
Anterior screw fixation can be considered a preferred treatment for Type II odontoid fractures.
Dr. Karthik Loganathan, Department of Orthopaedics, Government Stanley Medical College Hospital, Chennai, Tamil Nadu, India. E-mail: karindu1989@gmail.com
Introduction: Fractures of the odontoid process are common cervical spine injuries, accounting for 10–20% of all cervical spine fractures. Anterior screw fixation of odontoid fractures is an osteosynthetic technique that can give immediate stability and preserve normal mobility.
Case Series: The study was conducted in Government Mohan Kumaramangalam Medical college in the period 2017–2020. Five patients with Anderson and D’Alonzo type II odontoid Fractures were included in the study. Through anterior approach, using a horizontal skin incision, a K wire is inserted from the inferior edge of C2 through the incision and impacted into the odontoid process. A cannulated screw with non-threaded proximal shaft is inserted and tightened firmly to allow the distal fragment to compress on the body of C2. All the patients were reviewed postoperatively at 3, 6, and 12 months. Out of the five patients, all the patients had successful anatomical union at the end of 16 weeks. No neurological sequelae were reported.
Discussion: Anterior screw fixation provides a reasonable approach to odontoid fractures. Posterior stabilization using multiple techniques has been described with good union rates but has several disadvantages. Anterior screw fixation provides direct fracture fixation without the need for bone grafts. In addition, it reduces post-operative discomfort and length of hospital stay.
Conclusion: Anterior odontoid screw fixation was associated with relatively low complication rates and a high union rate in our study. We conclude that this shall be the preferred treatment method for Type II odontoid fractures.
Keywords: Odontoid, anterior screw fixation, cervical spine injuries.
Fractures of the odontoid process are common fractures among the injuries of cervical spine. 10–20% of all cervical spine fractures are attributed to odontoid fractures. Some type of odontoid fractures can even cause instability of the atlantoaxial complex and may lead to spinal cord damage [1]. The most commonest type is the type II which occurs at the junction of odontoid process and C2 vertebral body. It may also result in instability at the atlantoaxial joint. The fractured odontoid process may get displaced in anterior or posterior direction. Because of the complications associated with this fracture, achieving spinal stabilization is imperative. Anterior screw fixation of odontoid fractures is an unique technique. It provides absolute stability and can also preserve mobility in the atlantoaxial joint. (Fig. 1).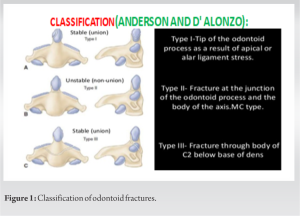
The study was conducted in Government Mohan kumaramangalam medical college hospital in the period of 2017–2020. Five patients with Anderson and D’Alonzo type II odontoid Fractures were included in the study. All patients underwent preoperative evaluation. Evaluation is done by plain x-rays of the cervical spine in AP and lateral positions. Open mouth view is also obtained. Computed tomography of the cervical spine is highly recommended [2, 3, 4]. Magnetic resonance imaging can also be used to visualize the neurological structures and the transverse ligament [3, 5]. The neurological status of the patient is also assessed preoperatively .
Operative Technique
The patient is placed in supine position with mouth open. The C-arm is positioned in such a way that the odontoid is visible in AP and lateral view. Using a horizontal skin incision through anterior approach in the mid-cervical region, platysma is divided and retracted to reach the anterior surface of the vertebral column. The longus coli muscle is identified. An incision is made over the fascia in midline, and the longus coli muscle is separated to expose the body of vertebra. Bluntly develop the prevertebral space along the front of cervical spine till the lower part of the body of axis is reached. Using a drill sleeve insert one 1.2 mm K wire is inserted in the midline in AP view. On the lateral view, wire entry is at the anterior edge of the end plate, and the wire is advanced into the odontoid process across the fracture. Insert a cannulated drill bit over the k wire and drill for the appropriate length up to the tip of odontoid process. Drill is removed and depth measured and tapped. Based on the measured depth, a 4.0 mm cannulated screw is inserted and tightened firmly to allow compression at the fracture site. Platysma and other layers are closed with a drain. Philadelphia collar was advised until union was achieved. All the patients were reviewed postoperatively at 3, 6, and 12 months.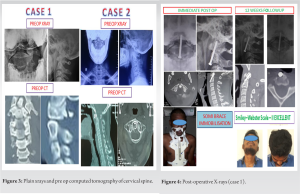 Neck mobilization exercises started after radiological union.
Neck mobilization exercises started after radiological union.  Functional outcome was measured using Smiley-Webster scale. Out of the five patients, all the patients had successful anatomical union at the end of 16 weeks. The union rate was 100%. There were no intra-operative complications. No neurological sequelae related to the screw fixation. No complications of infection or hematoma were seen. (Fig .3-5). (Table 1).
Functional outcome was measured using Smiley-Webster scale. Out of the five patients, all the patients had successful anatomical union at the end of 16 weeks. The union rate was 100%. There were no intra-operative complications. No neurological sequelae related to the screw fixation. No complications of infection or hematoma were seen. (Fig .3-5). (Table 1).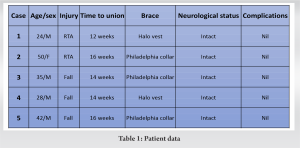
Anderson and D’Alonzo classification is the widely used classification for fractures of the odontoid. He classified it into three types. Among that, Type II is the most common type and involves the neck of odontoid process. This type of fracture also has high degree of instability. The odontoid process may be displaced anteriorly or posteriorly in relation to C2 vertebral body. In a study done by Apfelbaum et al., he has classified Type II fractures into anterior oblique, horizontal, or posterior oblique types [2]. The slope of the fracture line is an important parameter in the treatment. Anterior oblique fractures have less union rates when treated with an anterior odontoid screw [2].
Mortality and neurological injury
Odontoid fractures typically have a mortality rate under 40% [6, 7]. The majority of cases lack any neurological signs. In the research by Anderson and D’alonzo [8], it was discovered that 25% of the patients had Brown-Sequard syndrome, minimal upper limb weakness, decreased sensation in the occipital region, and exaggerated reflexes in the lower limbs. It has also been documented that symptoms can appear with a late onset [1, 9]. Neck discomfort is the most typical symptom, but stiffness and weakness have also been noted in some cases [1]. Orthoses have been used to heal Type I and Type III fractures, and the results have been promising. Immobilization and traction are not thought to be effective treatment for type I and III fractures. According to the study by Julien et al.’s [10], the union rate for type II fractures treated with cervical traction and collar immobilization was about 56%. When immobilization with a Halo vest device was used, non-union rate ranged from 7% to 100% [11, 12]. In some studies [13, 14], non-union rates ranging from 21% to 45% have been recorded. Treatment of odontoid fractures without surgery has very significant nonunion rates. Pseudo arthrosis or nonunion are the outcomes of inadequate stability at the fracture site. When immobilization with an orthosis was either impossible to use or had failed in the past, posterior neck fusion was performed. Brooks, Gallie, and later Dickman and Sonntag have all outlined posterior stabilization using a variety of methods. In a study by Dickman [15], he found fusion rates of more than 90% for fixation using trans articular screws and union rates of almost 80% for posterior fusion with wiring. The use of wire in posterior fusion techniques may damage neurological systems. All posterior procedures also need bone grafts to achieve adequate stability, which increases the risk of complications after surgery. A C1-2 joint fusion may result in reduction of rotational movement of almost 50%. Anterior odontoid screw fixation method, a more recent development that shows promise, has emerged recently to preserve the atlantoaxial joint’s normal range of motion. A study by Chiba et al. [16] described the anterior odontoid screw fixation method. Numerous writers have also discussed a similar screw fixation technique [17, 18, 19, 20, 21, 22]. Due to new developments in the use of fluoroscopy and other minimally invasive techniques, this approach has been improved and perfected [23, 24]. In contrast to posterior operations, this method offers direct fracture fixation. In a research by Montesano et al. [25] around 80% of the movements were preserved. Additionally, it shortens hospital stays and post-operative pain. For the operation to be carried out properly, a sufficient preoperative evaluation must be completed. The use of anterior screws allows for quick patient mobilization and little post-operative discomfort.
The most common fractures of the axis are those involving the odontoid process. Anderson and D’Alonso Type II fractures are the most common among them and are often best treated with surgery. Anterior screw fixation offers the patient early mobilization, less post-operative pain and a high union rate, compared to all the other available surgical techniques. It also provides direct fracture fixation without bone grafts. In our study this technique has shown low complication rate and high success rate. We conclude that anterior screw fixation can be considered as the preferred treatment method for Type II odontoid fractures.
Anterior odontoid screw fixation is a simple and effective technique for treatment of odontoid fractures.
References
- 1.Crockard HA, Heilman AE, Stevens JM. Progressive myelopathy secondary to odontoid fractures: Clinical, radiological, and surgical features. J Neurosurg 1993;78:579-86. [Google Scholar]
- 2.Apfelbaum RI, Lonser RR, Veres R, Casey A. Direct anterior screw fixation for recent and remote odontoid fractures. J Neurosurg 2000;93:227-36. [Google Scholar]
- 3.Deliganis AV, Baxter AB, Hanson JA, Fisher DJ, Cohen WA, Wilson AJ, et al. Radiologic spectrum of craniocervical distraction injuries. Radiographics 2000;20:S237-50. [Google Scholar]
- 4.Nepper-Rasmussen J. CT of dens axis fractures. Neuroradiology 1989;31:104-6. [Google Scholar]
- 5.Dickman CA, Sonntag VK. Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1997;40:886-7. [Google Scholar]
- 6.Bucholz RW, Burkhead WZ, Graham W, Petty C. Occult cervical spine injuries in fatal traffic accidents. J Trauma 1979;19:768-71. [Google Scholar]
- 7.Huelke DF, O'Day J, Mendelsohn RA. Cervical injuries suffered in automobile crashes. J Neurosurg 1981;54:316-22. [Google Scholar]
- 8.Anderson LD, D'Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg Am 1974;56:1663-74. [Google Scholar]
- 9.Fairholm D, Lee ST, Lui TN. Fractured odontoid: The management of delayed neurological symptoms. Neurosurgery 1996;38:38-43. [Google Scholar]
- 10.Julien TD, Frankel B, Traynelis VC, Ryken TC. Evidence-based analysis of odontoid fracture management. Neurosurg Focus 2000;8:e1. [Google Scholar]
- 11.Maiman DJ, Larson SJ. Management of odontoid fractures. Neurosurgery 1982;11:820. [Google Scholar]
- 12.Lind B, Nordwall A, Sihlbom H. Odontoid fractures treated with halo-vest. Spine (Phila Pa 1976) 1987;12:173-7. [Google Scholar]
- 13.Dickson H, Engel S, Blum P, Jones RF. Odontoid fractures, systemic disease and conservative care. Aust N Z J Surg 1984;54:243-7. [Google Scholar]
- 14.Fujii E, Kobayashi K, Hirabayashi K. Treatment in fractures of the odontoid process. Spine (Phila Pa 1976) 1988;13:604-9. [Google Scholar]
- 15.Dickman CA, Foley KT, Sonntag VK, Smith MM. Cannulated screws for odontoid screw fixation and atlantoaxial transarticular screw fixation. Technical note. J Neurosurg 1995;83:1095-100. [Google Scholar]
- 16.Chiba K, Fujimura Y, Toyama Y, Takahata T, Nakanishi T, Hirabayashi K. Anterior screw fixation for odontoid fracture: Clinical results in 45 cases. Eur Spine J 1993;2:76-81. [Google Scholar]
- 17.Borne GM, Bedou GL, Pinaudeau M, Cristino G, Hussein A. Odontoid process fracture osteosynthesis with a direct screw fixation technique in nine consecutive cases. J Neurosurg 1988;68:223-6. [Google Scholar]
- 18.Apfelbaum RI. Anterior screw fixation of odontoid fractures. In: Rengachary SS, Wilkins RH, editors. Neurosurgical Operative Atlas. 2nd ed. Baltimore: Williams and Wilkins; 1992. p. 189-99. [Google Scholar]
- 19.Böhler J. Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27. [Google Scholar]
- 20.Esses SI, Bednar DA. Screw fixation of odontoid fractures and nonunions. Spine (Phila Pa 1976) 1991;16:S483-5. [Google Scholar]
- 21.Geisler FH, Cheng C, Poka A, Brumback RJ. Anterior screw fixation of posteriorly displaced type II odontoid fractures. Neurosurgery 1989;25:30-7. [Google Scholar]
- 22.Lesoin F, Biondi A, Jomin M. Foraminal cervical herniated disc treated by anterior discoforaminotomy. Neurosurgery 1987;21:334-8. [Google Scholar]
- 23.Aebi M, Etter C, Coscia M. Fractures of the odontoid process. Treatment with anterior screw fixation. Spine (Phila Pa 1976) 1989;14:1065-70. [Google Scholar]
- 24.Apfelbaum RI. Neurosurgical Operative Atlas. Park Ridge, Ill, and Baltimore: American Association of Neurological Surgeons and Williams & Wilkins; 1991. [Google Scholar]
- 25.Montesano PX, Anderson PA, Schlehr F, Thalgott JS, Lowrey G. Odontoid fractures treated by anterior odontoid screw fixation. Spine (Phila Pa 1976) 1991;16:S33-7. [Google Scholar]




