
3D printing sequence and principles, advantages, and limitations of 3D printing for custom made endoprosthesis, management of pelvic osteosarcoma?
Dr. Dheeraj Makkar, Department of Orthopaedics, NC Medical College, NC Medical College, Room No. 204 , Panipat, Haryana, India. E-mail: makkardheeraj@gmail.com
Introduction: Osteosarcoma of the pelvis poses challenges in surgical resection due to its anatomical location and extensive nature. This case report focuses on the clinical presentation and therapeutic outcomes of a 20-year-old patient with osteosarcoma of the right iliac bone. The study highlights the efficacy of 3D printing technology in creating customized implants for improved surgical outcomes.
Case Report: The case report presents the clinical presentation, management, and outcomes of a patient with osteosarcoma of the right iliac bone. It emphasizes the impact of surgical resection extent and endoprosthetic reconstruction. The study highlights the advantages of 3D printing technology in creating customized implants that accurately fit the remaining bone. Limb-sparing surgery is advocated for better functional and psychological outcomes compared to amputation. The report also emphasizes the need for further research on alternative composite materials and discusses the limitations of 3D printing technology in orthopedics. The limitations of 3D printing, such as mechanical safety and material restrictions, are discussed, calling for future advancements to improve the reliability and effectiveness of 3D-printed implants in orthopedics.
Conclusion: The present case report provides valuable perspectives into the efficacious management of pelvic osteosarcoma and underscores the distinctive advantages of 3D printing technology in improving surgical results. Limb-sparing surgery demonstrates enhanced functional and psychological outcomes compared to amputation. Utilizing 3D custom-made implants, significantly reduces the likelihood of revision surgeries attributed to implant failure, improves the surgical outcome and precision.
Keywords: Osteosarcoma, pelvis, 3D printing, endoprosthesis, titanium.
Osteosarcoma is a malignant tumor of bone, typically seen in children and adolescents. While the knee is the most commonly affected site, osteosarcoma can manifest in any bone throughout the skeletal system. Roughly 5–10% of osteosarcoma cases arise primarily within the bony pelvis [1]. Owing to their anatomical site, regional spread, and voluminous nature, osteosarcomas that originate in the bony pelvis pose a significant challenge when attempting resection. Patients afflicted by this condition purportedly exhibit an unfavorable prognosis [2]. The purpose of this report is to provide a thorough analysis of the clinical presentation and therapeutic outcomes of a 20-year-old individual diagnosed with osteosarcoma of the iliac bone. Specifically, we examine the impact of the extent of surgical resection and endoprosthetic reconstruction on the patient’s condition. The results of this study offer valuable insights into the effectiveness of 3D printing and its potential for enhancing patient outcomes.
Chief complaints and history of present illness
The patient presented with persistent and worsening pain localized in the right iliac bone area of the pelvic region for 6 months. The pain, described as dull and aching, was aggravated by weight-bearing activities and worsened at night. Physical examination revealed a localized swelling of approximately tennis ball size with an irregular contour, accompanied by reddish discoloration, and dimpling of the overlying skin, indicating potential underlying pathology.
Laboratory findings
The patient’s laboratory test results were unremarkable, except for elevated levels of Alkaline Phosphatase and LDH, which were found to be 3200 U/L and 2200 U/L, respectively.
Imaging
The patient’s pelvic X-ray indicated bone loss with soft-tissue involvement, suggestive of osteosarcoma (Fig. 1).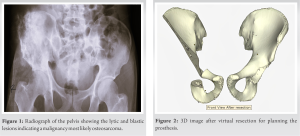 Computed tomography (CT) imaging confirmed osteoblastic lesions with cortical destruction and infiltration of surrounding tissues. Comprehensive CT scans of the chest and abdomen revealed no evidence of metastasis or secondary lesions.
Computed tomography (CT) imaging confirmed osteoblastic lesions with cortical destruction and infiltration of surrounding tissues. Comprehensive CT scans of the chest and abdomen revealed no evidence of metastasis or secondary lesions.
Biopsy
Under the supervision of an experienced surgeon, a surgical biopsy employing a lateral approach was conducted. Histopathological analysis revealed a high-grade osteosarcoma characterized by spindle cells, osteoid production, and positive immunostaining for osteocalcin, confirming the diagnosis.
Treatment
Planning
The treatment strategy involved an internal hemipelvectomy to preserve the patient’s limb, with the aid of a customized endoprosthesis created using 3D printing technology. 3D CT images generated a modified model of the remaining bone structure after digitally removing the osteosarcoma-affected region (Fig. 2).  This model served as the basis for designing an individualized implant made of porous titanium (Fig. 3a, 3b and Fig. 4).
This model served as the basis for designing an individualized implant made of porous titanium (Fig. 3a, 3b and Fig. 4).  The porous structure promotes osseointegration, enhancing implant stability and longevity within the patient’s body.
The porous structure promotes osseointegration, enhancing implant stability and longevity within the patient’s body.
Surgery
Before surgery, the patient underwent neoadjuvant chemotherapy consisting of methotrexate, doxorubicin, cisplatin, and ifosfamide for three cycles to reduce tumor size. The triradiate approach was employed, with the patient positioned supine and a curved incision made over the anterior hip joint (Fig. 5). Dissection exposed the underlying muscles, with the sartorius muscle retracted laterally. The tensor fasciae lata muscle was dissected, creating an interval for access to the joint capsule. Capsulotomy allowed manipulation and visualization of the femoral head and acetabulum during meticulous excision of the affected bone (Fig. 6).  The endoprosthesis was fixed onto the remaining pelvic bone using screws (Fig. 7), followed by closure of the incision using staples.
The endoprosthesis was fixed onto the remaining pelvic bone using screws (Fig. 7), followed by closure of the incision using staples.
Postoperative follow-up
The wound’s healing progress was observed, and after 15 days, the sutures were removed, without any complications. Subsequent follow-up appointments were scheduled at regular intervals during which we performed computed tomography CT scans. These studies consistently revealed no indications of local recurrence or distant metastasis, providing reassurance regarding the patient’s disease status. The patient has remained disease free for the past 2 years and has successfully resumed his normal activities.
The utilization of prosthetic reconstruction after extensive removal of primary osteosarcoma has resulted in a considerably higher rate of revisions, single and multiple, in contrast to biological reconstruction [3]. It was in contrast to our case, in which there were no recurrences over 2 years. Mittermayer et al. reported that long-term outcomes of modular prostheses have shown a need for additional surgeries due to bushing wear, increasing the risk of infection and aseptic loosening, which presents a disadvantage compared to biological reconstructions, such as autografts [4]. The higher revision rate in prosthetic reconstruction for primary osteosarcoma may be due to using non-customized prostheses instead of anatomically tailored implants created with 3D printing technology. While biological reconstruction showed improved revision-free survival, there was no statistical difference. The endoprosthetic reconstruction has less probability of local recurrence or subsequent amputation due to complications, in sharp contrast to the biological reconstruction group. This observation is noteworthy, as it highlights a potential advantage of endoprosthetic reconstruction over biological reconstruction, in terms of postoperative outcomes. The findings of Saab et al. indicate that a considerable percentage of patients (21%) developed osteosarcoma because of prior radiation therapy, with a notable incidence of secondary tumors observed in the pelvic region [5]. In comparison, previous investigations have reported varying proportions of secondary tumors in the pelvic area, ranging from 12.5% to 15.8% [3, 6]. However, our case report differs as the pelvic osteosarcoma was sporadic rather than radiation induced. Previous studies have associated larger tumor size with a poorer prognosis in pelvic and extremity osteosarcoma. Tumor size, measured as the greatest dimension (>15 cm in our case, Fig. 6), did not show significant prognostic value, although the limitation of a single patient and unavailability of tumor volume data should be considered [7]. Personalized 3D-printed implants offer significant advantages compared to allograft prosthetic composite. They provide shorter surgical durations, eliminate the need for allograft carving, simplify implant component fixation through preoperative customization, and improve surgeons’ understanding of procedures. Patient-specific instruments enable precise resection and reconstruction. The ability to manufacture anatomical implants with various shapes and structures, along with enhanced osseointegration due to the porous architecture, contributes to improved long-term performance. However, further research should address potential confounding variables associated with surgical duration. We identified some limitations of 3D printing, including the lack of guaranteed mechanical safety, particularly fatigue strength. Furthermore, the maximum size of the 3D-printed implant is restricted by the metal printer, typically to approximately 20 cm in length [8]. In addition, 3D printing with composite materials presents technical challenges, resulting in the preference for single titanium alloys for implant fabrication. For instance, we used Ti6Al4V is a suitable material for minimizing the stress shield effect and improving biocompatibility, but it exhibits weak wear resistance, which complicates the fabrication of joint implants using a single titanium alloy [9, 10]. The limitations identified in this study highlight the need for continued research and development efforts to address the key concerns related to the mechanical safety of 3D-printed orthopedic implants, expanding the printable size range, and overcoming technical challenges associated with the printing of composite materials. By making advancements in these areas, the potential of 3D printing in orthopedic applications can be significantly enhanced. Therefore, future studies and technological innovations should focus on these aspects to further improve the effectiveness and reliability of 3D-printed implants in orthopedics [9].
Prompt diagnosis and a comprehensive treatment approach involving neoadjuvant and adjuvant chemotherapy along with surgical intervention improve outcomes in pelvic osteosarcoma. Whenever feasible limb-sparing surgery should be pursued as the primary treatment option, as it offers superior functional and psychological results compared to amputation. Implementation of 3D printing technology has emerged as a precise technique that confers various advantages, including reducing surgical duration, facilitating precise resection, and enhancing preoperative planning. Nonetheless, further investigation is warranted to explore alternative composite materials beyond titanium for fabricating custom-made prostheses using this technique.
The pre-operative 3D printing in pelvic surgery offers advantages such as shorter duration and precise resection, but alternative materials require investigation.
References
- 1.Mirabello L, Troisi RJ, Savage SA. Osteosarcoma incidence and survival rates from 1973 to 2004: Data from the Surveillance, Epidemiology, and End Results Program. Cancer 2009;115:1531-43. [Google Scholar]
- 2.Fahey M, Spanier SS, Vander Griend RA. Osteosarcoma of the pelvis. A clinical and histopathological study of twenty-five patients. J Bone Joint Surg Am 1992;74:321-30. [Google Scholar]
- 3.Ham SJ, Kroon HM, Koops HS, Hoekstra HJ. Osteosarcoma of the pelvis--oncological results of 40 patients registered by The Netherlands Committee on Bone Tumours. Eur J Surg Oncol 2000;26:53-60. [Google Scholar]
- 4.Mittermayer F, Krepler P, Dominkus M, Schwameis E, Sluga M, Heinzl H, et al. Long-term followup of uncemented tumor endoprostheses for the lower extremity. Clin Orthop Relat Res 2001;388:167-77. [Google Scholar]
- 5.Saab R, Rao BN, Rodriguez-Galindo C, Billups CA, Fortenberry TN, Daw NC. Osteosarcoma of the pelvis in children and young adults: The St. Jude Children’s Research Hospital experience. Cancer 2005;103:1468-74 [Google Scholar]
- 6.Kawai A, Huvos AG, Meyers PA, Healey JH. Osteosarcoma of the pelvis. Oncologic results of 40 patients. Clin Orthop Relat Res 1998;388:196-207. [Google Scholar]
- 7.Bielack SS, Kempf-Bielack B, Delling G, Exner GU, Flege S, Helmke K, et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-90. [Google Scholar]
- 8.Park JW, Kang HG, Kim JH, Kim HS. New 3-dimensional implant application as an alternative to allograft in limb salvage surgery: A technical note on 10 cases. Acta Orthop 2020;91:489-96. [Google Scholar]
- 9.Ng SL, Das S, Ting YP, Wong RCW, Chanchareonsook N. Benefits and biosafety of use of 3D-printing technology for titanium biomedical implants: A pilot study in the rabbit model. Int J Mol Sci 2021;22:8480. [Google Scholar]
- 10.Murphy SV, De Coppi P, Atala A. Opportunities and challenges of translational 3D bioprinting. Nat Biomed Eng 2020;4:370-80. [Google Scholar]




