
To lessen the surgical insult on the growing skeleton of children with early-onset scoliosis, we require considerable research to develop efficient surgical and anesthetic techniques and better implant constructs.
Dr. Ankit Rai, Department of Orthopedics Surgery, PGIMER, Chandigarh, India. E-mail: ankitrai.doctor@gmail.com
Introduction: Growing rod construct is one of the most widely acknowledged treatment modalities for early-onset scoliosis around the world, but it is not without complications. Throughout the course of treatment, numerous planned and inadvertent surgical interventions are required, which increase the complexity of the treatment. We share our experience with case examples along with extensive literature search and review to get an insight and document the complications with growing rod treatment.
Case Report: These cases underwent surgery with dual growing rod for thoracolumbar idiopathic scoliosis in the view of failed conservative treatment and progressive deformity. Superficial infection is in one case and recurrence of deformity was a common finding though correction of deformity and final fusion was achieved in the cases. Breakage of screws, autofusion of the spanned segments, and profuse bony growths over the implants are common finding to get. Fibrosis and scar tissue from the previous surgeries result in difficulty in the exposure and performing corrective osteotomy.
Conclusion: Growing rod surgery has high complication rates. Repeated surgical and anesthesia exposure pose a great risk to the body and immature skeleton of the young patient. Previous studies have put forth many possible course of action to lower down the complication rates but have met with variable results. A better implant design and surgical efficacy are needed to cut down the number of complications and surgical interventions in growing rod surgeries.
Keywords: Early-onset scoliosis, dual growing rod, growth sparing surgery.
Regardless of the cause, early-onset scoliosis is first identified in children under the age of 10 and is associated with severe morbidity and mortality if overlooked [1]. By the age of 10, the thoracic cage has significantly grown, and the cardiovascular system has significantly developed. The early-onset scoliosis results in stunted growth of the dorsal spine and thoracic cage that culminates into downswing of the cardiopulmonary function [2]. In this age group, spinal fusion corrects the deformity but at the expense of compromising thoracic height. This increases the complexity of managing early-onset scoliosis. Growth sparing single rod surgery was first described by Harington and then modified by Moe et al. [3, 4]. Akbarnia et al. recommended use of growing dual rods with proximal and distal anchorage. This procedure avoided the spinal fusion to allow growth of thoracic spine and cage with satisfactory curve correction. The growing rod surgery has met with lot of success but not without complications. Previous studies have reported the complication rate in growing rod surgery ranging from 20% to 48% and that too rising with each surgical intervention given to the patient. Wound-related complications, implant failure, and loss of alignment increase the number of unplanned surgeries in this subset of patients [5]. The ultimate spinal fusion is considered end of growing rod treatment, but recent studies have found that it is not imperative in all cases and associated with increased morbidity [6]. We are reviewing our experience at tertiary care center in such cases.
Case 1
A 4-year-old boy presented with infantile idiopathic scoliosis with right-sided thoracolumbar curve. There were no other associated sign or symptoms. There was no sensory or motor deficit. Standing upright and bending radiographs were done to calculate curve magnitude which was 50°. There was no structural deformity in the spine. Surgical intervention was planned in view of high Cobb angle and progressive deformity. The patient received his index surgery in the form of dual growing rods with deformity correction. Four proximal and distal anchorages were connected with two separate rods to accommodate spinal growth. Post-operative period was uneventful and the patient was mobilized with brace. The patient received four planned surgical procedures during the ensuing period of follow-ups for rod lengthening to accommodate thoracic and lumbar spine growth. At the final follow-up, it was observed that growing rod has hampered the spinal growth and curve progression was also noted. Implant removal was planned. During the surgery, we discerned significant bone formation over the implant and autofusion of some spinal segments (Fig. 1). There were also broken screws which were not radiologically evident. These unforeseen complications lengthened the surgery time and blood loss during the surgery. The patient was advised thoraco-lumbo-sacral orthosis post-operatively and explained for need of spinal fusion surgery, when needed.
Case 2
A 7-years-old female presented with thoracolumbar scoliosis with progressive deformity. The patient was having back pain at presentation. On detailed clinical examination, nothing was found stipulating syndromic or neuromuscular nature of the scoliosis. Neurological examination was unremarkable. Radiological investigations were carried out, which included standing upright and lateral bending radiographs and MRI. A thoracolumbar scoliotic curve of 64° was noted. It was a structural deformity. The surgery with dual growing rods was planned with four proximal and four distal anchorages connected with rods. Proximal and distal anchors were then connected with two separate rods for lengthening. Total five lengthening procedures were performed. The patient acquired chest infection, which lengthened her hospital stay during her hospital admission for lengthening the growing rod for the second time. She developed superficial infection too which was treated with antibiotics. Over the course of treatment, we noted recurrence of the deformity (Fig. 2), which was corrected at the time of final fusion surgery with corrective osteotomy. The patient remained neurologically intact during entire course of treatment. The final fusion surgery was complicated by the extensive scarring, ossification around instrumentation, and autofusion of the segments.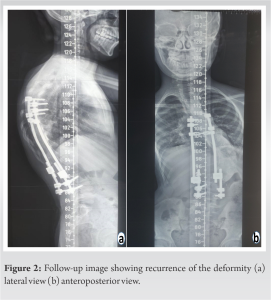
The growing rod surgery is having high complication rates of around 50% and it increases with each surgical procedure (Table 1). 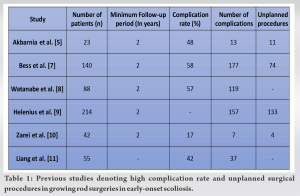 Complications can be related to implant, wound, or alignment [7]. In their multicenter study, Watanabe et al. reported complications in 50 patients (57%) out of 88 following growing rod surgery, with an average follow-up of 3.9 years. High thoracic Cobb angles, thoracic kyphosis, and more subsequent surgeries for rod lengthening were all identified as risk factors for complications in the growing rod surgery [8]. In a study of 23 patients who underwent growing rod surgery and had at least 2 years of follow-up, Akbarnia et al. found that 11 patients (48%) had 19 complications. Deep and superficial infections, implant failure, and alignment failure were the major complications, necessitating 11 unscheduled surgeries throughout treatment and following fusion [5]. Helenius et al. reviewed multicentric database with 107 children with moderate and severe scoliosis in each group. They saw 2.6 complications per patient in severe group and 1.9 complications per patient in moderate group. They saw complications related to anchor failure, longitudinal failure, neurological, and pulmonary complications. The complication rate was more in severe deformity group [9]. In 42 patients with a mean age of 4.8 years who underwent follow-up for a median of 34 months, Zarei et al. reported a 17% complication rate, with infections and proximal junctional kyphosis being the most common complications [10]. At an average follow-up of 5 years, Bess et al. reported complications in 58% of patients who underwent growing rod surgery. He suggested taking preventative measures to reduce complications, such as using dual rods rather than single rods, limiting the number of subsequent procedures for rod lengthening, and placing rods submuscularly [7]. Liang et al. analyzed 55 consecutive patients of early-onset scoliosis with dual growing rod surgery for risk factors of post-operative complications. They concluded that post-operative complications after growing rod surgery are likely multifactorial and associated with curve magnitude and duration between lengthening procedures [11]. Fusion after completion of treatment is also challenging. Autofusion of spanned segments along with extensive scarring from the previous multiple surgeries is among the prominent reasons for high complication rate following fusion surgeries. Cahill et al. retrospectively reviewed 9 skeletally immature children and noted autofusion in 89% of cases with average Cobb angle correction of 44% at final fusion. On an average, 7 osteotomies were needed before final fusion due to unintended autofusion. They concluded that growing rod treatment adversely affects the skeletally immature skeleton and leads to unintended autofusion which mandates osteotomies before ultimate fusion [12]. This increases the surgical duration and blood loss during the procedure. Jain et al. found no significant difference in curve magnitude and truncal heights in final fusion and retention of implant groups. He proposed that most of the spinal segments get ankylosed over the treatment course, so implant can be retained if correction and balance are acceptable with completed spinal growth [6]. Autofusion and stabilization are other proposed treatment end points but Kocyigit et al. [13] in their study of 10 patients noted clinically important worsening of curve magnitude in 9 patients after implant removal. Multiple exposures to anesthetic agents in young patients are another risk factor that adds to the morbidity. Goldstein MJ in a single-center review of 16 patients quantified the anesthesia exposure in the growing rod treatment. They stated that revisions and final fusion added most to the anesthesia exposure and 45% of total anesthesia exposure are because of associated care procedures. They highlighted the need of efficient measures to minimize the anesthesia exposure and duplication without compromising surgical goals [14].
Complications can be related to implant, wound, or alignment [7]. In their multicenter study, Watanabe et al. reported complications in 50 patients (57%) out of 88 following growing rod surgery, with an average follow-up of 3.9 years. High thoracic Cobb angles, thoracic kyphosis, and more subsequent surgeries for rod lengthening were all identified as risk factors for complications in the growing rod surgery [8]. In a study of 23 patients who underwent growing rod surgery and had at least 2 years of follow-up, Akbarnia et al. found that 11 patients (48%) had 19 complications. Deep and superficial infections, implant failure, and alignment failure were the major complications, necessitating 11 unscheduled surgeries throughout treatment and following fusion [5]. Helenius et al. reviewed multicentric database with 107 children with moderate and severe scoliosis in each group. They saw 2.6 complications per patient in severe group and 1.9 complications per patient in moderate group. They saw complications related to anchor failure, longitudinal failure, neurological, and pulmonary complications. The complication rate was more in severe deformity group [9]. In 42 patients with a mean age of 4.8 years who underwent follow-up for a median of 34 months, Zarei et al. reported a 17% complication rate, with infections and proximal junctional kyphosis being the most common complications [10]. At an average follow-up of 5 years, Bess et al. reported complications in 58% of patients who underwent growing rod surgery. He suggested taking preventative measures to reduce complications, such as using dual rods rather than single rods, limiting the number of subsequent procedures for rod lengthening, and placing rods submuscularly [7]. Liang et al. analyzed 55 consecutive patients of early-onset scoliosis with dual growing rod surgery for risk factors of post-operative complications. They concluded that post-operative complications after growing rod surgery are likely multifactorial and associated with curve magnitude and duration between lengthening procedures [11]. Fusion after completion of treatment is also challenging. Autofusion of spanned segments along with extensive scarring from the previous multiple surgeries is among the prominent reasons for high complication rate following fusion surgeries. Cahill et al. retrospectively reviewed 9 skeletally immature children and noted autofusion in 89% of cases with average Cobb angle correction of 44% at final fusion. On an average, 7 osteotomies were needed before final fusion due to unintended autofusion. They concluded that growing rod treatment adversely affects the skeletally immature skeleton and leads to unintended autofusion which mandates osteotomies before ultimate fusion [12]. This increases the surgical duration and blood loss during the procedure. Jain et al. found no significant difference in curve magnitude and truncal heights in final fusion and retention of implant groups. He proposed that most of the spinal segments get ankylosed over the treatment course, so implant can be retained if correction and balance are acceptable with completed spinal growth [6]. Autofusion and stabilization are other proposed treatment end points but Kocyigit et al. [13] in their study of 10 patients noted clinically important worsening of curve magnitude in 9 patients after implant removal. Multiple exposures to anesthetic agents in young patients are another risk factor that adds to the morbidity. Goldstein MJ in a single-center review of 16 patients quantified the anesthesia exposure in the growing rod treatment. They stated that revisions and final fusion added most to the anesthesia exposure and 45% of total anesthesia exposure are because of associated care procedures. They highlighted the need of efficient measures to minimize the anesthesia exposure and duplication without compromising surgical goals [14].
Growing rod surgeries have revolutionized the treatment of early-onset scoliosis but not without its implications and complications. Most of the complications are implant related and that too from proximal anchorage failure. Infections, wound scarring, malalignment, and autofusion further affect the course and outcome of fusion surgery. High complication rate, multiple planned and unplanned surgical procedures, and repeated exposure to anesthetic agents during anesthesia have their adverse effects on the young patients and their immature skeleton. We as authors feel that further research for better implants and surgical efficiency is the need of hour to cut down the number of uncalled surgical procedures and complication rate.
Growing rod surgery despite being widely used worldwide is associated with high complication rates. We need more efficient surgical techniques and implants for lowering number of surgical procedures along with complication rate.
References
- 1.Williams BA, Matsumoto H, McCalla DJ, Akbarnia BA, Blakemore LC, Betz RR, et al. Development and initial validation of the classification of early-onset scoliosis (C-EOS). J Bone Joint Surg Am 2014;96:1359-67. [Google Scholar]
- 2.Canavese F, Dimeglio A. Normal and abnormal spine and thoracic cage development. World J Orthop 2013;4:167-74. [Google Scholar]
- 3.Harrington PR. Treatment of scoliosis. Correction and internal fixation by spine instrumentation. J Bone Joint Surg Am 1962;44-A:591-610. [Google Scholar]
- 4.Moe JH, Kharrat K, Winter RB, Cummine JL. Harrington instrumentation without fusion plus external orthotic support for the treatment of difficult curvature problems in young children. Clin Orthop Relat Res 1984;185:35-45. [Google Scholar]
- 5.Akbarnia BA, Marks DS, Boachie-Adjei O, Thompson AG, Asher MA. Dual growing rod technique for the treatment of progressive early-onset scoliosis: A multicenter study. Spine (Phila Pa 1976) 2005;30:S46-57. [Google Scholar]
- 6.Jain A, Sponseller PD, Flynn JM, Shah SA, Thompson GH, Emans JB, et al. Avoidance of "Final" surgical fusion after growing-rod treatment for early-onset scoliosis. J Bone Joint Surg Am 2016;98:1073-8. [Google Scholar]
- 7.Bess S, Akbarnia BA, Thompson GH, Sponseller PD, Shah SA, El Sebaie H, et al. Complications of growing-rod treatment for early-onset scoliosis: Analysis of one hundred and forty patients. J Bone Joint Surg Am 2010;92:2533-43. [Google Scholar]
- 8.Watanabe K, Uno K, Suzuki T, Kawakami N, Tsuji T, Yanagida H, et al. Risk factors for complications associated with growing-rod surgery for early-onset scoliosis. Spine (Phila Pa 1976) 2013;38:E464-8. [Google Scholar]
- 9.Helenius IJ, Oksanen HM, McClung A, Pawelek JB, Yazici M, Sponseller PD, et al. Outcomes of growing rod surgery for severe compared with moderate early-onset scoliosis: A matched comparative study. Bone Joint J 2018;100-B:772-9. [Google Scholar]
- 10.Zarei M, Tavakoli M, Ghadimi E, Moharrami A, Nili A, Vafaei A, et al. Complications of dual growing rod with all-pedicle screw instrumentation in the treatment of early-onset scoliosis. J Orthop Surg Res 2021;16:112. [Google Scholar]
- 11.Liang J, Li S, Xu D, Zhuang Q, Ren Z, Chen X, et al. Risk factors for predicting complications associated with growing rod surgery for early-onset scoliosis. Clin Neurol Neurosurg 2015;136:15-9. [Google Scholar]
- 12.Cahill PJ, Marvil S, Cuddihy L, Schutt C, Idema J, Clements DH, et al. Autofusion in the immature spine treated with growing rods. Spine (Phila Pa 1976) 2010;35:E1199-203. [Google Scholar]
- 13.Kocyigit IA, Olgun ZD, Demirkiran HG, Ayvaz M, Yazici M. Graduation protocol after growing-rod treatment: Removal of implants without new instrumentation is not a realistic approach. J Bone Joint Surg Am 2017;99:1554-64. [Google Scholar]
- 14.Goldstein MJ, Kabirian N, Pawelek JB, Arandi NR, Mundis GM Jr., Yaszay B, et al. Quantifying anesthesia exposure in growing rod treatment for early onset scoliosis. J Pediatr Orthop 2017;37:e563-6. [Google Scholar]





