
Talus fractures are relatively uncommon injuries. Even though the fracture is evident in plain radiographs, a mandatory CT scan is helpful to know the plane of fracture line and to plan specific treatment. Internal fixation is helpful to restore the subtalar and ankle joint mechanics and allow early rehabilitation.
Dr. Rajesh Kumar Vemparala, Department of Orthopaedics, Athani Hospitals, Palakkad, Kerala, India. E-mail: drrajesh086@gmail.com
Introduction: Talus fractures are relatively rare injuries .These injuries are very serious because they can compromise the motion of foot and ankle and result in severe disability . Fractures of talar neck and body constitutes about 40% of all talus fractures. These occur secondary to high energy trauma most commonly motor vehicle collisions or fall from height . Fractures involving the lateral process results due to ankle inversion and dorsiflexion . Majority of talar surface is covered by articular cartilage and its role in force transmission between leg and foot makes successful treatment of such injuries a mandatory prerequisite to regain function. We present an atypical case of talus fracture in which fracture plane extends from posterior aspect of lateral talar process involving the body in coronal plane . Not much of literature has been published in this regard.
Case Report: A 28 year old male presented with pain in the left ankle following fall from a tree. Following the radiological investigations, in coronal plane fracture line extends from posterior aspect of lateral talar process into the body medially and anteriorly. Internal fixation of the fracture was done by an open approach and a strict rehabilitation protocol was followed. At three months the patient had satisfactory healing of fracture without any irregularity of the articular surface and ambulant pain free with full range of ankle movements .
Conclusion: There are several choices to treat talar fractures . The ideal treatment should be customized as per the fracture morphology . Open reduction and internal fixation is one of the best options to restore the tibiotalar and subtalar joint congruency and to prevent post traumatic arthritis . Appropriate diagnosis and perioperative treatment is the key to success in talar fracture management.
Keywords: Talar body fracture, lateral process, subtalar joint.
Talus fractures are uncommon injuries with the incidence of 0.1–0.85% of all fractures [1]. Talus is unique in having tenuous vascular supply and 60–70% of talar surface covered by articular cartilage but no muscle attachment. [2]. These are always associated with high-velocity injuries most frequent being road traffic accidents followed by fall from height. The prevalence rate for male : female is 4.8:1 [3]. Multiple articulations, tenuous blood supply, and complex structures create particular difficulty in achieving acceptable outcome even with optimal treatment therefore necessitating stable internal fixation of theses fractures. We present an atypical case of coronal plane talus fracture in which fracture line extends from posterior aspect of lateral talar process into the body medially and anteriorly (Fig.1) which does not fit into any classification. Two separate mini approaches were used to address the fracture.
Patient Information
A28 year old male presented with pain and swelling in the left ankle following fall from a tree. He had taken first aid elsewhere and presented on the same day to our hospital. There was no history of comorbidities.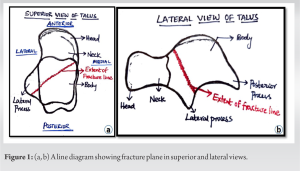
Clinical findings
His vitals were stable. Tense diffuse swelling around ankle was present. Tenderness was present over the lateral malleolus and over the heel. Attempted ankle movements were painful. There are no distal neurovascular deficits. The ankle was immobilized in below-knee plaster splint and radiographs were taken after stabilizing the patient. X-ray showed lateral talar process fracture with probable fracture line extending into body (Fig.2). CT scan revealed coronal plane talus fracture in which fracture line was found extending from posterior aspect of lateral talar process into the body medially and anteriorly (Fig.3a,b,c) and 3D images (3d, 3e). This atypical fracture does not fit into any classification but close to Martin and Weber’s classification [4] type-2.
CT scan revealed coronal plane talus fracture in which fracture line was found extending from posterior aspect of lateral talar process into the body medially and anteriorly (Fig.3a,b,c) and 3D images (3d, 3e). This atypical fracture does not fit into any classification but close to Martin and Weber’s classification [4] type-2.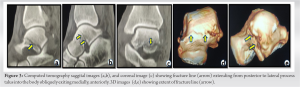
Treatment
Surgery was deferred for few days in view of swelling. The goals of surgical management are anatomic reduction of talus fractures and maintaining subtalar joint congruency. Minimal residual displacement or joint incongruency can adversely affect subtalar joint mechanics.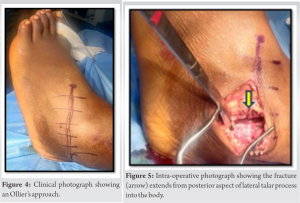 Ollier’s approach (Fig. 4) was used to reduce the fracture (Fig. 5) using clamps (Fig. 6a) and temporarily held in reduction using K-wires (Fig. 6b).
Ollier’s approach (Fig. 4) was used to reduce the fracture (Fig. 5) using clamps (Fig. 6a) and temporarily held in reduction using K-wires (Fig. 6b).  Fracture was stabilized using two Herbert screws. Using a separate mini incision from the anteromedial foot (Fig. 7), a partially threaded. 4-mm cannulated cancellous screw was inserted from head into the body. The screws head was countersunk.
Fracture was stabilized using two Herbert screws. Using a separate mini incision from the anteromedial foot (Fig. 7), a partially threaded. 4-mm cannulated cancellous screw was inserted from head into the body. The screws head was countersunk.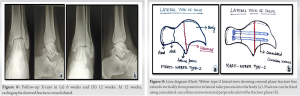
Follow-up and outcome
Post-operatively ankle was immobilized in neutral alignment with below-knee plaster splint. Later changed to a cast after suture removal and once wound healed. The patient was followed up at 6 and 12 weeks (Fig. 8a,b). At 6weeks, cast was removed and partial weight bearing was allowed. At 3months, full weight bearing started once and radiographs showed union at fracture site. Our patient has full range of ankle movements and ambulant pain free. Long-term follow-up is needed to assess the late complications such as avascular necrosis, malunion, and joint stiffness due to post-traumatic arthritis. Implant removal can be considered if there is persistence of pain limiting ankle movements or after 2years once, fracture united.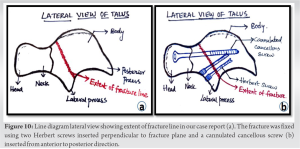
Talar fractures are uncommon injuries constituting 0.1–0.85% of all fractures [1]. Talus is the main link between the ankle and subtalar joints. Untreated talar fractures result in limitation of ankle and subtalar joint movements and result in severe disability [5]. A clear demarcation of talar neck and body fracture makes the difference in management and prognosis Inokuchi et al.[6]. The outcome of talar fractures can be predicted based on vascular supply [7]. Risk of avascular necrosis is highest in body fractures. Sneppen et al classified talar body fractures [8] in which injury happen due to axial compression caused by force transmitted from talus along body into the ankle joint. There are several case reports of talus body fractures along with associated fractures. The follow-up after treatment is shown to be good functional outcome. Shah et al.[9], Kaiashlaxmandevalia et al.[10],Alif Mechhat et al.[11]. We present an atypical talus fracture which does not fit into any classification but close to Marti and Weber’s classification [4] type-2. In Marti and Weber type-2, coronal plane fracture line extends vertically from posterior to lateral talar process into the body and exiting medially (Fig. 9a). The fracture can be stabilized with screw inserted in anterior to posterior direction (Fig. 9b) as the fracture plane is in the straight mediolateral direction. In our case fracture line was extending from posterior aspect of lateral talar process into the body medially and anteriorly creating an oblique fracture in coronal plane (Fig. 10a) which is rarely reported in the literature. Due to obliquity of fracture line, our case required two approaches to obtain adequate fixation. The goals of surgical management are to restore ankle and subtalar joint biomechanics, preventing post-traumatic stiffness. Here in our case conventional method of talar body fracture fixation will not address the fracture extending from posterior aspect of lateral talar process obliquely into the body. Hence the fracture was approached through two separate incisions. Ollier’s approach was used to reduce the fracture and through the same incision, two Herbert screws were inserted perpendicular to the fracture plane. Through mini-open dorsomedial incision ,a 4-mm cannulated cancellous screw was inserted from head into the body (Fig. 10b). Non-weight bearing was advised till 6 weeks with below-knee cast. Once radiographic union was achieved at 3months, full weight bearing ambulation was started. In our case, early union is achieved as deltoid branches of posterior tibial artery were preserved and it plays an important role in healing.
Anatomic and stable reduction plays an important role in achieving good functional outcome Reported our case has a good functional outcome as it was closed and underwent early operative reduction with early signs of vascularization.
Talar fractures extending from posterior aspect of lateral process into the body medially and anteriorly are relatively rare injuries. Accurate diagnosis and timely intervention by open reduction and internal fixation to restore ankle and subtalar joint mechanics allow early rehabilitation and minimize post-traumatic arthritis.
References
- 1.Fortin PT, Balazsy JE. Talus fractures: evaluation and treatment. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2001 Mar 1;9(2):114-27. [Google Scholar]
- 2.Higgins TF, Baumgaertner MR. Diagnosis and treatment of fractures of the talus: a comprehensive review of the literature. Foot & ankle international. 1999 Sep;20(9):595-605. [Google Scholar]
- 3.Sakaki MH, Saito GH, Oliveira RG, Ortiz RT, Silva JD, Fernandes TD, Santos AL. Epidemiological study on talus fractures. Revistabrasileira de ortopedia. 2014 Jul;49:334-9. [Google Scholar]
- 4.Marti R . Talus and calcaneus fractures. In: Weber BG, Brunner C, Freuler F. Fracture treatment in children and adolescents. 1974. [Google Scholar]
- 5.Huang CK, Kitaoka HB, An KN, Chao EY. Biomechanical evaluation of longitudinal arch stability. Foot & Ankle. 1993;14(6):353-7. [Google Scholar]
- 6.Inokuchi S, Ogawa K, Usami N. Classification of fractures of the talus: clear differentiation between neck and body fractures. Foot & ankle international. 1996 Dec;17(12):748-50. [Google Scholar]
- 7.Mulfinger GL, Trueta J. The blood supply of the talus. The Journal of bone and joint surgery.British volume. 1970 Feb;52(1):160-7. [Google Scholar]
- 8.Sneppen O, Christensen SB, Krogsøe O, Lorentzen J. Fracture of the body of the talus. Acta Orthopaedica Scandinavica 1977 Jan 1;48(3):317-24. [Google Scholar]
- 9.Shah K, Hakmi A. Unusual ankle injury—a case report. The Foot. 2004 Sep;14(3):169-72. [Google Scholar]
- 10.Devalia KL, Ismaiel AH, Joseph G, Jesry MG. Fourteen years follow up of an unclassified talar body fracture with review of literature. Foot and ankle surgery. 2006 Jan 1;12(2):85-8. [Google Scholar]
- 11.Mechchat A, Bensaad S, Shimi M, Elibrahimi A, Elmrini A. Unusual ankle fracture: a case report and literature review. journal of clinical orthopaedics and trauma. 2014 Jun 1;5(2):103-6. [Google Scholar]





