma