
Gouty tophi can abnormally occur on cruciate ligaments of knee without any signs of inflammatory arthritis and could be misdiagnosed with various knee pathologies.
Dr. Lakshmana Reddy Satti, Department of Orthopaedics and Traumatology, Siddhartha hospital, Kakinada, East Godavari, Andhra Pradesh, India. E-mail: slakshmanareddy@gmail.com
Abstract
Introduction: Gouty tophi generally develop around 10 years after the first attack of gout in untreated patients and are commonly found around feet, hands, and elbows. However, tophi can also occur as first sign of disorder. Tophaceous gout presenting in young at the posterior cruciate ligament (PCL) is extremely rare and difficult to diagnose because of its atypical presentation and no hallmark features in magnetic resonance imaging (MRI).
Case Report: Here, we report a 25-year-old man manual worker with no prior history of gout has presented with left knee pain and locking episodes for 3 weeks, X-ray shows no abnormality, on advanced imaging with MRI, a well-defined cyst noted adjacent to PCL toward lateral aspect. During arthroscopy, a cyst was seen between anterior cruciate ligament and PCL with the extrusion of chalky paste-like material on puncturing the cyst. The tophus was biopsied and excised arthroscopically with excellent outcome.
Conclusion: This case report demonstrates that gout does not only always cause severe joint pain from inflammatory arthritis, but can also cause mechanical pain and locking of joint atypically presenting as intra-articular tophi. Hence, gout should also be considered in differential diagnosis of intra-articular cyst. Arthroscopic removal and continuous urate-lowering therapy provide excellent outcomes for such atypical presentations.
Keywords: Gout, intra-articular tophi, posterior cruciate ligament cyst, case report.
Gout is the most prevalent form of inflammatory arthritis, affecting middle-aged men. It is characterized by the deposition of monosodium urate (MSU) crystals in and around joints and other tissues [1]. Clinical manifestations can present as recurrent acute attacks of severe pain, or chronic inflammation affecting peripheral, small and large joints with tophaceous intra- or extra-articular deposits [2]. However, it could also present atypically as intra-articular cyst without any history of inflammatory arthritis. Such presentations are very challenging to surgeons due to broad differential diagnosis [3]. Using conventional imaging such as magnetic resonance imaging (MRI), it is difficult to differentiate between these pathologies as they lack specific features. Herein, we report a case of posterior cruciate ligament (PCL) cyst which finally got diagnosed as gouty tophi mimicking as PCL cyst.
A 25-year-old male, formerly a manual worker, presented with pain in the posterior aspect of left knee and occasional locking episodes and stiffness for 3 weeks with no history of trauma. On local examination, tenderness present at posterior aspect of knee without any effusion and restricted terminal flexion, there was no ligament laxity, pain aggravated on work, and relieved on taking analgesics, there were no constitutional symptoms. X-ray was normal, the patient was not responding to conservative therapy; hence, MRI was advised.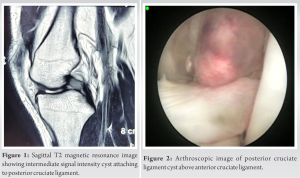 MRI revealed a well-defined T2/PDW intermediate signal intensity cyst of size 10.4 × 9.3 × 8.4 mm noted adjacent to upper third of PCL toward lateral aspect between anterior cruciate ligament [ACL] and PCL with normal signal intensity of PCL and the rest of the joint appearing normal, likely PCL ganglion cyst (Fig. 1), surgery was scheduled with arthroscopy and excisional biopsy of cyst, during arthroscopy a cyst was seen attached to PCL (Fig. 2) with the rest of the joint appearing normal.
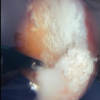
MRI revealed a well-defined T2/PDW intermediate signal intensity cyst of size 10.4 × 9.3 × 8.4 mm noted adjacent to upper third of PCL toward lateral aspect between anterior cruciate ligament [ACL] and PCL with normal signal intensity of PCL and the rest of the joint appearing normal, likely PCL ganglion cyst (Fig. 1), surgery was scheduled with arthroscopy and excisional biopsy of cyst, during arthroscopy a cyst was seen attached to PCL (Fig. 2) with the rest of the joint appearing normal.  On puncturing the cyst with 18G needle, white chalky paste-like calcified tissue extruded out (Fig. 3), the cyst was resected and sent for histopathology and the rest of the tissue debrided without injuring PCL (Fig. 4).
On puncturing the cyst with 18G needle, white chalky paste-like calcified tissue extruded out (Fig. 3), the cyst was resected and sent for histopathology and the rest of the tissue debrided without injuring PCL (Fig. 4). 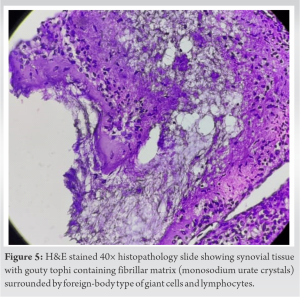 histopathological analysis revealed inflammatory cell collections and tophi composed of gout crystals and giant cells features suggestive of gouty arthritis (Fig. 5). Synovial lavage fluid showed elevated uric acid and needle-shaped MSU crystals. Postoperatively, serum uric acid levels were 9.4 mg/dL. The patient had drastic relief of pain postoperatively and was kept on febuxostat and advised dietary modifications. Follow-up after 2 months revealed good range of motion and complete cessation of pain and serum uric acid 7.2 mg/dL. The patient was followed till 18 months during which there was no recurrence of symptoms.
histopathological analysis revealed inflammatory cell collections and tophi composed of gout crystals and giant cells features suggestive of gouty arthritis (Fig. 5). Synovial lavage fluid showed elevated uric acid and needle-shaped MSU crystals. Postoperatively, serum uric acid levels were 9.4 mg/dL. The patient had drastic relief of pain postoperatively and was kept on febuxostat and advised dietary modifications. Follow-up after 2 months revealed good range of motion and complete cessation of pain and serum uric acid 7.2 mg/dL. The patient was followed till 18 months during which there was no recurrence of symptoms.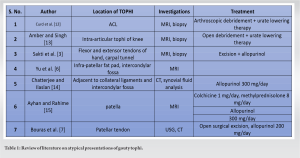
Tophi are the pathognomonic lesions of gout appearing in subcutaneous tissue with a predilection for peripheral joints of lower extremities [4,5]. Tophi occur as late clinical presentation of gout. However, tophi can occur atypically in and around knee as tophi of patellar tendon, within synovium, patella, intercondylar notch, and cruciate ligaments. Such acute presentation in patients without prior inflammatory arthritis may mimic neoplasm [6,7]. They may also occur at precarious positions which can lead to fatal problems, such as spinal cord, carpal tunnel, and heart valves [8,9]. Gouty tophus presenting as acute intra-articular cyst is very difficult to differentiate from other intra-articular pathologies through conventional MRI. Common pathologies of intra-articular mass include ganglion cysts, pigmented villonodular synovitis, meniscal cysts, synovial cysts, synovial chondromatosis, Lipoma arborescens, synovial sarcoma, pannus, and gouty tophi [10]. Most of these lesions including gout show intermediate signal intensity on T1-weighted images of MRI. MR features of gouty tophi have not been studied in detail, and MRI appearance of tophi is non-specific [11]. On review of literature, few authors have reported atypical presentation of gouty tophi and their respective modes of management, most of these groups had difficulty in diagnosing tophi preoperatively (Table 1).
Gout could present atypically as intra-articular cyst without any prior symptoms and elevated serum uric acid levels; hence, it should also be considered in differential diagnosis of intra-articular cyst. Treatment of PCL cyst is uniform throughout literature, some groups did arthroscopic debridement till base and some groups excised through open arthrotomy; here we performed an arthroscopic debridement and biopsy of specimen revealed it as gout. To accurately diagnose a gouty tophus, a dual approach using MRI and histological examination is necessary to differentiate it from other intra-articular cysts. No such case has been reported in literature till now, and findings of this report add to the growing knowledge base surrounding atypical presentations of tophi and their management.
Intra articular cysts in knee are difficult to diagnose, gouty tophi could atypically present in cruciate ligaments of knee without prior signs of inflammation and could be misdiagnoses with various knee pathologies, biopsy is the only diagnostic modality for such presentation; hence gout should also be considered in differential diagnosis of intra-articular cysts in knee.
References
- 1.Chen LX, Schumacher HR. Gout: Can we create an evidence-based systematic approach to diagnosis and management? Best Pract Res Clin Rheumatol 2006;20:673-84. [Google Scholar | PubMed]
- 2.Singh JA, Reddy SG, Kundukulam J. Risk factors for gout and prevention: A systematic review of the literature. Curr Opin Rheumatol 2011;23:192-202. [Google Scholar | PubMed]
- 3.Sakti M, Usman MA, Lee J, Benjamin M, Maulidiah Q. Atypical musculoskeletal manifestations of gout in hyperuricemia patients. Open Access Rheumatol 2019;11:47-52. [Google Scholar | PubMed]
- 4.Becker MA, Levinson DJ. Clinical gout and the pathogenesis of hyperuricemia. In: Koopman WJ, editor. Arthritis and Allied Conditions. 13th ed. Pennsylvania: Williams and Wilkins; 1997. p. 2041-71. [Google Scholar | PubMed]
- 5.Kelley WN, Wortmann RL. Gout and hyperuricemia. In: Kelley WN, Harris ED, Ruddy S, Sledge CB, editor. Textbook of Rheumatology. 5th ed. Philadelphia, PA: WB Saunders; 1997. p. 1313-51. [Google Scholar | PubMed]
- 6.Yu KH, Lien LC, Ho HH. Limited knee joint range of motion due to invisible gouty tophi. Rheumatology (Oxford) 2004;43:191-4. [Google Scholar | PubMed]
- 7.Bouras T, Gandhi M, Barnett A. Diagnosis and treatment of patellar tendon gouty tophus: A case report. Surg J (N Y) 2019;5:e46-9. [Google Scholar | PubMed]
- 8.Popovich T, Carpenter JS, Rai AT, Carson LV, Williams HJ, Marano GD. Spinal cord compression by tophaceous gout with fluorodeoxyglucose-positron-emission tomographic/MR fusion imaging. AJNR Am J Neuroradiol 2006;27:1201-3. [Google Scholar | PubMed]
- 9.Iacobellis G, Iacobellis G. A rare and asymptomatic case of mitral valve tophus associated with severe gouty tophaceous arthritis. J Endocrinol Invest 2004;27:965-6. [Google Scholar | PubMed]
- 10.Andrea AJ, Stensby JD, Rosas S, Emory CL. Diagnostic imaging and management of common intra-articular and peri-articular soft tissue tumors and tumorlike conditions of the knee. J Knee Surg 2019;32:322-30. [Google Scholar | PubMed]
- 11.YU JS, Chung C, Recht M, Dailiana T, Jurdi R. MR imaging of tophaceous gout. Am J Roentgenol 1997;168:523-7. [Google Scholar | PubMed]
- 12.Curd ED, Ravichandiran K, Abouali J. Gouty tophus presenting as an anterior cruciate ligament mass in the knee: Case report and brief review of relevant literature. Int J Surg Case Rep 2021;82:105920. [Google Scholar | PubMed]
- 13.Amber H, Singh VA. Gouty tophi mimicking synovial sarcoma of the knee joint. Turk J Rheumatol 2012;27:208-11. [Google Scholar | PubMed]
- 14.Chatterjee S, Ilaslan H. Painful knee locking caused by gouty tophi successfully treated with allopurinol. Nat Clin Pract Rheumatol 2008;4:675-9. [Google Scholar | PubMed]
- 15.Ayhan AŞ, Rahime İN. A rare cause of knee pain in gout patients: Tophi of patella. Arch Rheumatol 2015;30:71-4. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report
February 1, 2026 Gouty Arthritis Versus Chondrocalcinosis in a Stiff Knee, A Diagnostic Dilemma – A Case Report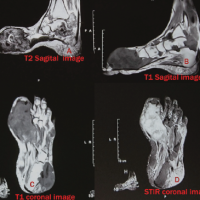 April 1, 2025 Gouty Arthritis with Massive Tophaceous Deposits Involving Bilateral Metatarsophalangeal Joints, Surgical Treatment with Excision and Reconstruction – A Case Report
April 1, 2025 Gouty Arthritis with Massive Tophaceous Deposits Involving Bilateral Metatarsophalangeal Joints, Surgical Treatment with Excision and Reconstruction – A Case Report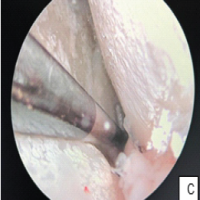 March 1, 2025 Arthroscopic Treatment of Isolated Tophaceous Gout of the Knee: A Rare Case Report
March 1, 2025 Arthroscopic Treatment of Isolated Tophaceous Gout of the Knee: A Rare Case Report January 10, 2020 A Case of Surgically Intervened Chronic Tophaceous Gout and Review of Literature
January 10, 2020 A Case of Surgically Intervened Chronic Tophaceous Gout and Review of Literature