
Pectoralis major muscle rupture is a serious injury in athletes and early diagnosis is essential to obtain a good esthetic and functional outcome after surgical treatment.
Dr. Ali Alayane, Orthopedic Surgery Fellow, Department of Orthopedic Surgery, Hopital Privé de L’ouest Parisien, 14 Rue Castiglione del Lago, Trappes 78190, France. E-mail: Alyane_ali@hotmail.com
Abstract
Introduction: Pectoralis major injury is a rare injury. Its incidence increases with sports related activities. Early diagnosis is essential to obtain a satisfactory functional outcome. We present in this paper a case of 39-year-old male patient presenting with missed chronic the right pectoralis major muscle injury treated with anatomic surgical reinsertion of the muscle tendon to the humerus.
Case Report: A 39-year-old male bodybuilder patient felt a snap in his right dominant shoulder while performing bench press. Diagnosis was missed by two physicians and right shoulder MRI confirmed the diagnosis of pectoralis major muscle injury. Reinsertion of the PM muscle tendon using suture anchor was done through deltopectoral approach. Shoulder immobilization for 1 month followed by passive and active range of motion exercises results in satisfactory cosmetic and functional outcome.
Conclusion: PM muscle rupture affects mainly young male weightlifters. Loss of the anterior axillary fold is pathognomonic for PM injury. Magnetic resonance imaging of the chest wall is the gold standard examination for the diagnosis. Acute surgical repair (<6 weeks) is recommended to obtain good or excellent cosmetic and functional outcomes. Reconstruction showed lower strength and patient satisfaction; however, results were still significantly better than non-operative treatment reserved for patients with partial tears, muscle belly irreparable damage, and elderly patients with medical comorbidities whom operative treatment is not indicated.
Keywords: PM, pectoralis major, chronic rupture, young weightlifter, shoulder surgery.
The pectoralis major muscle is a strong adductor, internal rotator, and forward flexor muscle of the humerus, as well as dynamic stabilization of the shoulder [1]. It is a triangular shaped muscle that originates from the lateral border of the sternum and inferior clavicle with two major superior clavicular head (CH) and inferior sternocostal heads inserting at 4 cm distal to the greater tuberosity on the lateral lip of the bicipital groove (Fig. 1) [2]. The past anatomic studies showed that there is no folding or twisting of the muscles segments before humeral insertion; in contrast, it insets in two anterior and posterior layers. PM muscle injury was considered a rare injury [3,4], it was first described by Patissier in 1822 [5]. However, incidence and awareness of pectoralis major injuries have increased in the past 20 years with the rise of sports related activities, mainly weightlifting sports and the anabolic steroids use [5]. The aim of this paper is to report a case of 39-year-old male patient presenting with missed chronic right pectoralis major muscle injury that was treated surgically with anatomic reinsertion of the muscle to its native footprint with satisfactory functional and cosmetic outcome. We present a review of literature about this injury and a discussion of all aspect of the case.
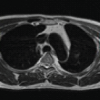
A 39-year-old male bodybuilder patient felt a snap in his right dominant shoulder while performing bench press. He immediately became aware of pain and a disruptive sensation in the right arm associated with massive swelling and ecchymosis that appeared over the medial aspect of his right upper arm. Diagnosis was missed by two physicians and the patient attended physiotherapy for 3 months without any clinical improvement. He sought medical advice 3 months after the injury complaining from persistent pain of the right shoulder, and discomfort with his daily activities. Physical examination showed obvious loss of the axillary contour and asymmetric retraction of the right pectoralis major muscle, mainly noticed by the “prayer” position (Fig. 2), associated with weakness of the right shoulder mainly in adduction and internal rotation. 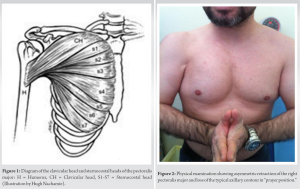 Diagnostic ultrasound of the right shoulder completed by shoulder magnetic resonance imaging (MRI) (Fig. 3), established the diagnosis of the right shoulder pectoralis major muscle rupture.
Diagnostic ultrasound of the right shoulder completed by shoulder magnetic resonance imaging (MRI) (Fig. 3), established the diagnosis of the right shoulder pectoralis major muscle rupture.  Through deltopectoral approach (Fig. 4), identification of the avulsed sternal head of the PM muscle from its humeral insertion lateral to the bicipital groove. Fibers of the CH of the pectoralis major were intact (Fig. 5).
Through deltopectoral approach (Fig. 4), identification of the avulsed sternal head of the PM muscle from its humeral insertion lateral to the bicipital groove. Fibers of the CH of the pectoralis major were intact (Fig. 5).  After dissection of scarring tissues surrounding the muscle tendon, anatomic humeral insertion of the tendon lateral to the bicipital groove was performed using two anchors with closure of the interval between the two clavicular and sternal heads with simple non-absorbable sutures. Shoulder immobilization for 1 month, followed by passive range of motion exercises for 2 weeks and active range of motion physiotherapy after 6 weeks from the surgery with satisfactory radiographic control (Fig. 6). Six months later, he returned to pre-injury level of weightlifting.
After dissection of scarring tissues surrounding the muscle tendon, anatomic humeral insertion of the tendon lateral to the bicipital groove was performed using two anchors with closure of the interval between the two clavicular and sternal heads with simple non-absorbable sutures. Shoulder immobilization for 1 month, followed by passive range of motion exercises for 2 weeks and active range of motion physiotherapy after 6 weeks from the surgery with satisfactory radiographic control (Fig. 6). Six months later, he returned to pre-injury level of weightlifting.  Twenty-four months later, the patient was very satisfied with the cosmetic and functional results without any limitation of adduction or internal rotation strength of his right upper limb.
Twenty-four months later, the patient was very satisfied with the cosmetic and functional results without any limitation of adduction or internal rotation strength of his right upper limb.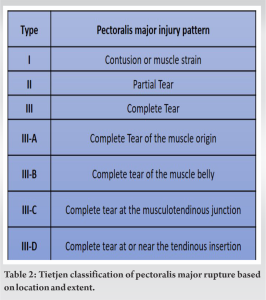
Pectoralis major muscle injury is most commonly reported in weightlifters, bodybuilders performing weight training sports [6]. The main reported mechanism of injury is sudden concentric contraction of the PM muscle during bench press exercises with the arms in abduction and external rotation position, leading to muscle rupture under tension [7]. Experimental cadaveric study reported by Wolfe et al. [8] showed that the most frequent site of PM rupture was at the musculotendinous junction; however, a meta-analysis done by Bak et al. [6] showed that insertion of the PM muscle on the humerus is the most frequent site of rupture with a 65% (Table 1) [6], this discrepancy can be explained by the age difference, because most of injuries of PM muscle insertion are found in young individuals involved in bodybuilding and weightlifting activities. Injury always involves the sternocostal head, which is the weakest inferior portion of PM, inserting, due to the normal 90° twist of the PM fibers, posterior and inferior to the CH that remains intact giving false impression about the continuity of the whole muscle attachment. The most widely used classification of the pectoralis muscle injury is the “Tietjen classification” (Table 2) [9], which grades PM injury based on the degree of the tear (contusion/partial/complete), the location of the tear (muscle origin/muscle belly/musculotendinous junction/insertion), and the chronicity of the injury. These classifications are very helpful for the decision of the appropriate treatment modality. Clinical presentation with upper limb pain, extensive soft-tissue swelling, and ecchymosis around the chest wall and the upper arm should raise the suspicion of a PM rupture. Physical examination also shows loss of the anterior axillary fold mainly seen in prayer position Fig. 2, associated with tenderness around the upper arm and weakness in adduction and internal rotation. However, acute PM injuries can be missed for months or years like our patient that presented 3 months after the injuries making the surgical treatment and rehabilitation more difficult. Standard radiographic imaging is normal except of rare cases of bony avulsion of the tendon described in the literature [10]. Ultrasound is considered a rapid and inexpensive initial screening examination of the rupture [11]; however, MRI of the chest wall with axial slices from the quadrilateral space to deltoid tuberosity is the gold standard for the diagnosis of the PM injury Fig. 3. Immobilization of the arm with a sling in an adducted and internal rotation position for 3 weeks is indicated for patients with partial muscle tears, irreparable muscle belly tears, and patients whom operative treatment is relatively contraindicated due to their age and medical comorbidities [9,12]. Surgical management is reserved for young and high demand patients with complete tears and isolated sternal head ruptures [11,13,14,15,16,17,18]. Our patient is a young active weightlifter patient with PM muscle rupture involving the sternocostal head of the muscle that needs surgical repair. Modified deltopectoral approach Fig. 4, with slight medialization of the incision for better identification of the retracted tendon is recommended [5,11]. Identification of the true superior border of the isolated sternal tears at the undersurface of the CH necessitates dissection at the inferior border of the CH and mobilization of the muscle-tendon unit with caution to avoid injury of medial pectoral nerves. Lots of surgical techniques have been described in the literature for the insertion of the pectoralis major tendon to its footprint lateral to the bicipital groove such as the use of bone tunnels, suture anchors Fig. 6, transosseous sutures, cortical button, and cortical screw fixation in rare PM muscle bony avulsion injuries [5,13,17,19]. Most of the literature clearly demonstrated that acute surgical repair of ruptured PM muscle (<6 weeks) has excellent to good results according to Bak et al. criteria [6,11], with less pain, cosmetic satisfaction, and objective strength improvement [6,8,13,14,17]. However, patients unable to have surgery report good outcomes with partial loss of adduction and decrease in torque strength [13,16,20]. Chronic pectoralis major muscle injury has been defined as injuries ranging from 3 to 8 weeks based on the muscle-tendon retraction and muscle belly atrophy that can be seen after 3 weeks from the injury [21]. Regardless the lower cosmetic and strength outcomes after chronic repair in comparison of acute repair, results of delayed repair remain acceptable and better than non-operative treatment in young active patients. The acute tear repair techniques are used in chronic cases; however, reconstruction using hamstring autograft, Achilles allograft, dermal allograft patch, and fascia lata allograft is needed in complex cases with significant muscle belly or tendon retraction and bad tissue quality [22,23]. Post-operative complications of PM repair include infection (4%), tendon re-rupture (4%), post-operative hematoma, heterotopic ossification, and proximal humerus fracture [24,25].
PM muscle rupture occurs mainly in young male individuals engaged in weightlifting sports. Pain, swelling, ecchymosis over the medial upper arm, and chest wall associated with loss of the anterior axillary fold should raise clinical suspicions of PM injury. MRI of the chest wall with axial slices from the quadrilateral space to deltoid tuberosity is the gold standard examination for the diagnosis. Acute surgical repair (<6 weeks) is recommended to obtain good or excellent cosmetic and functional outcomes without limitation of adduction or internal rotation strength. Delayed repair or reconstruction showed lower strength and patient satisfaction; however, results were still significantly better than non-operative treatment reserved for patients with partial tears, muscle belly irreparable damage, and patients whom operative treatment is relatively contraindicated due to their age and medical comorbidities.
Early diagnosis of acute Pectoralis major tendon rupture in young athletics population is essential for optimal clinical results.
References
- 1.Provencher MT, Handfield K, Boniquit NT, Reiff SN, Sekiya JK, Romeo AA. Injuries to the pectoralis major muscle: Diagnosis and management. Am J Sports Med 2010;38:1693-705. [Google Scholar | PubMed]
- 2.Fontes D, Naouri JF. Rupture traumatique du tendon de grand pectoral chez le Rugbyman. J Traumatol Sport 2007;24:161-3. [Google Scholar | PubMed]
- 3.Marmor L, Bechtol CO, Hall CB. Pectoralis major muscle. J Bone Joint Surg Am 1961;43:81-7. [Google Scholar | PubMed]
- 4.McEntire JE, Hess WE, Coleman SS. Rupture of the pectoralis major muscle. A report of eleven injuries and review of fifty-six. J Bone Joint Surg Am 1972;54:1040-6. [Google Scholar | PubMed]
- 5.Metzger PD, Bailey JR, Filler RD, Waltz RA, Provencher MT, Dewing CB. Pectoralis major muscle rupture repair: Technique using unicortical buttons. Arthrosc Tech 2012;1:e119-25. [Google Scholar | PubMed]
- 6.Bak K, Cameron EA, Henderson IJ. Rupture of the pectoralis major: A meta-analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc 2000;8:113-9. [Google Scholar | PubMed]
- 7.Reut RC, Bach BR, Johnson C. Pectoralis major rupture. Diagnosing and treating a weight-training injury. Phys Sportsmed 1991;19:89-96. [Google Scholar | PubMed]
- 8.Wolfe SW, Wickiewicz TL, Cavanaugh JT. Ruptures of the pectoralis major muscle. An anatomic and clinical analysis. Am J Sports Med 1992;20:587-93. [Google Scholar | PubMed]
- 9.Tietjen R. Closed injuries of the pectoralis major muscle. J Trauma 1980;20:262-4. [Google Scholar | PubMed]
- 10.Verfaillie SM, Claes T. Bony avulsion of the pectoralis major muscle. J Shoulder Elbow Surg 1996;5:327-9. [Google Scholar | PubMed]
- 11.Thompson K, Kwon Y, Flatow E, Jazrawi L, Strauss E, Alaia M. Everything pectoralis major: From repair to transfer. Phys Sportsmed 2020;48:33-45. [Google Scholar | PubMed]
- 12.Petilon J, Carr DR, Sekiya JK, Unger DV. Pectoralis major muscle injuries: Evaluation and management. J Am Acad Orthop Surg 2005;13:59-68. [Google Scholar | PubMed]
- 13.Schepsis AA, Grafe MW, Jones HP, Lemos MJ. Rupture of the pectoralis major muscle. Outcome after repair of acute and chronic injuries. Am J Sports Med 2000;28:9-15. [Google Scholar | PubMed]
- 14.Hanna CM, Glenny AB, Stanley SN, Caughey MA. Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-6. [Google Scholar | PubMed]
- 15.Antosh IJ, Grassbaugh JA, Parada SA, Arrington ED. Pectoralis major tendon repairs in the active-duty population. Am J Orthop (Belle Mead NJ) 2009;38:26-30. [Google Scholar | PubMed]
- 16.de Castro Pochini A, Andreoli CV, Belangero PS, Figueiredo EA, Terra BB, Cohen C, et al. Clinical considerations for the surgical treatment of pectoralis major muscle ruptures based on 60 cases: A prospective study and literature review. Am J Sports Med 2014;42:95-102. [Google Scholar | PubMed]
- 17.Haley CA, Zacchilli MA. Pectoralis major injuries: Evaluation and treatment. Clin Sports Med 2014;33:739-56. [Google Scholar | PubMed]
- 18.Butt U, Mehta S, Funk L, Monga P. Pectoralis major ruptures: A review of current management. J Shoulder Elbow Surg 2015;24:655-62. [Google Scholar | PubMed]
- 19.Merolla G, Paladini P, Campi F, Porcellini G. Pectoralis major tendon rupture. Surgical procedures review. Muscles Ligaments Tendons J 2012;2:96-103. [Google Scholar | PubMed]
- 20.Aärimaa V, Rantanen J, Heikkilä J, Helttula I, Orava S. Rupture of the pectoralis major muscle. Am J Sports Med 2004;32:1256-62. [Google Scholar | PubMed]
- 21.Kakwani RG, Matthews JJ, Kumar KM, Pimpalnerkar A, Mohtadi N. Rupture of the pectoralis major muscle: Surgical treatment in athletes. Int Orthop 2007;31:159-63. [Google Scholar | PubMed]
- 22.Joseph TA, Defranco MJ, Weiker GG. Delayed repair of a pectoralis major tendon rupture with allograft: A case report. J Shoulder Elbow Surg 2003;12:101-4. [Google Scholar | PubMed]
- 23.Zafra M, Muñoz F, Carpintero P. Chronic rupture of the pectoralis major muscle: Report of two cases. Acta Orthop Belg 2005;71:107-10. [Google Scholar | PubMed]
- 24.Gautschi OP, Zellweger R. A complete tear of the pectoralis major muscle from a seat belt injury. Eur J Emerg Med 2007;14:90-1. [Google Scholar | PubMed]
- 25.Silverstein JA, Goldberg B, Wolin P. Proximal humerus shaft fracture after pectoralis major tendon rupture repair. Orthopedics 2011;34:222. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report
June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report January 1, 2025 Chronic Rupture of the Pectoralis Major: Current Concepts and Various Surgical Repair Techniques – A Mini Review
January 1, 2025 Chronic Rupture of the Pectoralis Major: Current Concepts and Various Surgical Repair Techniques – A Mini Review August 6, 2024 Rupture of Pectoralis Major Muscle: A Case Report
August 6, 2024 Rupture of Pectoralis Major Muscle: A Case Report August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report