
Use of 3D-printed patient-specific femoral jig as an alternative to robotic or navigation total knee arthroplasty in a case of complex primary knee arthroplasty.
Dr. Aravind Sai Sathikumar, Division of Joint Replacement and Sports Medicine, VPS Lakeshore Hospital: Lakeshore Hospital and Research Centre Ltd., Kochi, Kerala, India. E-mail: dr.aravindsai94@gmail.com
Introduction: Patients with Paget’s disease develop abnormal bony anatomy which can result in significantly altered lower limb alignment predisposing them to early secondary osteoarthritis. Due to the severe extra-articular deformity, total knee arthroplasty (TKA) in these patients is challenging. Conventional knee arthroplasty using intramedullary guides is not an option and can lead to erroneous limb alignment postoperatively. Patient-specific instrumentation (PSI) is a simple solution in such complex primary knee arthroplasty.
Case Report: A 70-year-old male patient presented with a severe left femur deformity and left knee pain. He was diagnosed to have monostotic Paget’s disease of the left femur with tricompartmental osteoarthritis of the left knee. After reduction in pathological bone turnover, the patient was planned for a total knee replacement. As a standard intramedullary femoral jig was not applicable due to the femoral deformity, a computed topography-based 3D-printed patient-specific instrument was used. This custom jig was used to define and perform the distal femur cut at 90 degrees to the mechanical axis of the femur in the coronal and sagittal plane. Postoperatively, the patient did well and achieved good function and pain relief.
Conclusion: The use of a 3D-printed PSI for complex primary knee arthroplasty is an excellent option with no additional operative time than a conventional knee arthroplasty. Although a robotic or computer-navigated TKA would be an excellent option in this case, we restored the limb alignment using a cost-effective patient-specific femoral jig. This could be a viable option in centers without navigation or robotic arthroplasty.
Keywords: 3D-printed jigs, total knee arthroplasty, Paget’s disease, femur deformity, patient-specific instrumentation.
Paget’s disease is a common metabolic disorder of the skeletal system caused by deranged bone turnover. Monostotic Paget’s disease may manifest with knee joint pain due to osteoarthritis secondary to long bone deformities like excessive anterolateral bowing of femur [1]. Total knee arthroplasty (TKA) has been an excellent surgical solution for patients with knee osteoarthritis secondary to monostotic femoral Paget’s disease and literature has shown no increased post-operative complications when compared to a standard normal TKA [2, 3]. However, abnormal bony anatomy in the femur does not allow for standard intramedullary instrumentation to be used in such cases as the medullary canals do not accommodate the intramedullary rod and the distal femoral cut cannot be performed as in a normal mechanical TKA [4]. Navigated TKA and robotic TKA do solve this issue but in centers without such facility, other options must be employed. A 3D-printed jig can be considered a viable cost-effective solution. We report a case of primary TKA in a patient with monostotic Paget’s disease with abnormal femoral anatomy using a patient-specific 3D-printed jig.
A 70-year-old male patient presented to our outpatient department with the left knee pain, left thigh pain, and deformity. Clinical examination revealed an excessive biplanar bowing of the femur with a non-correctable varus deformity of the knee. The patient had medial joint line tenderness of the knee and 5° fixed flexion deformity. Further examination revealed the range of movement to be 5–120° with crepitus appreciated throughout the full range. Distal pulses and neurology were found to be normal. Routine standing knee and limb alignment X-rays revealed a severe left femoral bow with a sclerosed thickened femoral cortex and advanced tricompartmental left knee osteoarthritis. The patient was suspected to have Paget’s disease and the diagnosis was confirmed using a bone scan (Fig. 1) and blood tests-Alkaline Phosphatase (ALP), C-Telopeptide (CTX), and Procollagen Type I N-terminal propeptide (P1NP).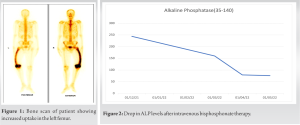 Under an endocrinologist’s care, the patient was treated with single dose intravenous bisphosphonate and was followed-up for 4 months to look for disease activity. When the reduction in pathological bone turnover was noted, which was assessed by evaluating serum ALP (Fig. 2), CTX, and P1NP levels along with significant relief in thigh pain relief, he was planned for a left TKA.
Under an endocrinologist’s care, the patient was treated with single dose intravenous bisphosphonate and was followed-up for 4 months to look for disease activity. When the reduction in pathological bone turnover was noted, which was assessed by evaluating serum ALP (Fig. 2), CTX, and P1NP levels along with significant relief in thigh pain relief, he was planned for a left TKA. 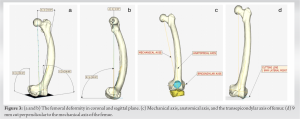 Due to the extreme bow of the femur in the coronal and sagittal plane (Fig. 3) and an overall 20° varus deformity of the knee joint, balancing the extension and flexion gaps during TKA would be challenging. As a standard intramedullary jig could not be used in view of an inaccurate measurement or a cortical breach, we designed a 3D-printed patient-specific distal femur jig (Supercraft3D, Bengaluru, India) that avoided intramedullary referencing. The entire lower limb morphology was studied using computed tomography scans and 3D bone modeling (Fig. 3). We considered the deformity as well as the mechanical axis of the femur and designed a jig referred from the distal-most femoral condyle at 90° angles to the sagittal and coronal plane (Fig. 4).
Due to the extreme bow of the femur in the coronal and sagittal plane (Fig. 3) and an overall 20° varus deformity of the knee joint, balancing the extension and flexion gaps during TKA would be challenging. As a standard intramedullary jig could not be used in view of an inaccurate measurement or a cortical breach, we designed a 3D-printed patient-specific distal femur jig (Supercraft3D, Bengaluru, India) that avoided intramedullary referencing. The entire lower limb morphology was studied using computed tomography scans and 3D bone modeling (Fig. 3). We considered the deformity as well as the mechanical axis of the femur and designed a jig referred from the distal-most femoral condyle at 90° angles to the sagittal and coronal plane (Fig. 4). 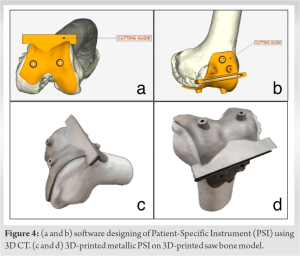 This custom jig (Fig. 5) allowed us to take accurately measure the entire femoral mechanical axis for an accurate parallel first distal femoral cut (extension gap) (Fig. 3d).
This custom jig (Fig. 5) allowed us to take accurately measure the entire femoral mechanical axis for an accurate parallel first distal femoral cut (extension gap) (Fig. 3d).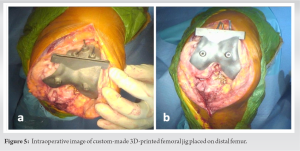 Following the distal femoral cut, a standard proximal tibial cut was performed using the tibial extramedullary guide. The extension gap was then measured and found to be well balanced. The femur was sized to two and the remaining femoral cuts performed. The gap balancing method was used to equalize the flexion gap and rotation of the femur (Fig. 6), achieving a stable well-balanced knee. We elected to use a semi-constrained implant to reduce the strain on the collateral ligaments due to the femoral deformity.
Following the distal femoral cut, a standard proximal tibial cut was performed using the tibial extramedullary guide. The extension gap was then measured and found to be well balanced. The femur was sized to two and the remaining femoral cuts performed. The gap balancing method was used to equalize the flexion gap and rotation of the femur (Fig. 6), achieving a stable well-balanced knee. We elected to use a semi-constrained implant to reduce the strain on the collateral ligaments due to the femoral deformity. The time taken for completion of the surgery was comparable to the conventional primary TKAs we perform. Post-operative X-rays were satisfactory (Fig. 7 and 8). The patient was mobilized, and rehab was conducted as a standard TKA. At 6-month follow-up he was mobilizing without any walking aids with excellent function and pain relief. He is followed-up for Paget’s disease activity with a serial evaluation of biochemical markers as per current guidelines [5].
The time taken for completion of the surgery was comparable to the conventional primary TKAs we perform. Post-operative X-rays were satisfactory (Fig. 7 and 8). The patient was mobilized, and rehab was conducted as a standard TKA. At 6-month follow-up he was mobilizing without any walking aids with excellent function and pain relief. He is followed-up for Paget’s disease activity with a serial evaluation of biochemical markers as per current guidelines [5].
Careful pre-operative planning is the key for successful outcome in cases of complex lower limb deformity. In this case, the use of a conventional intramedullary femoral jig is impossible as the medullary canal cannot accommodate the instrumentation [2]. TKA with simultaneous corrective osteotomy and intramedullary nailing or blade plate fixation has been described for osteoarthritis with severe extra-articular deformity, but is technically challenging, and increases the number of surgeries and risk of complications [6, 7]. In recent times, newer options have become available to perform accurate distal femur cuts without an intramedullary jig such as navigated or robotic TKA or using a patient-specific instrumentation (PSI). It has been documented that robotic TKA takes a longer duration of surgery than a conventional TKA but more importantly, it has the added cost of the robotic instrumentation [8, 9]. PSI has been employed for some time and literature has reported shorter operative time and increased accuracy of component sizing and position in complex primary TKA [10]. An additional theoretical benefit to shorter surgical duration is lower risk of infection [11]. Mattei et al. in their review article had concluded that PSI is beneficial during TKA of patients with severe extra-articular deformities [12]. Pauzenberger et al. in 2019 had reported that TKA using PSI was superior to conventional TKA in achieving accurate alignment [10]. However, despite the different operative methods and alignment philosophy, post-operative outcomes and patient-reported outcomes remain to be similar in all groups [13]. In the past, PSI has been expensive especially when employed for all the cutting jigs involved in a TKA. In our case, we used only one 3D-printed PSI jig for the distal femoral cut. With this one jig, we were able to perform the remaining TKA in a standard fashion to achieve a well-balanced knee in a complex primary TKA situation. 3D printing has made jig preparation simple, easily accessible, and inexpensive. Here the 3D-printed femoral jig provided a simple solution to the abnormal femoral anatomy without excessive cost or the need for all the jigs to be printed. Not using the intramedullary guide reduced the possibility of a cortical breach in the femoral bone and reduced intraoperative bleeding which may have been more pronounced in a bone with such pathology. Robotic TKA increases that the total hospital expense per patient due to increases intraoperative duration, use of additional instrumentation, and the cost of procuring the robot [14]. Such cost-effective 3D-printed custom jigs should be considered in complex TKA, especially in centers where navigation and robotic TKA is unavailable and where rising healthcare costs burden the patient.
Severe extra-articular deformity secondary to metabolic bone pathology like Paget’s disease, along with osteoarthritis of knee joint complicates a primary TKA. Options available for these cases are TKA with PSI, navigation TKA, or robotic TKA. The use of a 3D-printed custom patient-specific jig is an excellent cost-effective option. Due to severe correction of limb alignment, a semi-constrained implant is a safer option in such cases to support the surrounding soft-tissue structures. TKA has excellent outcomes in patients with secondary knee osteoarthritis due to monostotic femoral Paget’s disease. Diagnosis of Paget’s disease and control of the disease activity, along with careful pre-operative planning were key factors that helped in achieving a good post-operative outcome this case.
This case report provides surgeons with the possibility of an alternate option of using patient-specific instrumentation in a complex primary TKA especially in centers where robotic TKA or navigation TKA is not available.
References
- 1.Kravets I. Paget’s disease of bone: Diagnosis and treatment. Am J Med 2018;131:1298-303. [Google Scholar]
- 2.Popat R, Tsitskaris K, Millington S, Dawson-Bowling S, Hanna SA. Total knee arthroplasty in patients with Paget’s disease of bone: A systematic review. World J Orthop 2018;9:229-34. [Google Scholar]
- 3.Woods L, Maempel J, Beattie N, Roberts S, Ralston S. Outcomes following primary hip and knee arthroplasty in patients with Paget’s disease of the bone. Orthop Proc 2015;97-B:1-1. [Google Scholar]
- 4.Lee GC, Sanchez-Sotelo J, Berry DJ. Total knee arthroplasty in patients with Paget’s disease of bone at the knee. J Arthroplasty 2005;20:689-93. [Google Scholar]
- 5.Ralston SH, Corral‐Gudino L, Cooper C, Cooper C, Francis RM, Fraser WD, et al. Diagnosis and management of Paget’s disease of bone in adults: A clinical guideline. J Bone Miner Res 2019;34:e3657. [Google Scholar]
- 6.Incavo SJ, Kapadia C, Torney R. Use of an intramedullary nail for correction of femoral deformities combined with total knee arthroplasty: A technical tip. J Arthroplasty 2007; 22:133-5. [Google Scholar]
- 7.Lonner JH, Siliski JM, Lotke PA. Simultaneous femoral osteotomy and total knee arthroplasty for treatment of osteoarthritis associated with severe extra-articular deformity. J Bone Joint Surg Am 2000;82:342-8. [Google Scholar]
- 8.Kim YH, Yoon SH, Park JW. Does robotic-assisted TKA result in better outcome scores or long-term survivorship than conventional TKA? A randomized, controlled trial. Clin Orthop Relat Res 2020;478:26-75. [Google Scholar]
- 9.Nogalo C, Meena A, Abermann E, Fink C. Complications and downsides of the robotic total knee arthroplasty: A systematic review. Knee Surg Sports Traumatol Arthrosc 2023;31:736-50. [Google Scholar]
- 10.Pauzenberger L, Munz M, Brandl G, Frank JK, Heuberer PR, Laky B, et al. Patient-specific instrumentation improved three-dimensional accuracy in total knee arthroplasty: A comparative radiographic analysis of 1257 total knee arthroplasties. J Orthop Surg 2019;14:437. [Google Scholar]
- 11.Cheng H, Clymer JW, Chen BP, Sadeghirad B, Ferko NC, Cameron CG, et al. Prolonged operative duration is associated with complications: A systematic review and meta-analysis. J Surg Res 2018;229:134-44. [Google Scholar]
- 12.Mattei L, Pellegrino P, Calò M, Bistolfi A, Castoldi F. Patient specific instrumentation in total knee arthroplasty: A state of the art. Ann Transl Med 2016;4:126. [Google Scholar]
- 13.Lei K, Liu L, Chen X, Feng Q, Yang L, Guo L. Navigation and robotics improved alignment compared with PSI and conventional instrument, while clinical outcomes were similar in TKA: A network meta-analysis. Knee Surg Sports Traumatol Arthrosc 2022;30:721-33. [Google Scholar]
- 14.Fang CJ, Mazzocco JC, Sun DC, Shaker JM, Talmo CT, Mattingly DA, et al. Total knee arthroplasty hospital costs by time-driven activity-based costing: Robotic vs conventional. Arthroplasty Today 2021;13:43-7. [Google Scholar]






