
Strategies for diagnosis, treatment, and prevention of multiple finger extensor tendon attritional ruptures following volar plating of the distal radius.
Dr. Jonathan Persitz, Hand Program, Division of Plastic, Reconstructive and Aesthetic Surgery, University Health Network, Toronto Western Hospital, affiliated with University of Toronto, Temerty Faculty of Medicine, Toronto, Ontario, Canada. E-mail: yonipersitz@gmail.com
Abstract
Introduction: Hardware prominence is one of the major established complications following volar plating of distal radius fractures. In particular, dorsal prominence of screws is the leading risk factor associated with post-surgical extensor pollicis longus (EPL) tendon rupture. Although there are many descriptions of attritional EPL ruptures in the literature, concomitant presentation of attritional EPL and extensor digitorum communis (EDC) ruptures following volar plating of distal radius fractures are minimal.
Case Report: We present a case of concomitant rupture of the EPL and occult rupture of the EDC to the index finger following volar plating of the distal radius. This was discovered intraoperatively and complicated the proposed tendon transfer reconstruction.
Conclusion: Locked volar plate fixation has become the preferred technique for surgical management of distal radius fractures. The complication of multiple extensor tendon ruptures is rare but nevertheless may be encountered. We discuss strategies for diagnosis, treatment, and prevention. Surgeons should be aware of and prepared to proceed with alternative reconstructive procedures if this complication is discovered.
Keywords: Distal radius fracture, tendon transfer, extensor pollicis longus, extensor indicis proprius, extensor digitorum communis, tendon rupture.
Distal radius fractures are among the most common injuries encountered by orthopedic surgeons. When indicated, surgical management with volar locking plates has become increasingly popular. Benefits to this type of fixation include soft tissue coverage of the plate, stable fixation in poor quality bone, and the possibility for early mobilization. Despite this, there are several well-described complications including flexor and extensor tendon irritation or rupture, loss of reduction, hardware failure, and neurovascular injury [1]. Although extensor tendon rupture is a rare complication, involvement of the extensor pollicis longus (EPL) tendon is most common, occurring in approximately 3.3–8.6% of surgical cases treated with volar locking plates [1,2,3] and in up to 5% of non-surgical cases [2,4,5,6]. When this complication results in significant functional deficit, transfer of the extensor indicis proprius (EIP) has become the treatment of choice for delayed reconstruction [7]. Rupture of the fourth extensor compartment tendons has also been described and is generally attributed to tendon irritation by screws penetrating the dorsal cortex after surgery [1,2,8,9]. In this study, we present a case of concomitant EPL and extensor digitorum communis (EDC) to the index finger (EDC II) tendon rupture after locked volar plating of the distal radius. The purpose of this article is to describe this complication as well as strategies for diagnosis, treatment, and prevention.
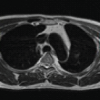
A 48-year-old, right hand dominant female sustained a fracture of the left distal radius. She underwent open reduction and internal fixation 10 days after injury with a volar locking plate. Approximately 2 months after surgery, she described a “pop” in the wrist and was subsequently unable to extend the thumb out of the plane of the palm. She continued with rehabilitation but eventually presented to our institution due to persistent limited range of motion (ROM) 3 months post-operatively. Clinical evaluation confirmed deficiency of the EPL tendon while extension to the remaining digits was maintained (including independent extension of the index and small fingers). Radiographs revealed solid union of the fracture and a volar plate with prominent dorsal screws (Fig. 1).  Magnetic resonance imaging (MRI) was performed by the referring physician, but this was of limited utility due to metal artifact from the plate and screws. As a result, the musculoskeletal radiologist report could not conclusively confirm continuity or discontinuity of the extensor tendons. After our initial evaluation, treatment options were discussed and surgical management involving hardware removal and EIP to EPL transfer to restore thumb extension was offered. Informed consent was obtained in accordance with our institutional guidelines. At the time of surgery, the previous volar incision was utilized, and all hardware was removed. An incision was then made dorsally over the metacarpophalangeal (MCP) joint of the thumb and the EPL tendon was isolated and confirmed to have sustained an attritional tear. A second dorsal incision was made at the level of the index MCP joint and the EIP and EDC II tendons were identified. The EIP was isolated and transected just proximal to the extensor hood. A third incision was made to retrieve the EIP tendon at the level of the wrist, just ulnar to Lister’s tubercle. During EIP retrieval, the fourth extensor compartment tendons were identified, and exploration revealed a concomitant attritional rupture of the EDC II tendon at this level. The proximal stump of the EDC II had retracted and was of insufficient quality and mobility to perform a direct repair. The remaining tendons were explored and found to be intact. This finding left a deficit in extension of both the thumb and index finger as the EIP tendon was transected distally for the planned transfer. As such, we elected to proceed with EIP to EPL tendon transfer to restore thumb extension. In addition, a weaved end-to-side transfer of the EDC II to the long finger (EDC III) was performed to restore index finger extension, with tensioning to recreate normal digital cascade. Both transfers were performed using a Pulvertaft weave technique and secured with non-absorbable braided suture. After wound closure, the patient was placed in a thumb spica and a volar resting splint to maintain full extension of the index finger and full radial abduction and extension of the thumb. At 2 weeks, the patient was provided with a custom thermoplastic splint to protect the repairs and started gentle ROM using wrist tenodesis. Starting at 6 weeks, she was gradually progressed through further rehabilitation as tolerated with stretching and strengthening exercises without formal limitation on IP, MCP, or CMC ROM. At 12-month post-operatively, the patient had obtained full ROM with regard to the thumb and index finger and had returned to full activities without restriction (Fig. 2 and 3).
Magnetic resonance imaging (MRI) was performed by the referring physician, but this was of limited utility due to metal artifact from the plate and screws. As a result, the musculoskeletal radiologist report could not conclusively confirm continuity or discontinuity of the extensor tendons. After our initial evaluation, treatment options were discussed and surgical management involving hardware removal and EIP to EPL transfer to restore thumb extension was offered. Informed consent was obtained in accordance with our institutional guidelines. At the time of surgery, the previous volar incision was utilized, and all hardware was removed. An incision was then made dorsally over the metacarpophalangeal (MCP) joint of the thumb and the EPL tendon was isolated and confirmed to have sustained an attritional tear. A second dorsal incision was made at the level of the index MCP joint and the EIP and EDC II tendons were identified. The EIP was isolated and transected just proximal to the extensor hood. A third incision was made to retrieve the EIP tendon at the level of the wrist, just ulnar to Lister’s tubercle. During EIP retrieval, the fourth extensor compartment tendons were identified, and exploration revealed a concomitant attritional rupture of the EDC II tendon at this level. The proximal stump of the EDC II had retracted and was of insufficient quality and mobility to perform a direct repair. The remaining tendons were explored and found to be intact. This finding left a deficit in extension of both the thumb and index finger as the EIP tendon was transected distally for the planned transfer. As such, we elected to proceed with EIP to EPL tendon transfer to restore thumb extension. In addition, a weaved end-to-side transfer of the EDC II to the long finger (EDC III) was performed to restore index finger extension, with tensioning to recreate normal digital cascade. Both transfers were performed using a Pulvertaft weave technique and secured with non-absorbable braided suture. After wound closure, the patient was placed in a thumb spica and a volar resting splint to maintain full extension of the index finger and full radial abduction and extension of the thumb. At 2 weeks, the patient was provided with a custom thermoplastic splint to protect the repairs and started gentle ROM using wrist tenodesis. Starting at 6 weeks, she was gradually progressed through further rehabilitation as tolerated with stretching and strengthening exercises without formal limitation on IP, MCP, or CMC ROM. At 12-month post-operatively, the patient had obtained full ROM with regard to the thumb and index finger and had returned to full activities without restriction (Fig. 2 and 3).
Rupture of the EPL tendon is a well-documented complication after distal radius fracture. It has previously been described with both cast immobilization and surgical management. This likely has to do with a combination of factors including impingement at the time of injury, mechanical irritation from fracture fragments and tendon subluxation, ischemia of the EPL at its watershed zone adjacent to Lister’s tubercle secondary to hematoma or direct trauma, and tendon sheath inflammation [10,11]. Surgically, drill bit penetration, prominent screws, and hardware impingement can further contribute to tendon irritation and the risk of rupture. Unlike the EPL tendon, rupture of the 4th extensor compartment tendons has been rarely described with non-surgical management. EDC attritional tear cases reported in the literature are limited and have generally been associated with dorsal penetrating screws, drill bit, and bony spurs [2,8,9,12]. The rare occurrence of EDC tendon rupture may be in part due to the fact that these tendons are in a larger compartment and may not be subject to the same mechanical or ischemic injury that is experienced by the relatively constrained EPL. To the best of our knowledge, concomitant rupture of the EPL and EDC II tendon has only been described twice previously. In the first article by de Boer, reconstruction of the EPL tendon was not performed after attritional rupture associated with non-surgical treatment of the distal radius fracture [13]. In 2020, a more recent publication by Bhardwaj et al. presented 2 patients with EPL and EDC II attritional tears after distal radius fracture. The first patient had a typical EPL rupture associated with prominent hardware treated with EIP to EPL transfer and hardware removal. The patient subsequently had a delayed presentation of rupture of the reconstructed EPL as well as EDC II presenting with a lack of thumb and index finger extension; this was treated with a side hitching of the index finger EDC to middle finger EDC and palmaris longus to EPL transfer with hemi-flexor carpi radialis graft. The second patient sustained an attritional rupture of EPL and EDC II around 6 years after volar plating of a distal radius fracture, the occult EDC II rupture was only identified at the time of surgery, but in this case, it was found prior EIP harvest. Given this, they were able to reconstruct EPL with intertendinous grafting using ipsilateral palmaris longus graft without sacrificing the EIP as the solo index finger extensor [12]. Another case report described concomitant rupture of the EPL and EDC III tendons; however, in this case, EIP to EPL transfer could still be performed without compromising index finger function [14]. Redundant index finger extension (with intact EIP and EDC II) is a prerequisite for reconstruction of the EPL with EIP transfer. Clinically, integrity of the EIP tendon can be confirmed with the presence of independent index finger extension. EDC II tendon rupture, however, is less reliably assessed and in this case was occult until discovered intraoperatively. Given that previous volar plating with prominent screws may be a risk factor for EDC tendon injury, we recommend exploration of the 4th extensor compartment tendons and confirmation of intact EDC II before proceeding with transfer of the EIP tendon. This is particularly important when previous internal fixation has been performed and there is clinical and/or radiographic concern regarding prominent hardware. Pre-operatively, dynamic ultrasound may be a more reliable modality than MRI for diagnosis given the issue of metal artifact and may be a more cost-effective pre-operative imaging modality than MRI. If an EDC II tendon rupture is found at the time of surgery, reconstruction may be performed as described in this case. Alternatively, if the EIP has not already been released distally, other EPL reconstruction options described in the literature are either grafting using palmaris longus, toe extensors, and fasciolata or tendon transfers using the extensor carpi radialis brevis, extensor carpi radialis longus, or the brachioradialis [7,15]. With respect to prevention, avoiding prominent dorsal screw penetration is most critical. Previous biomechanical studies have demonstrated that bicortical fixation is not essential with locked volar plating for extra-articular fractures and screws of 75% of bicortical length result in equal construct stiffness [16]. We routinely place screws approximately 2 mm less than the measured bicortical length. However, for intra-articular fractures, bicortical fixation may be desirable to capture specific dorsal fragments. In these cases, careful assessment of screw length is paramount. Intraoperative imaging using pronation and supination views and the dorsal horizon view can prevent screw prominence due to superposition of Lister’s tubercle on conventional lateral imaging [17]. In addition, post-operative ultrasound has shown excellent sensitivity for detection of prominent dorsal hardware compared to fluoroscopy [18,19]. Hardware removal should be considered in cases where clinical concern of tendon irritation is encountered, or significant prominence of dorsal hardware exists.
The complication of multiple extensor tendon ruptures is rare following distal radius fractures, but nevertheless may be encountered when treating patients with previous volar plating has been performed. Surgeons should be mindful of this possibility when performing EIP to EPL transfer and discuss this in the informed consent process. Pre-operative ultrasound examination and/or careful intraoperative examination of the integrity of the EDC tendons preceding an EIP harvest will prevent missed injuries and simplify reconstructive decision making. Surgeons should be aware of and prepared to proceed with alternative reconstructive procedures if this complication is discovered.
Surgeons should be mindful of multiple extensor tendon attritional ruptures following volar plating of distal radius fractures, especially when planning EIP to EPL tendon. Meticulous surgical technique for volar plating and ensuring proper screw length may avoid this complication.
References
- 1.Rampoldi M, Marsico S. Complications of volar plating of distal radius fractures. Acta Orthop Belg 2007;73:714-9. [Google Scholar | PubMed]
- 2.Al-Rashid M, Theivendran K, Craigen MA. Delayed ruptures of the extensor tendon secondary to the use of volar locking compression plates for distal radial fractures. J Bone Joint Surg Br 2006;88:1610-2. [Google Scholar | PubMed]
- 3.Zwetkow AN, Schibli S, Canova MA, Mark GI, Sommer C. Rupture of the extensor tendons: A complication following volar locking compression plate osteosynthesis of the distal radius. Br J Surg 2005;92:900-18. [Google Scholar | PubMed]
- 4.Cooney WP 3rd, Dobyns JH, Linscheid RL. Complications of Colles’ fractures. J Bone Joint Surg Am 1980;62:613-9. [Google Scholar | PubMed]
- 5.Lidstrom A. Fractures of the distal end of the radius. A clinical and statistical study of end results. Acta Orthop Scand Suppl 1959;41:1-118. [Google Scholar | PubMed]
- 6.Roth KM, Blazar PE, Earp BE, Han R, Leung A. Incidence of extensor pollicis longus tendon rupture after nondisplaced distal radius fractures. J Hand Surg Am 2012;37:942-7. [Google Scholar | PubMed]
- 7.Gelb RI. Tendon transfer for rupture of the extensor pollicis longus. Hand Clin 1995;11:411-22. [Google Scholar | PubMed]
- 8.Hattori Y, Doi K, Sakamoto S, Yukata K. Delayed rupture of extensor digitorum communis tendon following volar plating of distal radius fracture. Hand Surg 2008;13:183-5. [Google Scholar | PubMed]
- 9.Ward JP, Kim LT, Rettig ME. Extensor indicis proprius and extensor digitorum communis rupture after volar locked plating of the distal radius--a case report. Bull NYU Hosp Jt Dis 2012;70:273-5. [Google Scholar | PubMed]
- 10.Ferreres A, Llusá M, García-Elías M, Lluch A. A possible mechanism of direct injury to the EPL tendon at Lister’s tubercle during falls with the wrist fully extended. J Hand Surg Eur Vol 2008;33:149-51. [Google Scholar | PubMed]
- 11.Owers KL, Lee J, Khan N, Healy J, Eckersley R. Ultrasound changes in the extensor pollicis longus tendon following fractures of the distal radius--a preliminary report. J Hand Surg Eur Vol 2007;32:467-71. [Google Scholar | PubMed]
- 12.Bhardwaj P, Varadharajan V, Sabapathy SR. Concomitant rupture of extensor pollicis longus and index extensor tendons following distal radius plating-report of two cases and their clinical implication for tendon transfer surgery. Indian J Plast Surg 2020;53:435-8. [Google Scholar | PubMed]
- 13.de Boer SW, van Kooten EO, Ritt MJ. Extensor pollicis longus tendon rupture with concomitant rupture of the extensor digitorum communis II tendon after distal radius fracture. J Hand Surg Eur Vol 2010;35:679-81. [Google Scholar | PubMed]
- 14.Sadr B. Sequential rupture of extensor tendons after a Colles fracture. J Hand Surg Am 1984;9A:144-5. [Google Scholar | PubMed]
- 15.Ganon S, Bellity J, Zbili D, Boccara D. Reconstruction strategies after rupture of the extensor pollicis longus tendon: A systematic review. Hand Surg Rehabil 2020;39:502-7. [Google Scholar | PubMed]
- 16.Wall LB, Brodt MD, Silva MJ, Boyer MI, Calfee RP. The effects of screw length on stability of simulated osteoporotic distal radius fractures fixed with volar locking plates. J Hand Surg Am 2012;37:446-53. [Google Scholar | PubMed]
- 17.Joseph SJ, Harvey JN. The dorsal horizon view: Detecting screw protrusion at the distal radius. J Hand Surg Am 2011;36:1691-3. [Google Scholar | PubMed]
- 18.Watchmaker JD, Daley RA, Watchmaker GP, Grindel SI. Ultrasound imaging improves identification of prominent hardware in the surgical treatment of distal radius fractures: A cadaveric and prospective clinical study. J Wrist Surg 2016;5:36-41. [Google Scholar | PubMed]
- 19.Williams D, Singh J, Heidari N, Ahmad M, Noorani A, Di Mascio L. Assessment of penetration of dorsal screws after fixation of the distal radius using ultrasound: Cadaveric study. Ann R Coll Surg Engl 2016;98:138-42. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report
June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report June 1, 2026 Nonvascularized Iliac Crest Autograft for Wrist and Hand Reconstructions: A Report of Two Clinical Cases and Literature Review
June 1, 2026 Nonvascularized Iliac Crest Autograft for Wrist and Hand Reconstructions: A Report of Two Clinical Cases and Literature Review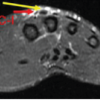 June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report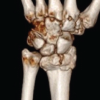 March 1, 2026 An Economically Feasible Solution for Distal Radius Fractures Treated with Column-specific Fixation
March 1, 2026 An Economically Feasible Solution for Distal Radius Fractures Treated with Column-specific Fixation