
Surgical treatment of chronic misdiagnosed lateral instability of the ankle after acute rotational injury, treated with autologous semitendinosus graft posing a good clinical outcome.
Dr. Christina Pechlivani, Department of Orthopedic Surgery and Traumatology - Unit for Sport Injuries, General Hospital of Thessaloniki “Agios Pavlos,” Ethnikis Antistaseos, Thessaloniki, Greece. E-mail: cpechlivani4963@gmail.com
Introduction: One of the most common orthopedic injuries seen in patients at the emergency department is that of the ankle. There are some efficient protocols for their treatment, but more often the clinician is focused in finding and treating possible fractures and disregards ligamentous lesions that lead to instability if they become chronic.
Case Report: A patient that suffered an ankle sprain was improperly handled, developed lateral instability of the ankle, and was treated surgically using an autologous semitendinosus graft. A 42-year-old Caucasian male that after an ankle sprain was examined in various primary health-care centers, four times within 6 months, with persistent symptoms of his left ankle. After all these months, he was eventually diagnosed with post-traumatic lateral instability of the ankle that was resistant to conservative treatment. In stress view X-rays, the talar tilt angle was 21° and the anterior drawer was measured at 13 mm. The patient was treated surgically with reconstruction of the anterior talofibular and the calcaneofibular ligament using an autologous semitendinosus graft from the left knee. The graft was pinned in the anatomical insertion sites of the ligaments with absorbable screws. A post-surgical physiotherapy regimen was ap-plied for 2 months. In the post-surgical dynamic stress view X-rays, the talar tilt angle and the anterior drawer were markedly improved, measured at 3° and 4 mm, respectively. In 11 months post-surgical follow-up, the patient’s American Foot and Ankle Score was 85, from the 60 evaluated before treatment.
Conclusion: The use of guidelines, regular follow-ups, and functional rehabilitation are key factors to treating ankle injuries. The reconstruction of lateral collateral ligament complex with a semitendinosus graft is one of the surgical options for restoring lateral ankle instability.
Keywords: Ankle sprain, autologous semitendinosus graft, lateral instability of the ankle.
Acute ankle injuries are some of the most frequently encountered orthopedic injuries [1] occurring at a rate of 1/10.000 individuals every day [2]. About 85% are associated with lateral ligamentous trauma that can lead to lateral ankle instability [3]. The occurrence of ankle injuries can come up to 45% of the total number of injuries in sports with high prevalence, such as basketball [1]. In general, they are considered “self-healing” with good prognosis and good outcomes following conservative treatment [4], but there are studies that show persistent symptoms for months, even years, after the initial injury [2]. These symptoms may be an indication of ankle instability and they range from mechanical symptoms, transient edema, weakness, stiffness, loss of range of motion, osteochondral lesions, and osteoarthritis [2, 5] that may lead to disability and may affect the quality of life [5]. The percentage of patients that may present with lingering symptoms and/or pathological signs is between 32% and 74% when examined from 6 months up to 7 years after a sprain [5]. Despite their prevalence and relative detrimental consequence in a patient’s life, there is still a staggering lack of effective treatment guidelines [6]. The fact that ankle sprains are easily dismissed by clinicians when no fracture is present is apparent when taking into account that in 77–99% of cases, X-ray is prescribed but only in 9–15%, there is a fracture [7]. Ligamentous abrasions should be brought into focus, as they are way more common than fractures [3].
In this case report, a patient with rotational ankle injury and acute ligamentous trauma was insufficiently treated and he developed lateral ankle instability that was belatedly treated surgically using an autologous semitendinosus graft.
History
Male Caucasian, 42 years old, manual worker had a rotational left ankle injury with varus-internal rotation mechanism of trauma. No symptoms from his lower extremities were recorded before his injury and he reported amateur sport activities during childhood (soccer). After the injury, he immediately consulted a medical practitioner at a primary care center, where a clinical and X-ray evaluation ensued, with no apparent bony defects. Gradually, he recovered and fully resumed the previous level of activity in 3–4 weeks, with no apparent protocol of rehabilitation. In 6 months, the patient was subjected to two additional ankle injuries with the same mechanism of action and no fractures were found with the two additional X-rays. He also consulted thrice a medical practitioner at two different primary care centers. The patient was occasionally using cold compresses and elastic bandages for his ankle but he did not follow a specific rehabilitation plan. Because of his worsening symptoms, the patient turned to our outpatient clinic for a solution.
Signs and symptoms
During his clinical evaluation, the patient complained of pain, especially at the lateral side and after activity, with a sense of instability and unreliability when walking and driving. On palpation, pain was reproduced just inferior and anterior of the lateral malleoli, anterior drawer test, and talar tilt test [8] tested positive. That showcased a rupture of both anterior talofibular and calcaneofibular ligaments [8].
Radiographic evaluation
Static and stress anteroposterior and profile radiographs were performed on both ankles. In the stress radiographs, the talar tilt of the left ankle was measured at 21° in the anterioposterior view (Fig. 1). In addition, anterior sliding of 13 mm was measured in profile view (Fig. 2).  In the magnetic resonance imaging, there was confirmation of the ruptures of anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL).
In the magnetic resonance imaging, there was confirmation of the ruptures of anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL).
Treatment
A program of non-surgical treatment followed our evaluation for 6 weeks that targeted on functional reeducation, biofeedback, and strengthening of dynamic ankle stabilizers. The non-surgical treatment failed, so we turned to anatomical reconstruction of ATFL and CFL with autologous semitendinosus graft as the best treatment for our case [9]. The procedure was performed as described in bibliography [9]. A lateral ankle approach was chosen with a straight incision that carved slightly posteriorly distally (Fig. 3), the soft-tissue was dissected, and complete degeneration of the lateral ligamentous complex of the ankle was found (Fig. 4), that signified no chance of anatomical repair and made the anatomical reconstruction imperative.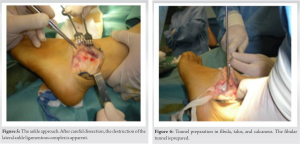 The semitendinosus graft was harvested from the ipsilateral knee (Fig. 5), debridement of the scar tissue was performed, and the positions of fixation in the lateral malleolus, talus, and calcaneus were marked and prepared. The graft was fixated with absorbable screws with the ankle in neutral position and the graft was slightly tightened (Fig. 6, 7, 8).
The semitendinosus graft was harvested from the ipsilateral knee (Fig. 5), debridement of the scar tissue was performed, and the positions of fixation in the lateral malleolus, talus, and calcaneus were marked and prepared. The graft was fixated with absorbable screws with the ankle in neutral position and the graft was slightly tightened (Fig. 6, 7, 8). The intra-operative stability of the ankle was found satisfactory and the surgical wound was closed. A dorsal backslap splint with the ankle in neutral position was placed.
The intra-operative stability of the ankle was found satisfactory and the surgical wound was closed. A dorsal backslap splint with the ankle in neutral position was placed.
Post-operative protocol
The splint was kept for 6 weeks. The sutures were removed at 2 weeks with no wound complications. After the 2nd week, the patient started exercises to improve the range of motion and light partial weight bearing. After the 4th week, a complete program of functional physiotherapy was applied for 2 months and included exercises for range of motion, stability, elasticity, and biofeedback of the ankle. The patient had several follow-up appointments, the last one being 11 months port-operatively. The patient’s American Foot and Ankle Score [10] improved from 60 before surgery to 85, with no complaints about subjective instability when walking on irregular surfaces (sandy or rocky terrain). On post-operative dynamic X-rays of the ankle, the talar tilt decreased from 21° to 3° in the anteroposterior view (Fig. 9) and the anterior translation from 13 mm to 4 mm in the profile view (Fig. 10).
Chronic lateral ankle instability may well be one of the most severe complications of a neglected ankle sprain [3]. About 20% of acute ankle sprains will become chronic instability [11], mainly because of the destruction of mechanoreceptors [12]. Most studies suggest conservative treatment initially, as results are similar compared to surgical treatment and lack the consideration of cost and complications of the second [13]. If the patient shows no or minimal clinical improvement, there is still the option of surgical repair or reconstruction, for which several procedures have been described [14], with 80–95% of their authors reporting good or very good results [15]. The procedures can be categorized to anatomical repairs, non-anatomical reconstructions, and anatomical reconstructions [14], the last of which has been proved to be superior in biomechanical studies [15]. In our patient, this anatomical reconstruction was chosen because of its advantages: The length of the graft was satisfactory, harvest and fixation were easier, the incision was smaller, and no anatomical structures of the ankle or foot were sacrificed as grafts [14]. The early observed good results are corroborated by studies with a longer list of cases that underwent anatomical reconstruction either with a semitendinosus graft [12] or a peroneus brevis graft [15].
To sum up, the treatment of acute ankle injury must follow the appropriate algorithms, as the one described by Polzer et al., according to which clinical evaluation and re-evaluation after 3–5 days when the pain and edema have eased up is the key and following rehabilitation protocol therein can ensure a satisfactory functional result [6]. In the cases that lateral instability sets in and non-surgical treatment has failed, reconstruction of ATFL and CFL with autologous semitendinosus graft can restore stability surgically with good results.
Acute ankle injuries are some of the most common injuries; an orthopedic surgeon will be called to treat in the emergency department, however, they appear to be mistreated in a very high rate. In our case, although the patient repeatedly visited medical practitioners due to clinical symptoms, he continued to be insufficiently treated for up to 6 months. It is of great importance to never forget the possibility of severe ligamentous injury and instability and if so to be appropriately treated.
References
- 1.Trevino SG, Davis P, Hecht PJ. Management of acute and chronic lateral ligament injuries of the ankle. Orthop Clin North Am 1994;25:1-16. [Google Scholar]
- 2.Struijs P, Kerkhoffs G. Ankle sprain. Clin Evid 2006;15:1493-501. [Google Scholar]
- 3.Peters JW, Trevino SG, Renstrom PA. Chronic lateral ankle instability. Foot Ankle 1991;12:182-91. [Google Scholar]
- 4.Groff GD. Ankle sprain. In: Klippel J, Dieppe P, editors. Rheumatology. London: Mosby; 1998. p. 14.10-14.13. [Google Scholar]
- 5.Anandacoomarasamy A, Barnsley L. Long term outcomes of inversion ankle injuries. Br J Sports Med 2005;39:e14. [Google Scholar]
- 6.Polzer H, Kanz KG, Prall WC, Haasters F, Ockert B, Mutschler W, et al. Diagnosis and treatment of acute ankle injuries: Development of an evidence-based algorithm. Orthop Rev (Pavia) 2012;4:e5. [Google Scholar]
- 7.Cameron C, Naylor CD. No impact from active dissemination of the Ottawa Ankle Rules: Further evidence of the need for local implementation of practice guidelines. CMAJ 1999;160:1165-8. [Google Scholar]
- 8.Van Dijk CN, Lim LS, Bossuyt PM, Marti RK. Physical examination is sufficient for the diagnosis of sprained ankles. J Bone Joint Surg Br 1996;78:958-62. [Google Scholar]
- 9.Paterson R, Cohen B, Taylor D, Bourne A, Black J. Reconstruction of the lateral ligaments of the ankle using semi-tendinosis graft. Foot Ankle Int 2000;21:413-9. [Google Scholar]
- 10.Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating sys-tems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 1994;15:349-53. [Google Scholar]
- 11.Berlet G, Anderson RB, Davis W. Chronic lateral ankle instability. Foot Ankle Clin 1999;4:713-28. [Google Scholar]
- 12.Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg 1998;6:368-77. [Google Scholar]
- 13.Tiling T, Bonk A, Hoher J, Klein J. Acute injury to the lateral ligament of the ankle joint in the ath-lete. Chirurg 1994;65:920-33. [Google Scholar]
- 14.Chan KW, Ding BC, Mroczek KJ. Acute and chronic lateral ankle instability in the athlete. Bull NYU Hosp Joint Dis 2011;69:17-26. [Google Scholar]
- 15.Tourné Y, Besse JL, Mabit C; Sofcot. Chronic ankle instability. Which tests to assess the lesions? Which therapeutic options? Orthop Traumatol Surg Res 2010;96:433-46. [Google Scholar]








